
Abstract
Background: Spondylolysis defects detected by nuclear scintigraphy but not by plain radiographs represent early lesions. Functional outcome and eventual bony union of these defects are unknown.
Hypothesis: Defects with greater degree of healing shortly after treatment will proceed to full bony union and better long-term functional outcome.
Study Design: Longitudinal cohort study.
Methods: Forty young athletes with early detected spondylolysis (radiograph negative, nuclear scintigraphy positive) were divided into 3 stages of healing by computed tomography scan. Functional outcome was assessed 7 to 11 years later using the low back outcome score and other factors. Degree of bony healing was assessed in volunteers.
Results: Thirty-two of 40 subjects (80%) completed the survey. Twenty-nine of 32 (91%) had good or excellent low back outcome scores. None required spinal fusion, but 1 required partial diskectomy. Functional outcome did not differ based on initial computed tomography results. Radiographic follow-up was obtained in 11 volunteers. None of the 7 bilateral defects healed, and 3 of these progressed to grade 1 spondylolisthesis. All 4 unilateral defects healed fully with bone.
Conclusions: Most young athletes conservatively treated for early spondylolysis maintain good functional outcome up to 11 years later. Unilateral defects can undergo full bony healing but may take longer than 12 weeks. Bilateral defects may undergo further degeneration and slip with time.
Spondylolysis is a defect of the pars interarticularis3,10 and is a common cause of back pain in active adolescents.3,10,12 Spondylolysis in this population is often painful and believed to represent a stress fracture of the pars from repetitive extension activities.3,10 Conventionally, the diagnosis has been established by demonstrating the defect on plain lumbar radiographs including oblique views. However, radiographs are not very sensitive for detecting early spondylolysis1,2,9 and often do not detect defects seen on CT scans. 17
Advances in radiologic studies have increased the physician's ability to diagnose spondylolysis at earlier stages and to reveal it in better anatomical detail. Bone scans and single photon emission computed tomography (SPECT) scans have been shown to be sensitive to detecting active spondylolysis and have often detected lesions not seen on plain radiographs.1,2,9 Lesions that are found on bone or SPECT scans but not identified on radiographs are believed to be relatively early in the lytic process and to have a better ability for bony healing. 11 Although bone and SPECT scans are sensitive in detecting active lesions, they do not offer adequate anatomical detail of the lesion. Currently, CT scans with reverse gantry angle images offer the best anatomical detail of the spondylolysis defect. 9
To date, most anatomical and functional outcome studies of spondylolysis have used plain radiographs to establish the diagnosis.2,6,13,14 Therefore, most of our knowledge regarding anatomical and functional outcome of spondylolysis is on older lesions with less likelihood for bony healing. Also, although the short-term results of conservatively treated symptomatic spondylolysis in adolescents have been promising,2,4,14,15 the long-term functional outcome has not been well studied. To the authors’ knowledge, no studies have used a validated functional low back survey to assess outcome after spondylolysis in active adolescents. The purpose of the present study was to evaluate the functional outcome and anatomical appearance on CT scans of conservatively treated spondylolysis in young athletes 7 to 11 years after early diagnosis.
Methods
The study population consisted of 40 subjects from a previous report 4 described by the following criteria: (1) age ≤ 20 years (range, 12-20 years), back pain worsened during extension, and involved in athletics (Table 1) at time of diagnosis; (2) initial radiographs with oblique views were normal, but either planar bone scan or SPECT scan showed active spondylolysis; and (3) CT scan with reverse gantry angle images was done 8 to 12 weeks after diagnosis. Treatment consisted of nonrigid lumbar bracing 23 hours per day, and a flexion-only trunk-strengthening program was started after 2 to 4 weeks of relative rest. Subjects with continued back pain by 4-week follow-up were placed in a rigid lumbar brace (2 of 40 subjects; 5%). At 6 to 8 weeks, the trunk stabilization program was advanced and a functional progression program prescribed. Subjects were allowed to return to sports wearing a nonrigid brace by 8 to 12 weeks if they were (1) pain free at rest, (2) pain free in hyperextension without a brace, and (3) pain free during their specific sporting activity with a brace. The use of braces was weaned over several weeks, with brace use during sporting activities being the last to go. All 40 subjects improved with this treatment and returned to their prior levels of athletics. Despite apparent early detection, athletes could be divided into 3 groups based on their initial CT scan findings: in group A, defects showed no evidence of new bone formation or healing (18 athletes); in group B, defects seemed to be in the process of healing with the potential for eventual bony union (16 athletes); and group C showed incomplete pars defects (6 athletes).
Sports Activity of Subjects at Time of Diagnosis a
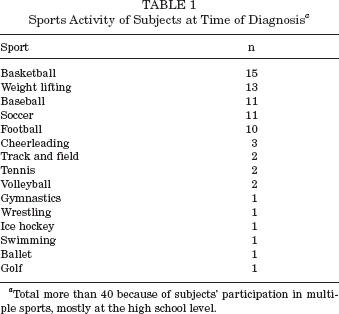
Total more than 40 because of subjects’ participation in multiple sports, mostly at the high school level.
Between November 2001 and May 2002, subjects were surveyed by telephone 7 to 11 years after diagnosis. The 10-minute survey consisted of calculating the low back outcome score (LBOS),7,8 determining whether interim low back surgery had been needed, and asking for a subjective assessment of the impact their low back function has had on employment and recreation choices. One investigator (SFM), who was blinded to the subjects’ initial CT findings, conducted all surveys. From this information, the functional outcome of the population as a whole was described. Then, the LBOS results of groups A, B, and C were compared by 95% confidence interval and t test analysis for differences in functional outcome. Using a power of 0.80 to detect a clinically important difference of 10 points on the LBOS would have required at least 19 subjects per group.
On a volunteer basis and free of charge, subjects underwent a follow-up limited CT scan with reverse gantry angle images to evaluate their backs for long-term bony healing. Volunteers also underwent a single lateral radiograph to assess for development of spondylolisthesis. One investigator (KS), who was blinded to the subjects’ LBOS and survey results, interpreted all radiographic studies.
Verbal consent was obtained before the phone survey, and written informed consent was obtained before follow- up radiologic studies. The Institutional Review Board at Children's Hospital Medical Center of Akron approved this study.
Results
Functional Outcome
Thirty-two of the 40 subjects (80%), with an average follow-up interval of 9 years (range, 7-11 years), completed the survey. Eight had relocated and could not be reached. There were 23 men and 9 women. The average age at follow-up was 24 years (range, 21-28 years), and all subjects were still active in a variety of sports (Table 2). The mean LBOS was 67.5 ± 9 (maximum score, 75), and 29 subjects (91%) had good to excellent results based on established scoring cutoffs (excellent, 65-75; good, 50-64; fair, 30-49; poor, 0-29). The 3 subjects with fair results were all from group A and had bilateral defects. Only 2 (6%) reported that their backs had influenced their choices of employment. Seven (22%) reported that their backs had influenced their choices of recreational activity (usually choice of certain weight-lifting techniques such as squat press). Twenty-nine (91%) had not visited a doctor, chiropractor, or physical therapist for their backs since the initial treatment. The other 9% only rarely sought medical help for their backs. No one required spinal fusion, but 1 subject required partial diskectomy for an extruded disk below the level of spondylolysis. Of the 32 subjects surveyed, there were 12 in group A (37%), 14 in group B (44%), and 6 in group C (19%). There was no statistical difference in functional outcome based on LBOS results between the 3 groups (P = .09) (Table 3).
Sports Activity of Subjects at Time of Follow-up a
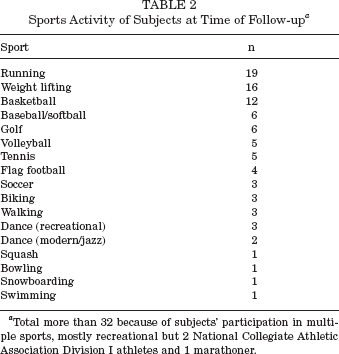
Total more than 32 because of subjects’ participation in multiple sports, mostly recreational but 2 National Collegiate Athletic Association Division I athletes and 1 marathoner.
Difference in Low Back Outcome Score (LBOS) Based on Degree of Defect Healing Seen on Initial CT Scan a
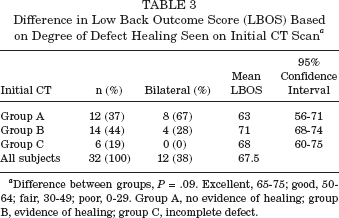
Difference between groups, P = .09. Excellent, 65-75; good, 50-64; fair, 30-49; poor, 0-29. Group A, no evidence of healing; group B, evidence of healing; group C, incomplete defect.
Anatomical Outcome
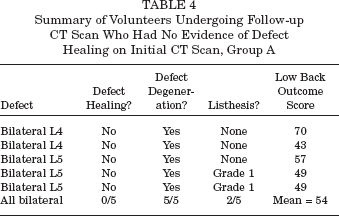
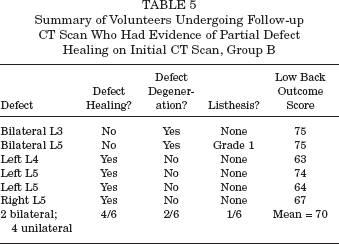
Follow-up radiographic studies were obtained in 11 of the 32 subjects (34%) (Tables 4 and 5). There were 5 athletes from group A, 6 athletes from group B, and none from group C. Follow-up CT scans revealed that no bilateral defects healed, regardless of anatomical appearance on initial CT scans. Bilateral defects showed signs of degeneration and fragmentation (Figure 1). Facet joints of some bilateral defects also showed changes of hypertrophic bone spurring. Lateral radiographs revealed 3 of 7 (43%) bilateral lesions progressed to a grade 1 slip. All 4 unilateral defects healed fully with bone, did not have facet joint changes, and did not develop slips (Figure 2).
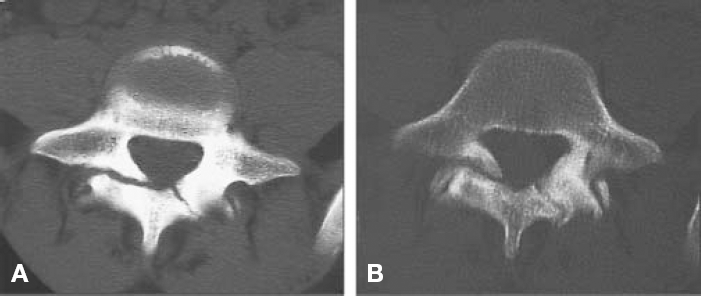
A, initial CT scan of bilateral L5 defects with marginal sclerosis (group A); B, a CT scan of the same defects 11 years later showing increased fragmentation and mild spurring.
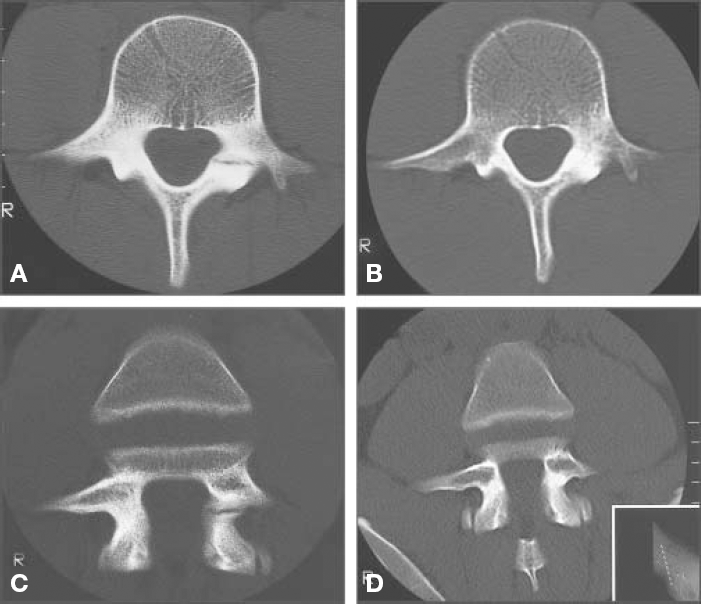
A, initial CT scan of left L4 defect with signs of healing (group B); B, a CT scan of the same defect 7 years later showing complete bony healing; C, initial reverse gantry CT scan of the same defect; D, reverse gantry CT scan 7 years later showing complete bony healing.
Summary of Volunteers Undergoing Follow-up CT Scan Who Had No Evidence of Defect Healing on Initial CT Scan, Group A
Summary of Volunteers Undergoing Follow-up CT Scan Who Had Evidence of Partial Defect Healing on Initial CT Scan, Group B
Discussion
Functional Outcome
Our results show that most adolescent athletes diagnosed early in the lytic process of painful spondylolysis and treated with nonsurgical management do well clinically up to 11 years later. The majority (91%) had good or excellent function on the LBOS. Also, none of those surveyed needed more than rare medical or manipulative treatment for their backs. Few reported that their backs had any influence on either employment or recreational activities. None of the athletes we surveyed had required lumbar fusion surgery at the time of follow-up. It is important that “diagnosed early in the lytic process” means that the defect was detectable by bone scan but not by plain radiographs at the initial evaluation.
Sys et al provide the only other outcome assessment of early (normal radiograph but positive bone scan) and conservatively treated spondylolysis in young athletes. They found “good” or “excellent” outcomes in 93% at a mean of 13 months. 15 Our study shows that a similar number do well at a mean of 9 years. Previous studies of adolescent spondylolysis included older defects detected by radiographs and subjects who required operative treatment shortly after initial diagnosis yet still found favorable outcomes in 87% to 96% at a mean follow-up of 2 to 4 years.2,14
Based on results of this study, evidence of defect healing on CT scans done shortly after initial diagnosis was not predictive of functional outcome after conservative treatment. However, subjects with no evidence of defect healing on initial CT scans (group A) tended toward a worse functional outcome than subjects with evidence of healing (groups B and C). In addition, all 3 subjects with less than good outcomes on the LBOS were from group A, and of these 3, 2 went on to spondylolisthesis. Admittedly, this study was limited by the number of subjects in the previous study, 4 and the sample size was too small to exclude the chance of a statistical difference. Therefore, a larger study population may still find a clinically important difference in outcome 7 to 11 years after treatment.
Although our study shows favorable outcomes of adolescents with early detected and conservatively treated spondylolysis up to 11 years after diagnosis, whether they will continue to do well beyond their mid-20s is not known. One 26-year-old patient from our study had back pain with radiating symptoms at the time of the survey and was later found to have an extruded disk on MRI. This patient had relief of symptoms after partial diskectomy. Persons with spondylolysis on plain radiographs have more severe disk degeneration below the level of the defect than the general population, starting at the age of 25 years.5,16 Therefore, persons with persistent defects may have more deterioration of function due to faster disk degeneration after age 25 than persons without defects.
Anatomical Outcome
The CT scans done shortly after initial diagnosis showed defects in various stages of healing. Group A showed no evidence of healing and was presumed to represent a nonunion. Group B showed evidence of calcification, but a full defect was still visible and was presumed to represent early defect healing. Group C showed the defect already partially bridged by solid bone and was presumed to represent a later stage of healing. Whether the latter 2 groups would continue to full bony healing was uncertain. As expected, follow-up CT scans showed that no defects from group A had healed, and in fact, all defects showed evidence of degeneration. Surprisingly, despite favorable response to conservative treatment and early evidence of calcification, some defects from group B still progressed to full lytic defects with evidence of degeneration.
From our results, the bilaterality of a defect is more important than the stage of apparent healing on early CT scans for predicting bony union. All 4 unilateral defects went on to bony union, whereas all 7 bilateral defects did not. Likewise, 3 of 7 bilateral defects progressed to grade 1 slip, and all showed defect degeneration, which is clearly not desirable for patients in their 20s. Similarly, Blanda et al found that most defects that heal were unilateral. 2 Yamane et al also reported bony union of several defects on CT scans but did not distinguish between unilateral and bilateral defects. 18 Sys et al found all 11 unilateral defects healed compared to 5 of 17 bilateral defects. 15 It is likely that the vertebra with a unilateral spondylolysis has more stability and less motion across the defect, which allows greater possibility for bony fusion. Stability can be inferred by the continued healing of unilateral defects in our study beyond 12 weeks of treatment and without prolonged activity limitation. On the other hand, the relatively greater motion across a bilateral defect reduces its chances of bony fusion even years after treatment. Increased motion is supported by the degeneration and fragmentation of bilateral defects seen years later. It would be interesting to know the long-term functional outcome of athletes with persistent bilateral defects versus those who attained bony union. Because of the limited number of follow-up CT scans, we could not perform this analysis.
Another point should be made from our data. An athlete's defect was classified as unilateral or bilateral by initial CT scan appearance. A few bone scans showed unilateral activity, but the corresponding CT scan showed bilateral defects. It was assumed that the bone scan activity represented a recent defect, whereas the contralateral CT defect was older. Sys et al described a similar finding in which asymmetric activity on bone scan was termed “pseudobilateral.” 15 In their study, none of the 8 pseudobilateral lesions healed bilaterally, but functional outcomes did not differ at a mean of 13 months. It is possible that defects with asymmetrical onset may have different healing potential, and future studies should take this into account.
There are limitations to our study. As stated above, the sample size is small, and a statistical difference in the effect of early defect healing on LBOS results at 7- to 11- year follow-up cannot be excluded. Also, any survey has potential recall bias. At the time of survey, subjects may be more likely to downplay low back symptoms experienced in the past. However, the fact that less than 10% required interim medical treatment leads us to believe that most truly were doing well. In addition, the small number of follow-up CT scans may not be definitive of a larger population. That is to say that there may be some bilateral lesions that do go on to fuse and some unilateral lesions that do not. Lastly, the volunteer nature of the follow-up CT evaluation could also bias toward subjects with more low back symptoms. Less symptomatic subjects may be less likely to volunteer. Thus, less symptomatic subjects with bilateral defects could have less degeneration or even have complete fusion but would not have been evaluated.
In conclusion, most adolescent athletes nonsurgically treated for symptomatic spondylolysis maintain good functional outcome up to 11 years later. Unilateral defects are more likely to undergo full bony healing but may take longer than 12 weeks to appreciate on CT scan. Persistent bilateral defects undergo further degeneration with time. Whether bony union of a defect will influence functional outcome beyond 11 years requires further study.