
Abstract
Background
Revision anterior cruciate ligament reconstruction requires flexibility and variability in treatment options. This study analyzed the functional outcomes and graft stability of 48 consecutive revision anterior cruciate ligament reconstructions using previously unharvested ipsilateral autografts.
Hypothesis
Using previously unharvested ipsilateral autografts will achieve similar outcomes to other graft choices in revising previously failed anterior cruciate ligament reconstructions.
Study Design
Prospective nonrandomized clinical trial.
Methods
Forty-eight patients (48 operations) were observed for 2 to 13 years (mean, 90 months). All agreed to have revision reconstruction with ipsilateral autografts. The details of the technique varied according to the original graft choice and the abnormality encountered. Concomitant procedures were necessary in 40 (84%) of 48 knees. Twenty-three patients (48%) had revision reconstruction with previously unharvested ipsilateral autogenous hamstring tendons. Ten (21%) were 2-stranded grafts, and 13 (27%) were 4-stranded (quadrupled) autografts. Twenty-five patients (52%) had revision reconstruction with previously unharvested ipsilateral patellar tendon autografts, 6 (12%) using the 2-incision rear-entry method and 19 (40%) using the single-incision technique.
Results
Results were evaluated with Lysholm and Gillquist scores and International Knee Documentation Committee ratings, including KT-2000 arthrometer examinations. Seventy-three percent of the patients had International Knee Documentation Committee normal (A) or nearly normal (B) knees (42% of the patients had A knees and 42% had B knees). Twelve percent of patients had C knees, and 4% had a D rating. Sixty-seven percent of the knees had a KT-2000 arthrometer side-to-side difference of 3 mm or less, and an additional 21% of the knees had a side-to-side difference of 3 to 5 mm; therefore, 94% of the grafts were functional or partially functional. Six percent of grafts had more than 5 mm of laxity and were considered failures.
Conclusions
Previously unharvested ipsilateral autografts proved reliable in improving function and stability in revision anterior cruciate ligament reconstruction. However, outcomes were less favorable with revision reconstructions than with primary reconstructions.
Primary ACL reconstructions have a reported success rate of restoring stability in 90% to 97% of knees.1, 4, 9, 18–20, 29, 30 As reported by Owings and Kozak, in 1996 more than 102 000 ACL reconstructions were reported annually by surgical facilities in the United States alone. 27 The number of primary ACL reconstructions is expected to increase, and with a failure rate of primary stabilizations of up to 10%, the necessity for stabilizing the knee with a failed reconstruction will continue to increasingly challenge surgeons.1, 4, 18–20 Primary graft failure has been attributed to errors in surgical technique, including but not limited to anterior placement of femoral and tibial tunnels,2, 8, 12, 15 inadequate notchplasty5, 31 and graft fixation,15, 16 and poor technique in selection and harvest of the graft. 6
Graft choices for revision ACL reconstruction include ipsilateral and contralateral bone–patellar tendon–bone autografts, including reharvesting of the ipsilateral bone-tendon-bone graft,3, 14, 26, 29 semitendinosus-gracilis hamstring autografts, 33 quadriceps tendon autografts, 34 and bone–patellar tendon–bone or Achilles tendon allografts.13, 23 An advantage of ipsilateral grafts is the absence of surgical trauma to the contralateral knee. 14 Allografts also avoid surgical trauma to the contralateral knee; however, using ipsilateral autografts prevents the risk of disease transmission that is found with allografts. 14
High success rates3, 26 and alarmingly high failure rates14, 22 have been reported with reharvest of the ipsilateral bone–patellar tendon–bone graft for revision ACL reconstruction. High failure rates have also been reported for allograft bone–patellar tendon–bone revision reconstructions. 23
Each case of revision ACL reconstruction surgery is unique and requires an individual approach involving extensive preoperative evaluation of the patient's physical demands, socioeconomic situation, pathologic state, and available graft options. The graft selection must be a reasonable option not only for the patient but for the surgeon as well. Ideally, the surgeon can avoid surgical trauma to the contralateral knee, yet improve on the reported failure rates with reharvested ipsilateral bone–patellar tendon–bone autografts and allografts.
The purpose of this prospective study was to determine the functional outcome and arthrometer-measured success rate in arthroscopically assisted revision ACL reconstructions using previously unharvested ipsilateral knee autografts consisting of either semitendinosus-gracilis tendons or bone–patellar tendon–bone grafts. No reharvest of bone–patellar tendon–bone was done. The previously reported success rate of these 2 ipsilateral graft constructs by this author for ACL reconstruction was 92%. 24
Materials and Methods
Between August 1989 and December 2000, 146 patients who had a failed ACL reconstruction procedure for knee stabilizion were examined. Fifty-five patients had primary extra-articular reconstructions with failure of knee stability, requiring an intra-articular revision reconstruction, and were not included in this study. Thirty-seven patients chose to modify their activities and avoid further surgery. Four patients presented with bilateral cruciate ligament reconstructions and were excluded from inclusion in the study group, as the contralateral knee could not be considered as an accurate baseline in arthrometer, range of motion, and single-legged-hop tests.
Study Group
The study group included the remaining 50 patients. After an institutionally approved informed consent was obtained, the patients were entered into the study to revise their failed ACL reconstructions with ipsilateral, previously unharvested grafts. Two patients were lost to follow-up. One died of lymphoma 23 months postoperatively, and one died of a gunshot wound 24 months postoperatively. The remaining 48 patients had a follow-up of 2 to 13 years (mean, 90 months). Two patients were included in the author's previous studies.24, 25
Twenty-eight operations were done in male patients and 20 in female patients. The mean age at surgery was 33 years (range, 13–57 years). All 48 patients had reinjured the knee during a sports activity. Ten patients (21%) had modified their sports activities after their primary ACL reconstructions, unable to “trust” their knees—3 (6%) feeling their knees were unstable and 7 (15%) feeling their knees were weak. All 10 patients had grade II or higher positive Lachman examination scores, and all 10 had MRI studies documenting absent or torn anterior cruciate grafts. Thirty-eight patients (79%) had a clear history of an acute new trauma to the reconstructed knee, followed by the new onset of instability. The mean time from the primary ACL reconstruction to the arthroscopically assisted revision ACL reconstruction was 60 months (range, 7-276 months).
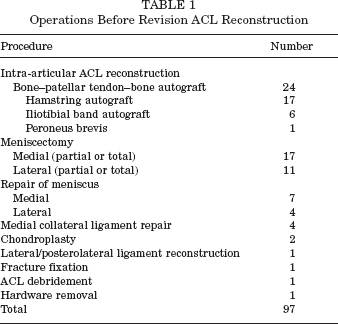
The 48 patients in this study had 70 operations, including 97 procedures before the revision operation (Table 1).
Operations Before Revision ACL Reconstruction
Operative Technique
At the time of the index operation, the knee was examined under anesthesia for associated instability. Then, an arthroscopic examination was done, and any associated injuries were treated.
Depending on the graft choice for the failed ACL reconstruction, the available previously unharvested alternative graft was used for the revision surgery. Six patients had primary failed reconstructions with iliotibial band grafts, and 1 patient had a failed reconstruction with a peroneus brevis tendon graft. With both the previously unharvested patellar tendon and hamstring tendon available, 6 of the 7 patients were revised with patellar tendons. A 28-year-old woman with grade III patellar chondromalacia and the failed peroneus brevis graft had a revision with hamstring tendons. Two-incision and endoscopic techniques were used, and decisions were based on tunnel widening and previous tunnel placement. The quality of the tunnel bone and graft quality had to be assessed in planning fixation options. The same surgeon (D.B.O.) did all the procedures.
Two-Incision Technique with a Semitendinosus-Gracilis Graft
Ten patients (10 operations) had revision ACL reconstructions using semitendinosus and gracilis 2-stranded ipsilateral autografts and the arthroscopically assisted rear-entry technique. 25 All 10 patients were male, with a mean age of 32 years (range, 17–40 years). All 10 patients had failure of patellar tendon grafts with what appeared arthroscopically to be correctly placed tunnels; however, femoral tunnel widening was encountered with loose interference screws. Thus, a new tunnel could be created with the rear-entry technique. Femoral tunnels were centered within 7 mm of the posterior notch cortex at the 1-o'clock or 11-o'clock position, and tibial tunnels were centered centrally 7 mm anterior to the posterior cruciate ligament. The rear-entry 2-incision technique required for new femoral tunnels necessitated longer hamstring grafts than could be achieved when the pes tendons were folded over and quadrupled. The 2-stranded gracilis and semitendinosus graft was doubly stapled to the lateral femoral cortex proximal to the cortical drill hole in the rear-entry technique.
Endoscopic Technique with Quadrupled Semitendinosus-Gracilis Grafts
Fifteen patients (15 operations) had revision ACL reconstructions using ipsilateral quadrupled semitendinosus and gracilis autografts. Ten of the 15 patients had failure of the patellar tendon graft secondary to anterior placement of the femoral tunnel. The remaining 5 patients had correct femoral tunnel placement and no appreciable tunnel widening.
The pes anserinus was identified through a 4-cm vertical incision, beginning 4 cm distal to the anteromedial tibial joint line (Figure 1). The semitendinosus and gracilis tendons were obtained proximally with an open-ended tendon stripper (Orthopedic Systems, Hayward, Calif), and they were dissected sharply and freed from the insertion on the tibia.
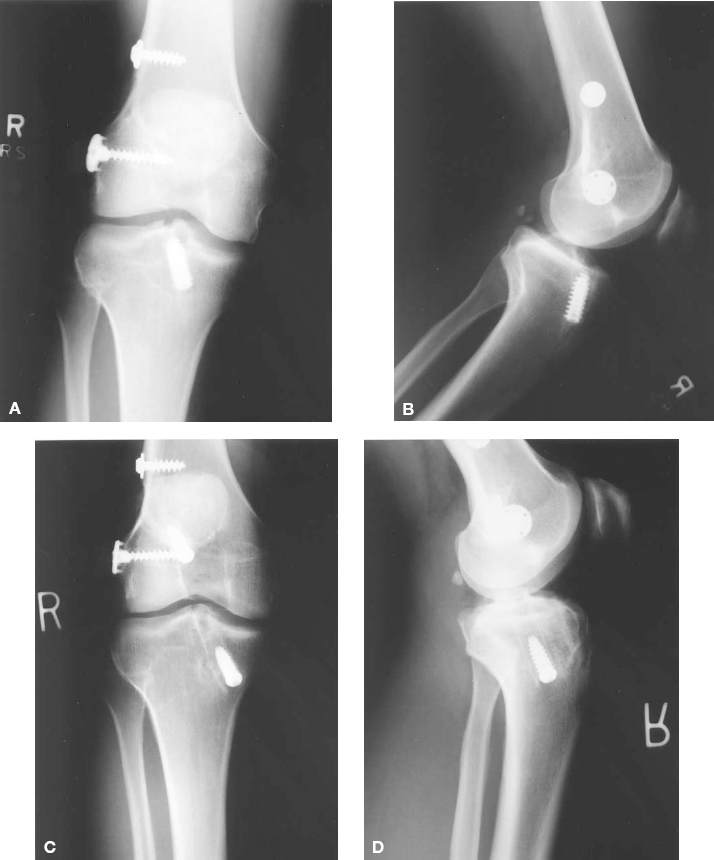
The endoscopic quadrupled semitendinosus-gracilis autograft secured with the RCI screws. A and B, the anteroposterior and lateral radiographs, respectively, of the right knee of a 30-year-old who had a patellar tendon ACL reconstruction and posterolateral reconstruction 7 years previously while involved in collegiate soccer. C and D, the anteroposterior and lateral radiographs, respectively, of the knee 6 years after the revision ACL reconstruction with quadrupled semitendinosus-gracilis grafts secured with RCI screws. The previously placed tibial interference screw required removal. The man continues to play competitive soccer, despite the mild increase in compartment space narrowing over the revision postoperative interval.
The tendons were doubled over a nonabsorbable 2-0 suture, and whipstitches were placed in the 4 free ends for traction. The proximal 2.5 cm of the quadrupled graft were sutured in whipstitch fashion, taking care to leave the 2-0 nonabsorbable doubling suture free for later pullout.
A generous arthroscopic notchplasty was done, and tibial and femoral endoscopic tunnels were made to match the diameter of the quadrupled graft, usually 8 mm but up to 10 mm in diameter. The lateral femoral cortex was penetrated from the endoscopic approach with a 6-mm-diameter drill. The quadrupled graft was pulled retrograde through the tibial tunnel and into the femoral tunnel via a Beath pin and the 2-0 nonabsorbable suture. The Beath pin was pulled through the anterolateral thigh to grasp the suture and pull tension on the graft.
With tension on the graft and the knee flexed more than 90°, a femoral interference screw of the same diameter as the femoral tunnel was placed over a parallel guide wire. Pretensioning of the graft was accomplished by moving the knee through 25 repetitions of flexion and extension; the grafts were then secured in the tibial tunnel with a similarly sized interference screw with distal tension on the graft and the knee in full extension. The nonabsorbable lead suture was then pulled out through the anterolateral thigh.
Eight patients, 5 men and 3 women, had fixation with the nonabsorbable RCI screws (DonJoy Orthopedics, Vista, Calif) (Figure 1). Seven patients, 4 women and 3 men, had interference fixation with absorbable Mitek screws as they became available (Mitek, Norwood, Mass) (Figure 2). The endoscopic quadrupled semitendinosus-gracilis autograft patients were a mean age of 32 years (range, 16–56 years).

The endoscopic quadrupled semitendinosus-gracilis autograft secured with absorbable screws. A and B, the anteroposterior and lateral radiographs, respectively, of the right knee of a 33-year-old who had a patellar tendon ACL reconstruction 53 months previously. C and D, the anteroposterior and lateral radiographs, respectively, of the knee 50 months after revision ACL reconstruction with quadrupled semitendinosus-gracilis grafts secured with absorbable screws using the endoscopic single-incision technique. The previously placed tibial interference screw required removal. The patient continues to play basketball and indoor soccer and has no interval degenerative changes seen on radiographs.
Two-Incision Technique with a Patellar Tendon Graft
Four patients had revision reconstruction using patellar tendon ipsilateral autograft and the 2-incision rear-entry technique with metal interference screws. 25 The 2 men and 2 women were a mean age of 34 years (range, 28–44 years). All 4 patients had femoral tunnel widening, and rear-entry reconstruction allowed creation of a new tunnel for interference screw fixation.
Single-Incision (Endoscopic) Technique with a Patellar Tendon Graft
Nineteen patients (19 operations) had revision ACL reconstruction using ipsilateral patellar tendon autograft and the endoscopic technique. 25 Ten of the patients had anterior or superior femoral tunnels that did not interfere with correct tunnel placement. Nine patients had correct tunnel placement, 6 of whom had no appreciable tunnel widening. Three patients with widening of the femoral tunnel required interference screws that had a diameter greater than 10 mm.
Nine patients, 7 women and 2 men, had fixation with nonabsorbable Mitek screws, and 10 patients, 6 men and 4 women, had fixation with absorbable Mitek interference screws. The endoscopic patellar tendon revision reconstruction patients were a mean age of 34 years (range, 13–57 years).
Concomitant Operations
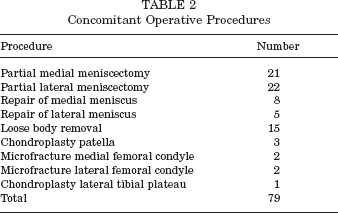
Forty (84%) of the patients had at least one additional injury in the ipsilateral knee. Concomitant with the revision ACL reconstruction, 8 medial and 5 lateral menisci were repaired, and 21 medial and 22 lateral partial meniscectomies were done (Table 2). Loose osteochondral bodies were removed from 15 knees, and 4 patients had femoral condyle microfracture procedures. Three patellar chondroplasties were done, and 1 patient had a chondroplasty of the lateral tibial plateau.
Concomitant Operative Procedures
Postoperative Regimen
All procedures were done in an outpatient setting. With the exception of the 4 microfracture patients who were kept nonweightbearing for 8 weeks, the postoperative regimen did not vary based on revision technique or concomitant operations. The patients were asked to begin immediate full weightbearing and were pushed through a full range of motion of the knee. Postoperative pain was managed with oral narcotics for up to 1 week.
Running was permitted at 3 months, but cutting, pivoting, and jumping were delayed until the fourth postoperative month. Competitive athletic activity was allowed 6 months postoperatively.
Isokinetic testing of the knee extensors and flexors was done with a dynamometer (LidoLinea, West Sacramento, Calif) at 18 weeks and at yearly intervals after the index procedure. Tests were performed at 60°/s, 180°/s, and 240°/s, and deficits were recorded at all of the levels tested.
Instrumented laxity testing was done with the KT-2000 arthrometer (MedMetric, San Diego, Calif) 18 weeks postoperatively and at yearly intervals after the operation. All arthrometer tests were administered by the same senior physical therapist at the same facility.
Postoperative orthopaedic evaluations were performed at 1, 2, 6, 12, and 18 weeks; at 6 months; and annually thereafter. Examinations included Lachman and pivot-shift tests, determination of associated instabilities and range of motion measurements, thigh circumference measurements, and 1-legged-hop tests beginning at 6 months. Extension was measured with a goniometer with the patient prone and the foot extended over the end of the rigid examination table. Flexion was measured on the same rigid table with the patient in the prone position, pulling the heel to the buttock. Measurements were compared to the contralateral knee. Normal extension was from 0° to 7° of hyperextension, and normal flexion was from 140° to 155°.
Radiographs were taken at 1 and 6 weeks and then on an annual basis. An anteroposterior standing radiograph was taken with the knee in full extension, and a lateral radiograph was taken with the knee in 40° of flexion. Baseline radiographs were taken within 3 months preoperatively, and progression of postoperative degenerative changes and cartilage space narrowing was determined and measured by the senior hospital radiologist.
At yearly intervals, function was evaluated according to the system of Lysholm and Gillquist 17 , as modified by Tegner and Lysholm 32 , and the International Knee Documentation Committee (IKDC),10, 11 as well as with the 1-legged-hop test for distance. 7
Statistical significance of the data was analyzed using the t test, analysis of variance, and the Kruskal-Wallis H test. 28 The α error was fixed at 5% (the traditional 95% confidence level) for power analysis, and the statistical power or β error was calculated.
Results
Fifty consecutive patients underwent revision ACL surgery, and adequate follow-up was available for 48. The mean time from initial surgery to revision surgery was 60 months (range, 7-276 months). Seventy-nine percent of the patients (38 of 48) experienced an isolated reinjury of the knee, whereas 10% had never trusted the knee postoperatively.
Failure of the Graft
On the basis of the KT-2000 arthrometer test results and pivot-shift examinations at the last follow-up, 35 of the 48 (73%) ligament revisions were functional, 10 (21%) were partially functional, and 3 (6%) had failed (Appendix 1, available in the online version of this article at www.ajsm.org/cgi/content/full/32/8/PE ADD PG NUMBER/DC1). A graft was considered functional if the knee demonstrated a side-to-side difference of 3 mm or less and had a negative pivot-shift examination result; a partially functional graft had a side-to-side difference of 3 to 5 mm and a trace pivot shift. A graft was considered a failure if the side-to-side difference was greater than 5 mm and the pivot shift was greater than a trace. The 3 graft failures in the patellar tendon endoscopic group with metal interference screw fixation do represent statistical significance (P < .05, Student t test, 95% confidence level); however, the failures occurred in the initial 4 revision reconstructions in the group and represent the steep learning curve. These same 3 failures also make the correlation between failure and length of follow-up statistically significant (P < .03) because they have the longest follow-up. If these 3 initial failures were excluded from the data for length of follow-up, with the numbers available, there would be no significant difference in graft failure based on length of follow-up.
Return to Preinjury Level of Activity
Thirty-six (75%) of the 48 patients in this revision study were able to return to athletic participation at a level equivalent to the level they had before the initial ACL tear. However, only 21 (44%) of the patients participated in sports that involved cutting, pivoting, and contact after the revision reconstruction.
Range of Motion
Fifteen patients (31%) lost terminal flexion of 2° to 25° (mean, 5°) as measured at final follow-up examination. Overall, 2 to 3 patients in each of the technique groups lost some terminal flexion.
Two patients (4%) lost terminal extension, one with a contracture of 3° and the other with a contracture of 5°.
Deficit in Strength of the Quadriceps and Hamstring Muscles
On isokinetic testing at all of the speeds evaluated, 27% of patients (13 patients) had a deficit of 10% or more in the strength of the quadriceps, and 10% of patients (5 patients) had a deficit of 20% or more (Appendix 2, available in the online version of this article at www.ajsm.org/cgi/content/full/32/8/PG O/DC1). Nine patients (19%) had hamstring deficits between 10% and 20%, and only 1 patient (2%) had a 20% deficit.
Serial data obtained at the 2-year follow-up examination and annually thereafter showed that the muscular deficits diminished with time. Although the trend shows greater hamstring deficits in the semitendinosus-gracilis graft revisions, and greater quadriceps deficits in the patellar tendon graft revisions, the findings were not statistically significant (P < .18, Student t test).
Subsequent Operative Procedures
Three patients (6%) have had 1 additional operation, and 2 patients (4%) have had 2 additional operations. Procedures in these additional operations included 3 partial medial meniscectomies, 2 partial lateral meniscectomies, 2 loose body removals, and a medial meniscal repair, a lateral femoral condyle chondroplasty, a microfracture of the medial tibial plateau, a tibial cyst excision, and a reclosure of a wound dehiscence.
Findings on Postoperative Radiographs
Thirty patients (63%) showed no evidence on radiographs of progressive degenerative changes in the knee (Appendix 3, available in the online version of this article at www.ajsm.org/cgi/content/full/32/8/PG NO/DC1). Thirteen patients (27%) were found to have mild changes seen on radiographs, and 5 patients (10%) had moderate progressive degenerative findings on radiographs.
Eight patients (17%), 4 with semitendinosus-gracilis grafts and 4 with bone–patellar tendon–bone grafts, had further tibial bone tunnel widening of up to 2 mm at a mean of 4 years postoperatively. The widening did not progress over the ensuing years of this study, and none of these knees had side-to-side differences on KT-2000 arthrometer testing of more than 2 mm. No progressive femoral tunnel widening was observed in these patients. There were no statistical differences among operative groups with regard to radiographic changes over time, and no significant relationship between meniscal repair, partial meniscectomy, or chondral injury and radiographic signs of progressive degeneration was found (β < .3).
Functional Testing
In this study, the IKDC10, 11 scale proved to be more discriminating than were knee scores assessed according to the system of Lysholm and Gillquist17, 32 with the reported findings.
Forty of the 48 patients (84%) had normal (IKDC A) or nearly normal (IKDC B) knee function (Appendix 4, available in the online version of this article at www.ajsm.org/cgi/content/full/32/8/PG O/DC1). Of the 20 patients with IKDC B ratings, points were lost for mild changes on radiographs, motion deficits, single-legged-hop deficits, and laxity on KT arthrometer testing. Six patients (12%) had IKDC C ratings, and 4 of the C ratings had 1-legged-hop tests less than 75%. Two C patients had moderate progressive degenerative findings on radiographs, 1 patient lacked full extension, and 1 patient had excessive laxity on KT arthrometer testing. Two patients (4%) had IKDC D ratings, 1 patient who lacked 25° of flexion and 1 patient who refused the 1-legged-hop test.
Functional testing was statistically significant (P < .05) for poorer outcomes in the group with endoscopic patellar tendon grafts with metal interference screw fixation, but as mentioned previously, 3 of the 4 initial patients in this study had revisions with this technique that failed. When these 3 initial failures are excluded, with the numbers available, there was no statistically significant difference in functional outcome (P = .4).
Discussion
In a previous study of 225 ACL reconstructions using similar techniques, 24 the author found that 92% of the knees were IKDC normal (A rating) or nearly normal (B rating) at a follow-up of 6 to 11 years. Sixty-four percent of the knees were in the normal category. The results of the present study involving revision ACL surgery demonstrated that 84% of the knees were in these 2 categories, with 42% having an A rating and 42% having a B rating. The graft failure rates in the 2 series were 6% in the current study and 7% in the prior study. The difference was not statistically significant (P < .1).
Preoperative planning can be extensive for the revision reconstruction. Previous tunnels and hardware must be addressed and available graft sources for reconstruction evaluated. Endoscopic and rear-entry guides must be available to the surgeon in the revision setting to deal with tunnel widening from previous surgery. A wide variety of interference screw diameters must be available for fixation of the graft in a compromised tunnel, and the surgeon should have the ability to bone graft the tunnel site. Standard screws and washers should also be available to tie sutures over a post, if necessary. The severely malpositioned tunnel in a failed reconstruction poses less of a problem, allowing for correct tunnel placement and standard fixation techniques. Although the results of previous studies reflect the difficulty of the revision procedure,21, 22, 33, 34 there has been a wider variety of grafts used than used in the present study. Previous studies have included use of contralateral bone–patellar tendon–bone autografts, reharvest of the ipsilateral bone–patellar tendon–bone autograft site, allograft bone–patellar tendon–bone, and semitendinosus-gracilis autografts.
Twenty (42%) of the 48 revision reconstructions had femoral tunnels from the primary reconstructions that were too anteriorly or superiorly placed. These revision reconstructions proceeded with less difficulty than did the 28 (58%) revision reconstructions with appropriate tunnel placement. Fourteen (29%) of the revision reconstructions required a 2-incision rear-entry technique to facilitate the creation of a new femoral tunnel. The holes left by the removal of interference screws in correctly placed but enlarged tunnels necessitated the use of new interference screws that were larger than 10 mm in diameter in 3 (6%) patients. No bone grafting of tunnels was done in this series of patients, and no patient had a 2-stage revision reconstruction procedure.
In a study of 55 revision reconstructions, Noyes and Barber-Westin had a graft failure rate of 24% (13 of 55 knees), 22 but 11 knees were reconstructed from reharvested bone–patellar tendon–bone graft sites, and 6 of these grafts failed. They found it necessary in 17 of the 55 knees to include secondary ligament reconstructions, while no patient in the present series was felt to have greater than grade II secondary ligament instability requiring reconstruction. Noyes and Barber-Westin currently recommend use of contralateral bone–patellar tendon–bone autograft for reconstructing the failed ACL. No patient in our series had reharvesting of a previously used patellar tendon or hamstring tendon. The recommendation for a revision reconstruction if both the bone–patellar tendon–bone and semitendinosus-gracilis ipsilateral grafts have been previously harvested would be to use contralateral bone–patellar tendon–bone autografts. 29
In Noyes and Barber-Westin's autogenous graft study, 88% (46 of 55 knees) were rated as improved by the patients. 22 In the present study, 84% (40 of 48) of the knees were rated on the IKDC scale as normal or nearly normal (A or B).
The patient numbers in the present study and in Noyes and Barber-Westin's study were similar, as their study included 1 patient with bilateral procedures and included 7 patients who had only extra-articular primary procedures with no previous attempt at an intra-articular reconstruction. Extra-articular reconstructions were not deemed as ACL reconstructions and were excluded from the present study. Bilateral procedures were also excluded from the present study, to obtain accurate data from the contralateral knee. Only 47 of the 55 patients in the Noyes and Barber-Westin study group would have been included in this study.
This study has confirmed that the results of revision ACL surgery are less favorable than are the results of primary ACL surgery. The findings were similar to those of other authors who used similar techniques and demonstrated that satisfactory results can be achieved over the long term with the use of previously unharvested ipsilateral autografts.
Although the data seem to suggest that semitendinosus-gracilis grafts provided better functional outcomes (P < .05) than did the patellar tendon grafts in these revision ACL reconstruction patients, the data more accurately reflect the steep learning curve in this revision series. Intraoperative decisions as to tunnel position and bone quality were made. Three of the initial 4 revision patients in this prospective study had previously failed ipsilateral hamstring tendon grafts that were placed using rear-entry femoral guides. Three of the initial ipsilateral patellar tendon revision grafts fixed with metallic interference screws that were placed with the endoscopic technique had failed. The failures were likely secondary to poor femoral fixation. If the study excluded these first 3 learning curve failures, there is no clear advantage of one technique over any other. It is clear that intraoperative decision making as to rear-entry versus endoscopic femoral tunnel techniques and adequate fixation with a variety of screw diameters and cortical staple fixation can determine the final stability and outcome.
The author's current recommendation for a previously failed ACL bone–patellar tendon–bone reconstruction would be to use an ipsilateral hamstring graft for the revision reconstruction. Conversely, if it has not been previously harvested, the ipsilateral bone–patellar tendon–bone graft is recommended.
Footnotes
Appendix
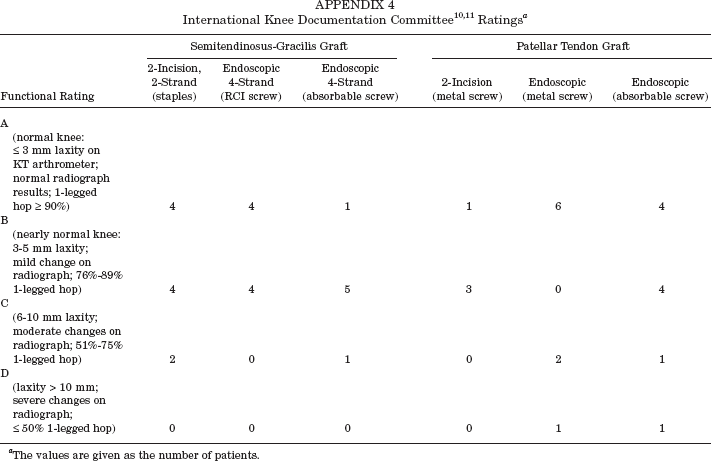
| Functional Rating | Semitendinosus-Gracilis Graft |
Patellar Tendon Graft |
||||
|---|---|---|---|---|---|---|
| 2-Incision, 2-Strand (staples) | Endoscopic 4-Strand (RCI screw) | Endoscopic 4-Strand (absorbable screw) | 2-Incision (metal screw) | Endoscopic (metal screw) | Endoscopic (absorbable screw) | |
| A | ||||||
| (normal knee: ≤ 3 mm laxity on KT arthrometer; normal radiograph results; 1-legged hop ≥ 90%) | 4 | 4 | 1 | 1 | 6 | 4 |
| B | ||||||
| (nearly normal knee: 3–5 mm laxity; mild change on radiograph; 76%-89% 1-legged hop) | 4 | 4 | 5 | 3 | 0 | 4 |
| C | ||||||
| (6–10 mm laxity; moderate changes on radiograph; 51%-75% 1-legged hop) | 2 | 0 | 1 | 0 | 2 | 1 |
| D | ||||||
| (laxity > 10 mm; severe changes on radiograph; ≤ 50% 1-legged hop) | 0 | 0 | 0 | 0 | 1 | 1 |
The values are given as the number of patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.