
Abstract
Background
The jerk test has been used as a diagnostic test of the posteroinferior instability of the shoulder. Pain may or may not be associated with posterior clunking during the jerk test.
Purpose
To evaluate the presence or absence of pain with the jerk test as a predictor of the success of nonoperative treatment for posteroinferior instability of the shoulder and to identify the pathologic lesion responsible for the pain in the jerk test.
Study Design
Retrospective review of prospectively collected data.
Methods
Eighty-one patients (89 shoulders) who had posteroinferior instability with a positive posterior clunk in their shoulders during the jerk test were nonoperatively treated. The patients were divided into 2 groups with respect to the presence of pain in the jerk test: the painless jerk group (54 shoulders) and the painful jerk group (35 shoulders). Response to the nonoperative treatment was evaluated after at least a 6-month rehabilitation program. Patients who did not respond to the rehabilitation underwent arthroscopic examination to identify any pathologic lesions.
Results
The painful jerk group had a higher failure rate with nonoperative treatment (P< .001). In the painless jerk group, 50 shoulders (93%) responded to the rehabilitation program after a mean of 4 months. Four shoulders (7%) were unresponsive to the rehabilitation. In the painful jerk group, 5 shoulders (16%) were successful with the rehabilitation, whereas the other 30 shoulders (84%) failed. All 34 shoulders that were unresponsive to the rehabilitation had a variable degree of posteroinferior labral lesions.
Conclusions
The jerk test is a hallmark for predicting the prognosis of nonoperative treatment for posteroinferior instability. Shoulders with symptomatic posteroinferior instability and a painful jerk test have posteroinferior labral lesions.
Nonoperative management incorporating a rehabilitation program has been the first line of choice in treating posteroinferior instability of the shoulder.5, 8, 9, 18, 19, 23 Surgical treatments have been considered only in patients who have not responded to an adequate trial of rehabilitation treatment and remain significantly disabled. 11 However, clinical results of rehabilitation treatments have not been well known.5, 8 Furthermore, there is no guideline for selecting patients for either nonoperative or operative treatments. Although nonoperative treatments are recommended as an initial treatment, there is a certain group of patients who do not respond to a rehabilitation program. 8 Early detection of these patients, who are unresponsive to nonoperative management, is of value to provide appropriate treatment.
The jerk test has been used as a diagnostic test for posteroinferior instability. Posterior clunking occurs while the humeral head is subluxated or reduced over the posterior glenoid rim and may or may not be accompanied with abrupt pain. 14 A selective attention mechanism of the body, pain usually signals impending or acute tissue damage and thus permits an individual to avoid harm.6, 24 To date, there has been no documentation explaining the source of shoulder pain, which is accompanied by clunking during the jerk test. The hypothesis of this study was that shoulders with a painful jerk test, compared to those with a painless jerk test, may have different pathologic lesions and thus may have different responses to nonoperative treatment. Therefore, the purposes of this study were to evaluate the presence or absence of pain with the jerk test as a predictor of the success of nonoperative treatment for posteroinferior instability of the shoulder and to identify the pathologic lesion responsible for the pain.
Materials and Methods
Patient Selection
We selected patients from our prospectively collected data registry in our institute from 1997 to 2001 to enroll in this retrospective analysis when the following criteria were met: (1) patients were treated for posteroinferior instability with a rehabilitation program as the initial treatment, (2) patients did not undergo a previous stabilization procedure, (3) patients were without a major traumatic episode, and (4) patients were compliant and finished at least a 6-month rehabilitation program.
Diagnosis of posteroinferior instability was based on the following clinical symptoms and physical signs: The shoulder was loose posteriorly and inferiorly with or without anterior laxity. The shoulder had dysfunction including pain, fatigue, loss of control during activity, or “dead arm” symptoms. Pain was elicited with sports activities involving a cross-body adduction position such as the follow-through phase of throwing or swimming. Daily activities such as carrying a heavy object or painting also produced shoulder pain. On physical examination, a palpable or audible posterior clunk during the jerk test was present. Posterior translation was increased in the posterior load-shift test. Inferior translation showed increased laxity with a greater than grade 1+ sulcus sign. 17 Anterior apprehension (the fulcrum test 4 ) and relocation tests were negative.
A major traumatic episode was defined when a patient sustained a traumatic event during sports or an accident that required immediate medical attention or termination of the same activity. Compliance of participation in regular rehabilitation exercises was measured by self-assessment. Patients recorded weekly the completion of the exercises, and a patient was considered compliant if he or she participated in more than 70% of them. Patients who did not finish 70% of the assigned exercises at every follow-up reinitiated them.
We excluded patients who had concomitant anterior instability with a documented Bankart lesion, traumatic unidirectional posterior instability, posteroinferior instability with dysplastic glenohumeral bony structures, noncompliance to the rehabilitation program, or an asymptomatic loose shoulder that did not need intensive nonoperative treatment. Patients with asymptomatic loose shoulders were those who have increased translation in posterior, inferior, and anterior directions without pain in daily and sports activities. These patients did not fit the criteria of instability and did not require intensive treatments. Sixty-eight patients were diagnosed with asymptomatic loose shoulders during the index period. For these patients, intermittent shoulder exercise was recommended to prevent a potential development of shoulder symptoms.
Ninety consecutive patients (98 shoulders) met selection criteria. Six patients were lost during the follow-up period. Of 84 patients, 14 were noncompliant for at least 1 set of exercises. After repeated exercise, 11 finished the assigned program and 3 patients remained noncompliant. Therefore, 89 shoulders in 81 patients were included in this study. The patients were divided into 2 groups according to the findings of the jerk test: a painless jerk group and a painful jerk group. The Institutional Review Board of our center approved the study, and each patient signed a detailed informed-consent form.
The Jerk Test
The jerk test was performed by the senior author with all patients in a sitting position. While stabilizing the patient's scapula with one hand and holding the affected arm at 90° abduction and internal rotation, the examiner grasps the elbow and axially loads the humerus in a proximal direction. The arm is moved horizontally across the body. A positive result is indicated by a sudden clunk as the humeral head slides off the back of the glenoid. When the arm is returned to the original position, a second jerk may be observed, that of the humeral head returning to the glenoid3, 14 (Figure 1). The painless jerk group included patients with posterior clunking that did not evoke any pain, whereas the painful jerk group included patients who showed abrupt pain in concurrence with posterior clunking.
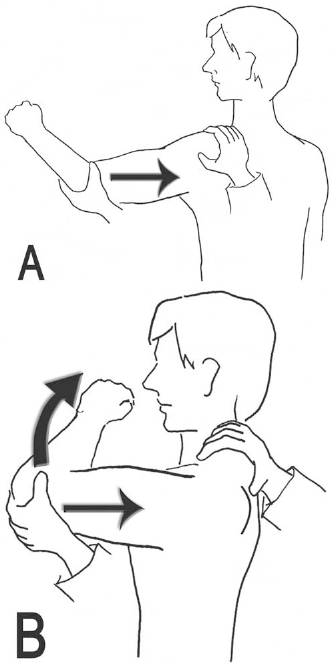
The jerk test. A, axial force is applied on the arm in 90° abduction and internal rotation; B, the arm is horizontally adducted while maintaining the axial load.
Nonoperative Treatment
All patients were initially treated nonoperatively with a rehabilitation program. 5 Any provocative motion or activity was prohibited until the complete rehabilitation was finished. Nonsteroidal anti-inflammatory medication was used when shoulder pain was severe enough to prevent rehabilitation exercise. Rehabilitation focused on strengthening of the rotator cuff muscle, posterior deltoid, and scapular stabilizers. Initially, internal and external rotation strengthening with the arm at the side was practiced for 3 weeks using different-sized rubber bands. During this time, external rotation was emphasized. Internal rotation strengthening exercise was also performed to balance the muscle couples. Then, forward elevation exercise in the scapular plane was performed. Rotational exercise with the arm in 90° of elevation was added. Strengthening exercises included both concentric and eccentric exercises. Resistance of the rubber band was slowly increased according to the patient's progress. Diagonal strengthening exercises were followed after 6 weeks. Free weights were used to increase resistance exercise in scaption, external rotation in varying degrees of shoulder abduction, and horizontal abduction. In athletes, isokinetic exercises were added in the supervised exercise program. More vigorous strengthening exercises were initiated according to the patient's progress.
Patient Evaluation
After completion of the rehabilitation program, the patients were evaluated using 2 subjective measurement tools (the pain 22 and function10, 11 visual analog scales) and 3 objective measurement tools (the Rowe score, 21 UCLA scale, 7 and modified American Shoulder and Elbow Surgeons [ASES] 20 scores). The jerk test was repeated and evaluated for pain, and the results were compared between the 2 groups. Failure of the nonoperative treatment occurred when the patients showed the following conditions: (1) persistence of previous shoulder pain or discomfort, (2) shoulder function less than 80% of the previous level, and (3) a fair or poor Rowe score. Subjective measurement of shoulder function was evaluated using a modified method from Kim et al.10, 11 Using the visual analog scale, each patient was asked to evaluate the preoperative and postoperative function of their affected shoulder as a percentage of its preinjury level. Return to activity was divided into 5 grades. Grade 0 represented no limitation of sports activities and a complete return to the patient's prior job (100% of preinjury level). Grade I represented mild limitation in performing daily activities and returning to a previous job (90% of preinjury level or greater). Grade II was rated when the patient had moderate restriction on performing the resumed sports activities or job (80% of preinjury level or greater). Grade III represented severe limitation (70% of preinjury level or greater). Grade IV indicated very severe limitation or an inability to return to prior sports activities or job (less than 70% of preinjury level). Grades 0, I, and II were classified as satisfactory returns, whereas grades III and IV were classified as unsatisfactory returns.
Before the nonoperative treatment, an MRI arthrogram was performed on all patients to evaluate any intra-articular lesions. A labral lesion in the MRI arthrogram was classified according to Kim et al.11, 13 For patients who did not respond to the nonoperative treatment, an arthroscopic examination was performed. The labral lesion in the arthroscopic evaluation was also classified according to Kim et al11, 13; the surgical procedure has been described in our previous articles.11–13 The basic principle involves recreation of the labral height by completely releasing the posteroinferior labrum from the glenoid and reattaching it on the surface of glenoid, as well as restoration of the ligament tension by superior shift of the posteroinferior and anteroinferior capsule and rotator interval closure.
Statistical Analyses
The Wilcoxon signed rank test was performed to evaluate the differences in preoperative and postoperative pain, function, and shoulder scores. To compare the measurements between the 2 groups, a Mann-Whitney U test was performed. Failure of the rehabilitation treatment was compared between the 2 groups using the χ2 test. The SPSS program (SPSS Science Inc, Chicago, Ill) was used for all analyses, with the α level set at .05.
Results
Patient Demographics
The painless jerk group included 48 patients (54 shoulders). The mean age was 24 years (range, 19–31 years). There were 31 male and 17 female patients. The predominant symptoms were vague discomfort after daily or sports activities and mild pain after exercise or heavy weight lifting. The jerk test demonstrated posterior clunking without pain. The painful jerk group included 33 patients (35 shoulders). The mean age was 25 years (range, 18–29 years). Twenty-six patients were male and 7 were female. Of 35 shoulders, 6 shoulders (6 patients) had recurrent pain after previously successful nonoperative treatment. The predominant symptoms were pain during daily activities and looseness of the shoulder during sporting activities. The jerk test elicited a painful posterior clunk. Initial parameters, including age, sex, shoulder pain, function, and shoulder scores, were similar in both groups (Mann-Whitney U test, P > .05). Twelve patients in the painless group and 11 in the painful group were participating in sports such as swimming, ballet, baseball, and golf. There was no difference in ligamentous laxity in terms of the sulcus sign between the 2 groups (P > .05) (Table 1). All other demographic data are listed in Table 1.
Demographic Data a
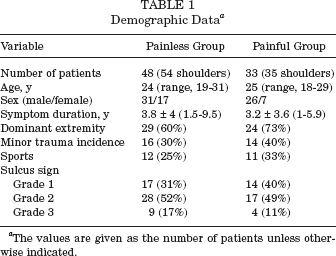
The values are given as the number of patients unless otherwise indicated.
MRI Arthrogram Findings and Validity of the Painful Jerk Test
According to the classification of Kim et al,11, 13 the painless jerk group had labral lesions in 3 shoulders (type I in 1 and type III in 2 shoulders), whereas the painful jerk group showed labral lesions in 26 shoulders (type I in 9, type II in 6, and type III in 11 shoulders).
Based on the MRI arthrogram findings, the sensitivity of the painful jerk test to diagnose posteroinferior labral lesions was 89.7%, specificity was 85%, positive predictive value was 72.2%, and negative predictive value was 94.4%.
Response to the Rehabilitation
The painful jerk group had a higher failure rate with rehabilitation treatment (χ2, P < .001). After rehabilitation treatment, shoulder function and pain as well as shoulder scores were better in the painless jerk group (Mann-Whitney U test, P < .001).
In the painless group, pain (from 3.6 ± 3.1 to 0.2 ± 0.5), function (from 42 ± 15 to 93 ± 14), and shoulder scores such as the Rowe (from 50 ± 11 to 93 ± 10), UCLA (from 24 ± 4 to 33 ± 3), and modified ASES (from 68 ± 13 to 92 ± 8) scores were improved (Wilcoxon test, P < .001) (Table 2). Fifty shoulders (93%) responded to the rehabilitation program for a mean of 4 months (range, 1–7 months). All 50 shoulders improved shoulder function, and preexisting shoulder pain or discomfort disappeared. However, the clunking persisted in the jerk test, although it was still painless. Four shoulders (7%) were unresponsive to rehabilitation. Objective and subjective measurements were stationary or aggravated. Of these 4 shoulders, the jerk test was converted to a painful clunk in 1 shoulder and remained a painless clunk in the other 3 shoulders.
Clinical Outcome of the Painless Group
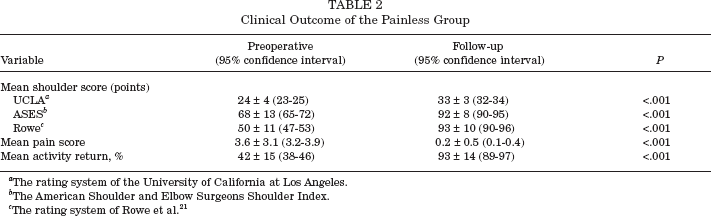
The rating system of the University of California at Los Angeles.
The American Shoulder and Elbow Surgeons Shoulder Index.
The rating system of Rowe et al. 21
In the painful jerk group, overall, shoulder function improved but still was unsatisfactory in both subjective (pain score, from 3.5 ± 1.4 to 2.3 ± 1.8; function score, from 41 ± 17 to 61 ± 19) and objective measurements (Rowe score, from 52 ± 12 to 69 ± 15; UCLA score, from 23 ± 3 to 27 ± 5; modified ASES score, from 65 ± 12 to 72 ± 16) (Table 3). Five shoulders (16%) were responsive to the rehabilitation, whereas the other 30 shoulders (84%) were unresponsive to the rehabilitation. These 30 shoulders that failed rehabilitation had persistent, positive, painful jerk tests with preexisting symptoms.
Clinical Outcome of Painful Group
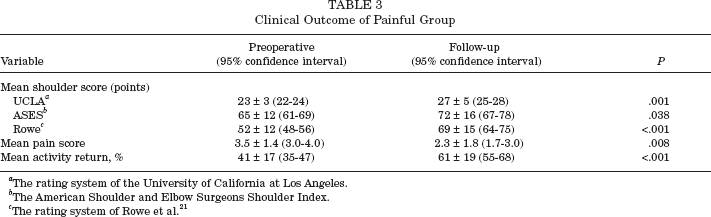
The rating system of the University of California at Los Angeles.
The American Shoulder and Elbow Surgeons Shoulder Index.
The rating system of Rowe et al. 21
Arthroscopic Findings
All 34 shoulders unresponsive to the rehabilitation had a variable degree of posteroinferior labral lesions. The labral lesions were type I in 8, type II in 13, type III in 10, and type IV in 3 shoulders according to classification of Kim et al 11 (Figure 2). There were 6 shoulders with type II superior labral lesions, 5 shoulders with Ellman 7 grade I articular surface partial-thickness tears, and 4 shoulders with reverse Hill-Sachs lesions. Of the 4 patients who had previously painless jerk tests, the 1 who had conversion to the painful jerk test showed a type II lesion and the other 3 patients had type III lesions.
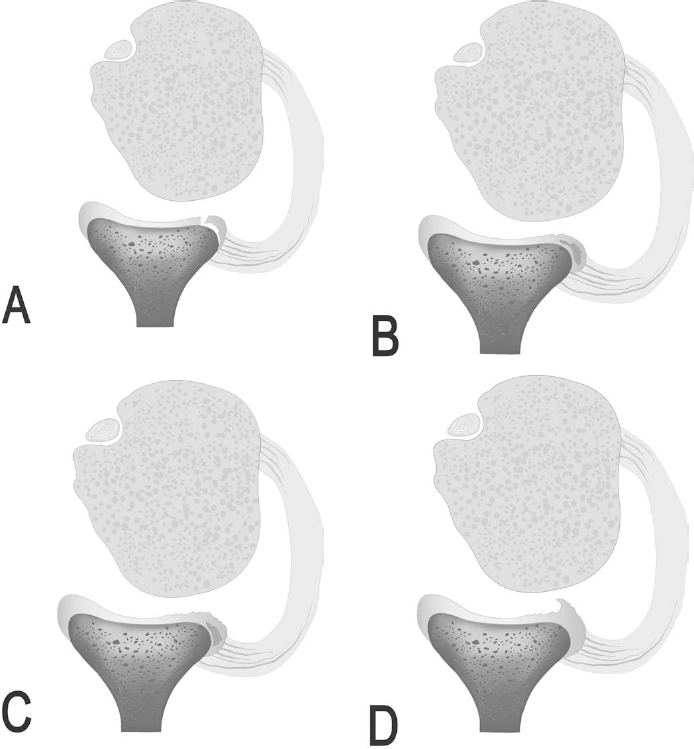
Four types of labral lesions of the posteroinferior instability. A, type I: incomplete detachment; B, type II: marginal crack or Kim lesion; C, type III: chondrolabral erosion; D, type IV: flap tear.
Discussion
Although nonoperative treatment has been the initial modality of treatment for posteroinferior instability of the shoulder, there has been no predictive sign for the success of nonoperative treatment. This study demonstrated that the jerk test can be used as a predicting measure for nonoperative treatment. The painful clunk in the jerk test is invariably associated with a structural defect, the posteroinferior labral lesion.
Diagnosis of posteroinferior multidirectional instability by physical examination is usually difficult. The clinical presentation of patients is variable, and the treating physician must maintain a high index of suspicion of this condition in young, active patients with atypical shoulder pain. 15 Diagnostic tests include the posterior apprehension sign, 25 the posterior stress test,2, 19 the jerk test,1, 8, 16 and the load-and-shift test. 23 However, these diagnostic examinations have not provided useful clues in selecting a treatment modality. It has been the general consensus that a prolonged course of nonoperative treatment including rehabilitation exercises should be instituted before considering surgical intervention.
The jerk test, which is sometimes called the posterior stress test, is positive for almost all patients with posterior instability of the shoulder.1, 2, 8, 15, 19 A sudden clunk during simultaneous adduction and posteriorly directed axial loading in the involved arm in 90° abduction may or may not elicit sudden pain. The jerk test is a dynamic test; this horizontal maneuver simulates posteroinferior subluxation of the shoulder and reproduces the same symptoms that occur during daily and sports activities. Although the posterior clunk is usually typical in posteroinferior instability, pain can be the only positive finding, and posterior clunking can be traced in some patients.
Although previous researchers have reported that simultaneous pain generated with the jerk test indicated a positive sign of posteroinferior instability, others did not clearly describe the results of the test.1, 2, 14–16, 26 In this study, shoulders with a simple posterior clunk without pain or discomfort were best treated with a nonoperative treatment. The majority of patients had satisfactory outcomes with rehabilitation exercises, despite persistent posterior subluxation.
However, the majority of shoulders with the painful jerk test failed to improve with nonoperative treatment. Arthroscopic findings support the hypothesis that the abrupt pain during the jerk test may be elicited from a rim loading of the humeral head over the pathologic posteroinferior labral lesion (Figure 3). Kim et al11, 13 reported that all patients with traumatic posterior instability and atraumatic posteroinferior multidirectional instability had a labral lesion. They introduced a concealed labral lesion in which the superficial portion had a marginal crack and the deep portion of the posteroinferior labrum was loose.11–13 The posteroinferior labrum became flat by a loss of normal labral height. This may suggest that the posteroinferior labrum may have been subjected to structural remodeling by repetitive posterior subluxation. The researchers introduced capsulolabroplasty, which creates a complete release of the posteroinferior labrum from the glenoid and reattaches on the surface of the glenoid. Superior shift of the posteroinferior and anteroinferior capsule as well as closure of the rotator interval were added. Of 31 patients, 30 patients were stable after a mean follow-up of 51 months. 13
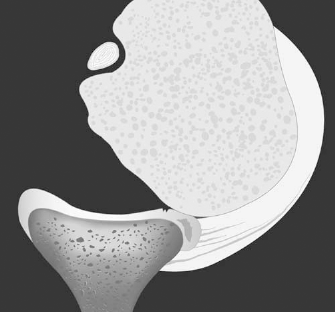
Abrupt pain during the jerk test may be elicited from a rim loading of the humeral head over the pathologic posteroinferior labral lesion.
The strength of this study is that we selected patients in a consecutive series from one surgeon's experience. All data were prospectively collected. The weakness is that there was no comparative analysis of the arthroscopic findings between the 2 groups because we performed the arthroscopic examination in patients who had failed nonoperative treatments. Although rehabilitation exercises successfully improved the shoulder symptoms of the painless jerk group, we do not have further knowledge as to whether these symptoms recurred afterward. However, it seems that nonoperative treatment does not provide permanent relief of pain. Six patients who were previously successful with the nonoperative treatment and showed a painless jerk test developed recurrent shoulder symptoms and a painful jerk test. All of these patients had posteroinferior labral lesions during arthroscopic examination. Therefore, it seems that the painless jerk test can be converted to a painful jerk test with time.
In conclusion, the jerk test is a hallmark for predicting the prognosis of nonoperative treatment for posteroinferior instability. Shoulders with a painful jerk test have posteroinferior labral lesions.