
Abstract
Background
No consensus exists on the amount of tension that should be applied to anterior cruciate ligament grafts to best facilitate graft incorporation and re-create normal knee mechanics.
Hypothesis
Differences in initial graft tension will affect postoperative knee stability.
Study Design
Prospective, randomized, double-blind clinical trial.
Methods
Forty-nine patients undergoing bone-patellar tendon-bone autograft anterior cruciate ligament reconstruction by a single surgeon were randomized into high-tension (n = 27) and low-tension (n = 22) groups. Grafts were set at 90 N or 45 N. Arthrometric measurements (KT-1000 arthrometer manual maximum) of anterior tibial displacement and knee range of motion were made before surgery and at 1 week and an average of 20 months after surgery. Knee outcome scores were collected before and after surgery, and a single-leg hop test was also performed at final follow-up.
Results
After anterior cruciate ligament reconstruction, anterior tibial displacement was significantly greater in the patients in the low-tension group (P < .05). The side-to-side difference in anterior tibial displacement in the high-tension and low-tension groups was 1.1 ± 1.7 mm versus 2.4 ± 2.4 mm 1 week after surgery and 2.2 ± 1.6 mm versus 3.0 ± 2.2 mm at follow-up. Five patients had abnormal anterior tibial displacement (>5 mm side-to-side difference), and all were in the low-tension group (P <.05). Knee outcome scores improved with surgery (P < .01), with similar results for low-tension and high-tension groups. Hop test deficits were not different between groups.
Conclusions
Initial graft tension affects the restoration of knee stability. A graft tension of 45 N was not sufficient for restoring knee stability.
Many variables must be taken into account when performing ACL reconstruction, all of which may have an effect on the ultimate outcome. Choice of donor graft tissue, 4 anatomic placement of the bone tunnels,5, 7 position of the knee at the time of graft tensioning,5, 19 method of graft fixation, 21 and initial tension on the graft at the time of fixation11, 14, 15, 18, 22, 23 have all been implicated as important factors in ACL reconstruction. No consensus has been reached regarding the amount of graft tension needed to re-create normal knee mechanics while providing the ideal biologic milieu for graft healing. In practice, few surgeons control for the degree of tension placed on the graft at the time of fixation. Undertensioning of the graft may result in a nonfunctional graft, leading to an excessively lax and unstable knee. 3 Overtensioning the graft may overconstrain the knee, leading to tissue failure, failure of fixation, or restriction in range of motion (ROM).5, 14, 15, 19 Excess tension may also create a less favorable milieu for biologic incorporation of the graft.12, 24 Katsuragi et al 12 recently demonstrated that overtensioning the graft had a detrimental effect on the biomechanical properties of the graft in a canine model.
Several in vitro studies have used cadaver models to examine the effect of initial graft tension on the biomechanics of the knee after ACL reconstruction.4, 5, 7, 9, 14, 15, 18, 19 In vivo studies have used a canine model to examine the effect of controlled initial graft tension on outcome.2, 6, 12, 24 In addition, 2 prospective clinical studies22, 23 used a human model to evaluate the effect of initial graft tension on ACL reconstruction. Yasuda et al 23 demonstrated that lower initial graft tension was associated with increased postoperative laxity 2 years after reconstruction with autogenous doubled hamstring tendons. This effect was apparent for initial graft tensions of 20 N versus 80 N. Conversely, van Kampen et al 22 demonstrated no effect of initial graft tension on postoperative laxity 1 year after reconstruction using autogenous bone–patellar tendon–bone grafts. However, only initial graft tensions of 20 N and 40 N were compared. The current literature does not address whether initial graft tensions higher than 40 N would provide a greater improvement in knee stability after ACL reconstruction using autogenous bone–patellar tendon–bone grafts. The purpose of this study was to examine the effect of initial graft tension on knee stability and functional outcome in patients undergoing bone–patellar tendon–bone ACL reconstruction in a randomized prospective fashion.
Materials and Methods
Graft Tensioning Measurement Technique
A piezoelectric force transducer (Kistler Instruments, Amherst, NY) was used to measure graft tension during ACL reconstructions using central-third bone–patellar tendon–bone autografts. The transducer was calibrated before each procedure and was set to a measurement sensitivity of 0.1 N. It was then placed in series with the tibial sutures to provide a force reading when manual tension was applied to the graft. Before attaching the force transducer, the graft was fixed at the femur using an interference screw and subsequently cycled 10 times to decrease creep. The graft was not pretensioned. Graft tension was recorded with the knee in full extension immediately before tibial graft fixation with an interference screw.
Pilot Study
A pilot study was initially carried out to determine the normal intersurgeon and intrasurgeon measurement range and variability for initial graft tension. In the pilot study, graft tension at the time of fixation was measured during 30 ACL reconstructions, 10 each performed by 2 experienced surgeons (A and B) and 1 senior resident (C). The surgeons were blinded to the tension they were applying at the time of fixation. An autogenous bone–patellar tendon–bone graft was used in each case. Graft tension was lower (P < .05) for surgeon B (47.9 ± 4.4 N) compared to surgeons A (82.8 ± 15.0 N) and C (71.4 ± 22.2 N). In addition, the coefficient of variation was 18.1% for surgeon A, 9.1% for surgeon B, and 31.1% for surgeon C. Measurement variability (coefficient of variation) was lower for the 2 experienced surgeons (A and B) compared with the inexperienced surgeon (C) (P < .05). Based on the upper 95% confidence interval for surgeon A and the lower 95% confidence interval for surgeon B, a high tension of 90 N and a low tension of 45 N were used for the randomized groups.
Randomized Trial
After signing informed consent forms, 49 patients with isolated ACL tears undergoing arthroscopically assisted reconstruction using a central-third bone–patellar tendon–bone autograft were prospectively randomized into 2 groups (high = 90 N and low = 45 N graft tension). The institutional review board approved the study procedures. There were 27 patients (19 men and 8 women) in the high-tension group and 22 patients (14 men and 8 women) in the low-tension group. The groups were similar in age (30 ± 7 years vs 33 ± 8 years), height (170 ± 13 cm vs 167 ± 17 cm), and weight (73.8 ± 12.2 kg vs 73.9 ± 15.7 kg). In the high-tension group, 14 patients had acute injuries (<2 months after injury), 6 had subacute injuries (2–6 months after injury), and 7 had chronic injuries (>6 months after injury). In the low-tension group, 14 patients had acute injuries, 2 had subacute injuries, and 6 had chronic injuries.
Surgical Technique
All reconstructions were performed by a single surgeon (surgeon A) using an identical arthroscopically assisted single-incision technique for each patient. Patients received either epidural anesthesia or general anesthesia. A pneumatic tourniquet was used in all cases. The central third of the patellar tendon was then incised using a 10-mm or 11-mm double-bladed scalpel. The tibial and patellar bone blocks were then harvested. The tibial bone blocks typically measured 25 to 30 mm in length, and the patellar bone blocks measured 20 to 25 mm in length. The patellar harvest site was bone grafted in each case using the autologous bone remaining after graft preparation. The tunnel on the femoral side was placed using the Linvatec (Largo, Fla) over-the-top guide with a desired location of 10:30 for a right ACL and 1:30 for a left ACL. Guide pins were placed and overdrilled with the appropriate sized reamer.
Associated Pathologies
There were minimal differences in associated pathologies between patients in the high-tension and low-tension groups. In the high-tension group, 1 patient had a grade I medial collateral ligament sprain and 1 patient had a grade II lateral collateral ligament sprain; 8 patients had a medial meniscal tear, 4 had a lateral meniscal tear, and 1 had combined medial and lateral medial tears. In addition, 1 patient had grade I chondromalacia of the patella, and 3 patients had grade III chondromalacia (1 medial femoral condyle and 2 lateral femoral condyle). In the low-tension group, 3 patients had a lateral meniscal tear, and 4 patients had both lateral and medial meniscal tears; 3 patients had grade I chondromalacia (2 lateral tibial plateau, 1 patella), 1 patient had grade II chondromalacia of the lateral femoral condyle, 2 patients had grade III chondromalacia (1 medial femoral condyle, 1 lateral femoral condyle), and 1 patient had grade IV chondromalacia of the medial tibial plateau.
Five medial meniscal repairs were performed (1 in the low-tension group and 4 in the high-tension group). Six partial medial meniscectomies (1 in the low-tension group and 5 in the high-tension group) and 9 partial lateral meniscectomies were performed (6 in the low-tension group and 3 in the high-tension group). One patient in the high-tension group had a total lateral meniscectomy.
Postoperative Regimen
Postoperatively, all patients were encouraged to bear weight with the knee braced in extension, using crutches as needed. All crutch use was discontinued at 1 week after surgery. The brace was unlocked for ambulation at 2 weeks and discontinued 4 weeks after surgery. During the first postoperative week, patients used continuous passive motion, performed voluntary quadriceps contractions in extension (quadriceps set), and performed hip-strengthening exercises. Formal physical therapy began 1 week after surgery. The rehabilitation protocol has been previously described. 17
Clinical Evaluation
Each patient was evaluated before surgery by history and physical examination. The physical examination included graded assessments for the presence of an effusion and the status of the Lachman and pivot-shift tests. Objective testing included ROM of the knee as measured by a goniometer and laxity as measured by a knee arthrometer (KT-1000 arthrometer, MEDmetric Corp, San Diego, Calif). Clinical evaluations were performed by a single blinded examiner. Subjective evaluation consisted of a modified Knee Outcome Survey (KOS). 10
Arthrometric measurement (KT-1000 arthrometer) of knee stability was the primary dependent variable for determining the effect of graft tension on knee stability after ACL reconstruction. 13 Side-to-side difference in anterior tibial displacement (ATD) with manual force applied to the calf (manual maximum) was recorded. Side-to-side differences in ATD were categorized as normal (<3 mm), nearly normal (3–5 mm), abnormal (6–10 mm), and severely abnormal (>10 mm). 20 Measurements were made on all 49 patients before surgery, 1 week after surgery, and again at an average of 20 ± 14 (± SD) months after surgery (6 months to 4 years). The measurement 1 week after surgery provided an indication of stability before graft incorporation. All patients were also evaluated on each occasion for knee joint effusion (0, +1, +2, +3) and passive knee ROM measured goniometrically in flexion and extension. KOS scores and single-limb hop test scores were also recorded at follow-up. Hop distance on the involved and noninvolved sides was recorded and reported as a deficit. The same examiner made all preoperative and postoperative measurements and was blinded as to whether the patient was in the high-tension or low-tension group. In a subgroup of 22 patients (12 low tension, 10 high tension), all measurements were made once between 6 months and 1 year after surgery and again more than 2 years after surgery (range, 2–4 years). This subgroup was tested to examine changes after patients had resumed normal activities for a prolonged period of time.
Statistics
The effect of initial graft tension on static knee stability after ACL reconstruction was determined by a mixed-model analysis of covariance (ANCOVA) with the effect of time (1 week vs final follow-up) as a within-subjects factor and graft tension (high vs low) as a between-subjects factor. The ANCOVA controls for the potential confounding effects of other variables that may affect the dependent variable (postoperative ATD). For these analyses, preoperative side-to-side difference in ATD was the only covariate (see the Results section). Similarly, an ANCOVA was used to examine the effect of initial graft tension of postoperative knee extension and flexion loss with preoperative extension and flexion losses entered as covariates in each analysis. Preoperative motion loss is known to be a risk factor for postoperative motion loss. 16 The comparison of motion loss between groups was performed to determine if a high initial graft tension overly constrained the knee.
The effect of initial graft tension on KOS was tested by mixed-model analysis of variance with the effect of time (1 week vs final follow-up) as a within-subjects factor and tension (high vs low) as a between-subjects factor (there were no confounding variables [covariates]). The effect of graft tension on the single-limb hop tests was tested by independent t test. All data in the text are reported as mean ± standard deviation. A χ2 analysis was used to test for between-group differences in categorical variables.
Because arthrometric knee stability was the primary dependent variable in the present study, it was essential that the sample size yielded adequate power to detect a difference between groups. Based on values from a previous study examining the effect of graft tension on knee stability after ACL reconstruction using a patellar tendon graft, 22 standard deviations of 1.4 mm and 1.8 mm for between-subject variance in postoperative stability measures were used. Using these values, it was determined that with a sample size of 49, an effect size (average difference between groups) of 1.6 mm could be detected as significant (P < .05) at 80% power.
Results
Arthrometric Knee Stability
Before surgery, side-to-side difference in ATD was not significantly different between groups (high tension, 5.7 ± 2.7 mm; low tension, 5.3 ± 2.4 mm; P = .62). Four patients (3 low tension, 1 high tension) were graded as normal (<3 mm), 20 patients (8 low tension, 12 high tension) were graded as slightly abnormal (3–5 mm), 24 patients (11 low tension, 13 high tension) were graded as abnormal (6–10 mm), and 1 patient (high tension) was graded as highly abnormal (>10 mm). Preoperative arthrometric measurements were similar between patients with acute (5.4 ± 2.8 mm), subacute (5.6 ± 2.7 mm), and chronic injuries (5.7 ± 2.1 mm) (P = .91).
Side-to-side difference in ATD at 1 week and at final follow-up after surgery was correlated to preoperative ATD (r = 0.48–0.30; P < .05). Postoperative side-to-side difference in ATD was unrelated to extension loss (P = .34 at 1 week; P = .46 at follow-up), effusion (P = .25 at 1 week), or gender (P = .11); therefore, these variables were not entered as covariates.
Side-to-side difference in ATD was significantly greater in the low-tension group after surgery (P = .01) (Table 1). Five patients in the low-tension group had abnormal laxity at final follow-up compared with 0 patients in the high-tension group (P < .05). The effect of graft tension was most apparent in those patients with abnormal preoperative laxity (P < .05) (Table 2). Of the 25 patients with abnormal or highly abnormal preoperative laxity, 4 patients in the low-tension group still had abnormal laxity 7 months after surgery compared with 0 patients in the high-tension group. All subjects were considered to have intact grafts based on a firm endpoint with Lachman testing. The tightest reconstructed knees were in 2 patients in the high-tension group who had 1 mm less ATD on the involved side.
KT-1000 Arthrometer Side-to-Side Difference, a mm

Mixed-model analysis of covariance: effect of graft tension, P = .01; effect of time, P = .13; graft tension by time, P = .48.
KT-1000 Arthrometer Grades at 20 Months After Surgery in Patients With an Abnormal Preoperative Grade a
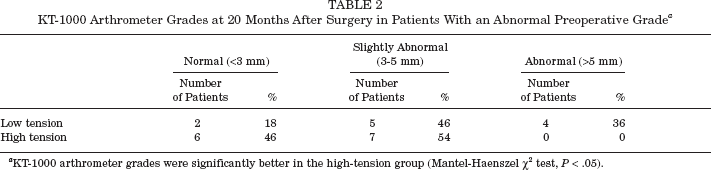
KT-1000 arthrometer grades were significantly better in the high-tension group (Mantel-Haenszel χ2 test, P < .05).
Arthrometric measurements were also taken on 22 patients once between 6 months and 1 year after surgery and again between 2 and 4 years after surgery. This subgroup was tested to determine whether the results changed from 6 months to 4 years after surgery. Side-to-side difference in ATD was 2.3 ± 1.8 mm at 6 months to 1 year after surgery (low tension = 2.8 mm; high tension = 2.2 mm) and 2.1 ± 1.6 mm at 2 to 4 years after surgery (low tension = 2.6 mm; high tension = 2.2 mm), indicating no increase in laxity over time (P = .84).
Knee Extension and Flexion ROM
Before surgery, extension loss was 3.0° ± 4.9° in the low-tension group and 0.8° ± 1.4° in the high-tension group. Extension loss 1 week after surgery was 6.0° ± 4.0° and 5.5° ± 3.4° in the low-tension and high-tension groups, respectively. By 20 months after surgery, extension loss had decreased (P < .01) to 1.3° ± 3.3° and 0.9° ± 3.5° in the low-tension and high-tension groups, respectively. Postoperative knee extension loss was unaffected by initial graft tension (P = .99). Two patients in the low-tension group and 1 patient in the high-tension group had ≥5° extension loss at final follow-up. All 3 of these patients lacked full extension before surgery. Postoperative knee flexion loss was also unaffected by initial graft tension (0.54); at final follow-up, 1 patient in the low-tension group and 2 patients in the high-tension group had more than 10° flexion loss.
Postoperative Complications
Four patients had postoperative complications resulting in a second arthroscopic procedure. One patient (in the low-tension group) had an infection and 3 patients (2 in the high-tension group) had arthrofibrosis. All procedures were performed within 12 weeks of initial surgery. All 3 patients requiring arthroscopic debridement for arthrofibrosis lacked full extension before ACL reconstruction and had full return of motion after debridement.
Functional Outcome
The KOS and hop test measurement provided an indication of the patient's functional outcome; KOS improved comparing preoperative values to values at final follow-up (P < .001). Final KOS values were not different between the low-tension group (92 ± 4) and the high-tension group (90 ± 7) (P = .26). Side-to-side difference in the hop test (percent deficit) was 7.3% ± 9.2% for the low-tension group and 12.3% ± 10.6% for the high-tension group (P = .09).
Discussion
The only previous study examining the effect of initial graft tension on knee stability after autogenous bone–patellar tendon–bone ACL reconstruction was published by van Kampen et al, and the study found no difference between grafts set at 20 N and 40 N. 22 However, the forces in that study were lower than the tensions routinely applied during graft tensioning by the 3 surgeons who participated in the pilot testing for this study. Yasuda et al showed that a graft tension of 80 N in autogenous hamstring grafts resulted in better knee stability than did graft tension of 20 N. 23 Of note, the grafts in their study were fixed at 30° of knee flexion, whereas in the present study they were fixed in full extension. Therefore, the goal of our study was to further examine the effect of initial graft tension on knee stability after autogenous bone–patellar tendon–bone reconstruction using graft tensions within the normal range for experienced surgeons. Our results show significantly better arthrometric knee stability when a high initial graft tension was used. The magnitude of this effect was small and had limited power with this sample size. However, it is important to note that 5 patients in the low-tension group had abnormal laxity (>5 mm side-to-side difference in ATD) compared with no patients in the high-tension group. The results for those 5 patients are unsatisfactory according to International Knee Documentation Committee classifications, 1 and a KT-1000 arthrometer side-to-side difference of >5 mm has been used as criteria for surgical failure. 20
The possibility of overconstraining a knee when using high graft tensions has been examined. Yasuda et al suggested that less ATD on the involved side and/or extension loss may represent an overconstrained knee. 23 They reported that 2 patients whose hamstring grafts were set at 80 N had 3 mm less ATD on the involved side. In the present study, there was no evidence of overconstraint, with only 2 of 27 patients in the high-tension group having 1 mm less ATD on the involved side. An additional concern with overconstraining the knee was that patients may not regain full motion, but knee ROM was clearly not different between the high-tension and low-tension groups. It is important to note that grafts were fixed in full extension in the present study compared to 30° in the study by Yasuda et al. 23 Tensioning in full extension should limit the risk of overconstraint.
An additional concern with overtensioning the graft was that excessive tension could be detrimental to graft incorporation and subsequent tissue remodeling. Using a canine model, Katsuragi et al demonstrated that excessive graft tensioning resulted in lower graft stiffness and tensile strength over time. 12 Based on the change in ATD beyond 1 week after surgery, there was no evidence of graft “stretch out” in the high-tension group compared with the low-tension group.
Although the purpose of this study was to examine the effect of initial graft tension on postoperative knee stability, it was necessary to identify other factors affecting postoperative stability to control for confounding effects. Surprisingly, only one other factor—preoperative side-to-side difference in ATD—was related to ATD after reconstruction. This relationship indicates that it may be more difficult to restore normal stability in patients with greater preoperative side-to-side difference in ATD. In those patients with abnormal preoperative laxity (>5 mm side-to-side difference in ATD), a graft tension of 45 N was inadequate for restoring stability to clinically acceptable levels (Table 2). Only 2 of 11 patients with abnormal preoperative laxity had normal postoperative results (<3 mm side-to-side difference). Furthermore, all 5 patients with abnormal postoperative laxity were in the low-tension group, and 4 of these patients had abnormal preoperative laxity.
The mean side-to-side differences in ATD in the high-tension (2.2 ± 1.6 mm) and low-tension (3.0 ± 2.2 mm) groups are comparable to the values reported by van Kampen et al 22 of 2.6 ± 1.4 mm for the 20 N graft tension group and 2.5 ± 1.8 mm for the 40 N graft tension group. Of note, van Kampen et al reported that 4 of 38 patients (1 in the 20 N group and 3 in the 40 N group) had a ≥5 mm side-to-side difference in ATD. In the current study, 5 of 22 patients in the low-tension group (45 N) had a >5 mm side-to-side difference in ATD. Together, these findings indicate that a graft tension of up to 45 N is inadequate for restoring static knee stability.
The final stability value in the high-tension group (2.2 ± 1.6 mm) was appreciably greater than 0. Graft tensions in excess of 90 N may be required to achieve greater stability, but this may increase the number of patients having less ATD on the involved versus the noninvolved side (an indication of overconstraint). Although the present study demonstrates that knee stability after ACL reconstruction is affected by initial graft tension and preoperative laxity, numerous other factors can potentially affect ultimate knee stability. By documenting preoperative laxity and initial graft tension, other factors affecting graft tension can be more easily identified.
The lack of difference in functional outcome between high-tension and low-tension groups is consistent with the findings of Yasuda et al. 23 An average of 20 months follow-up may be inadequate time to see functional differences. In addition, the associated abnormalities probably affected functional outcome, and these were quite variable between groups. The primary concern would be to see if a low graft tension leads to recurrent instability and/or complete graft failure. None of the patients in this study had experienced graft failure or reported episodes of giving way at follow-up. It is possible that the increased laxity associated with a low initial graft tension has no long-term functional implications. However, a high graft tension of 90 N did not overconstrain the knee and resulted in better static knee stability and therefore may be a safer choice.
Conclusions
Established recommendations with regard to optimal ACL graft tension have yet to be elucidated. In an animal model, Katsuragi et al demonstrated that overtensioning the graft can be detrimental, but they acknowledged, “The upper and lower limits for the appropriate range remain unknown at present.”12(p55) Similarly, in a review of recommendations for ACL reconstruction, Fu et al concluded, “At present the precise amount of tension that should be applied to the graft has yet to be defined.”8(p126) The present study provides some insight with respect to the tensioning of bone–patellar tendon–bone autografts, indicating that a graft tension of 45 N may lead to increased laxity, whereas a tension of 90 N should provide improved stability without overconstraining the knee.