
Abstract
Although often perceived as a leisurely activity, golf can be a demanding sport, which can result in injury, usually from overuse and sometimes from poor technique. The shoulder is a commonly affected site, with the lead shoulder, or the left shoulder in the right-handed golfer, particularly vulnerable to injury. A thorough understanding of the biomechanics of the golf swing is help-ful in diagnosing and managing these injuries. Common shoulder problems affecting golfers include subacromial impingement, acromioclavicular arthrosis, rotator cuff tear, glenohumeral instability, and glenohumeral arthrosis. Although the majority of patients with these disorders will respond to nonsurgical treatment, including rest and a structured program of physical therapy, further benefits can be obtained with subtle modifications of the golf swing. Those golfers who fail to respond to nonsurgical management can often return to competitive play with appropriate surgical treatment.
Golf has become an increasingly popular sport, especially over the past 5 to 10 years, with an estimated 37 million participants and 518 million rounds played in 2001 in the United States alone. 2 With rapidly improving golf equipment technology, increasing development of golf courses, and expanding media coverage with its own dedicated 24-hour cable network, golf is more readily accessible to the general public than ever before.
Because of this growing golfing population, more patients of all ages will develop golf-related injuries. At first glance, the golf swing may appear to be a relatively benign activity, but on closer evaluation, it requires a synchronized effort of muscle strength, timing, and coordination to generate high clubhead speeds, often in excess of 100 mph, and to drive a ball more than 300 yd.
For the professional golfer, the shoulder is the third most commonly injured body area, after the lumbar spine and the wrist or hand.12,28 For amateur golfers in the United States, the shoulder has been cited as the fourth most commonly affected site, trailing the lumbar spine, the elbow, and the wrist or hand,26,38 but for European amateur golfers, it has been recently reported that the shoulder is the second most commonly affected region, after the elbow. 12 Professional and elite-level golfers often sustain injuries as a result of overuse from repeated swings during frequent practice sessions,12,27,28 sometimes performing up to 2000 or more swings per week. 18 Amateur golfers can also suffer problems from overuse as they work to improve their game. They may injure themselves as a result of poor swing mechanics,27,38 overzealous playing, 36 or from a traumatic event such as hitting the ground awkwardly when taking a large divot.
The purpose of this article is to review the current literature pertaining to shoulder conditions affecting golfers and to provide a foundation for evaluating and treating shoulder problems in this particular patient population.
Biomechanics/Electromyography Studies
To effectively appreciate the shoulder problems that afflict golfers, one must understand the biomechanics of the normal golf swing and the dynamic forces created by the shoulder girdle. The golf swing can be divided into 5 phases: (1) takeaway (from address until the club is horizontal), (2) backswing (from horizontal to top of backswing), (3) downswing (from top of backswing until the club is horizontal), (4) acceleration (from horizontal club to impact), and (5) follow-through (from ball contact until end of swing)17,32 (see Figure 1). Golfers may give a history of symptoms that occur only during 1 specific phase of the swing.
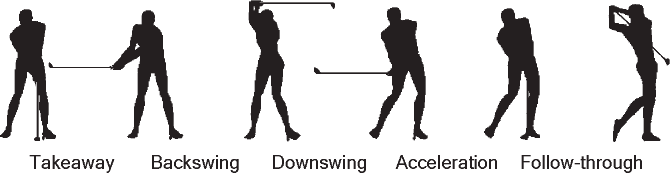
The 5 phases of the golf swing.
The lead shoulder (left shoulder for a right-handed golfer) is an important link during the golf swing. To generate power and clubhead speed, the skilled golfer will attempt to maximize the shoulder turn relative to the hip turn during the backswing. Using high-speed videography and 3-dimensional analysis techniques, this differential between the shoulder and hip rotation at the top of the back-swing has been confirmed in low-handicap golfers. 4 Interestingly, in amateur male golfers, the shoulder rotation has been shown to decrease with increasing age of the golfer when examined by high-speed camera motion analysis. 29
The relative activity of the rotator cuff muscles during the golf swing of professional golfers was examined by Jobe et al16,17 and later by Pink et al 32 using fine-wire electromyography (EMG) and high-speed photography. These researchers noted that there were no significant differences in muscle activity during the swing between male and female professional golfers. 17 They discovered that the supraspinatus and infraspinatus muscles in the lead shoulder demonstrated relatively low, synchronized activity throughout the swing, with peak activity during takeaway and follow-through, and concluded that these muscles act as abductors and external rotators to help to stabilize the glenohumeral joint. The subscapularis in both shoulders was the most active of the rotator cuff muscles, showing activity during most of the swing but especially during the acceleration phase. The latissimus dorsi and the pectoralis major demonstrated the most activity of all the shoulder muscles, with the latissimus dorsi acting maximally during the downswing and acceleration phases, whereas the pectoralis major demonstrated activity later in the swing, during acceleration and follow-through. Finally, the deltoid muscle was conspicuously nonactive, except for the anterior deltoid, which was most active during the follow-through phase of the swing, acting as a flexor of the arm (Table 1).
Relative EMG Activity of Rotator Cuff and Shoulder Muscles During the Golf Swing for a Right-Handed Golfer a
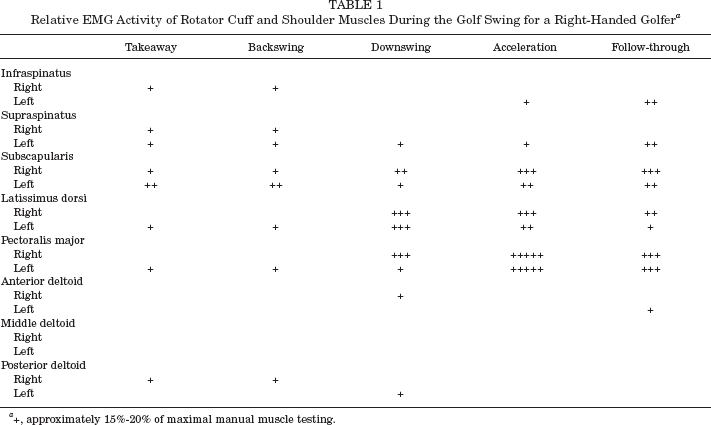
+, approximately 15%-20% of maximal manual muscle testing.
From the same laboratory, scapular muscle activity during the golf swing was also evaluated in a similar manner. 21 The trapezius muscle helped to retract the scapula and showed the greatest activity during the downswing and acceleration phases for the lead arm, whereas peak activity of the trapezius in the trailing arm occurred during takeaway. For the rhomboid and levator scapulae muscles of the lead arm, scapular retraction and elevation were most active during the downswing and acceleration phases—for the trailing arm, both muscles were also active during the downswing to help with scapular protraction and overall scapular stabilization. Finally, the serratus anterior muscle acted mainly as a scapular protractor and demonstrated peak activity during the downswing, acceleration, and follow-through phases of the trailing arm. In contrast, for the leading arm, the serratus anterior exhibited low, synchronized activity throughout the entire swing, which may explain why it can be susceptible to fatigue in some golfers (Table 2).
Relative EMG Activity of Scapular Stabilizer Muscles During the Golf Swing for a Right-Handed Golfer a
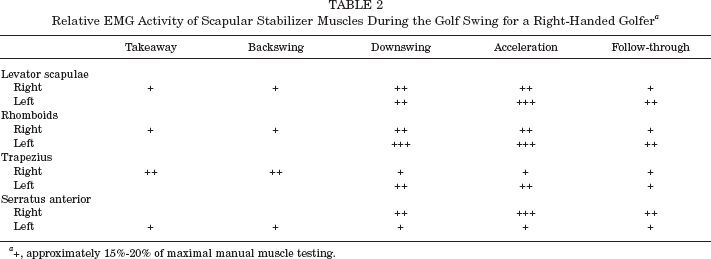
+, approximately 15%-20% of maximal manual muscle testing.
It should be noted that these EMG studies were performed in healthy, elite-level golfers whose swings were highly reproducible. Nevertheless, these studies have helped us to appreciate the relative contributions of the rotator cuff and shoulder girdle muscles and have also served as a guide to better understand the pathoanatomical mechanisms for golfing shoulder injuries. Moreover, this information has served as a basis for the training and improvement of swing mechanics as well as for appropriate rehabilitation programs that involve selective strengthening of the rotator cuff and scapular stabilizers.16,20,21,33
In contrast to professional golfers who consistently activate the same muscles each time they swing, amateur and recreational golfers tend to have erratic muscle control and often cannot duplicate the swing with each shot.20,32 This inconsistency results in poor mechanics, to the point that practice and repeated swinging can be harmful and may lead to premature injury.
Clinical Evaluation
As always, a careful history and thorough physical examination are critical in making an accurate diagnosis when evaluating a golfer with shoulder problems. The age of the golfer can be very helpful in making a diagnosis. In general, younger golfers are more likely to have instability or a traumatic injury; middle-aged golfers tend to have sub-acromial impingement, rotator cuff disease, or acromioclavicular disease; and older golfers can also have injury to the rotator cuff as well as arthrosis of the glenohumeral joint. As mentioned earlier, the lead shoulder, most commonly the left shoulder in the right-handed golfer, is usually the symptomatic side. In a survey of professional golfers, injuries to the left shoulder were almost 3 times more common than injuries to the right shoulder, 28 and more recently, it has been reported that more than 90% of shoulder problems in golfers involved the lead shoulder.24,32 The character, location, and nature of the onset and duration of shoulder pain should all be elicited by history. Any prior history of shoulder injury or trauma, as well as any cervical spine symptoms, should be carefully documented.
In addition, the examiner should ask the golfer during which phase of the golf swing the symptoms are most troublesome. For example, during the backswing, the lead shoulder undergoes internal rotation, forward flexion, and cross-body adduction as it moves to the top of the back-swing. These positions can exacerbate subacromial impingement and acromioclavicular joint disease and may provoke associated symptoms. Posterior shoulder discomfort during the top of the backswing, when the lead arm is fully adducted across the body, may represent posterior glenohumeral instability. During the follow-through of the swing, the lead shoulder is abducted and externally rotated, and symptoms during this stage of the swing can suggest a diagnosis of anterior instability or biceps tendinitis.
On physical examination, a thorough cervical spine and upper extremity evaluation should always be performed, including a careful neurologic and vascular examination. A complete shoulder evaluation, which includes inspection for atrophy and scapular winging, assessment of both glenohumeral and scapulothoracic motion, palpation for any areas of tenderness, and strength testing, should always be performed. In addition, special provocative tests for shoulder impingement, acromioclavicular joint disease, rotator cuff abnormality, superior labrum tears, biceps dis-ease, and instability should be performed to help narrow the diagnosis. Perhaps most helpful is asking the golfer to demonstrate the full golf swing so that the specific motion that produces symptoms can be determined. Moreover, selective injection of local anesthetic into suspected areas of abnormality, such as the acromioclavicular joint or the subacromial space, can be very helpful in clarifying the diagnosis.
Radiographic evaluation usually consists of standard plain radiographs, including anteroposterior, axillary lateral, and supraspinatus outlet views. An MRI should be employed when injuries to the rotator cuff or labrum are suspected. The use of MRI arthrography with a gadolinium-containing contrast agent may enhance the identification of subtle labral tears.
Subacromial Impingement/Acromioclavicular Joint/Rotator Cuff Disease
Although strictly not an overhead sport, golf still requires an element of humeral elevation and rotation to perform a mechanically sound swing. It is usually at the extremes of range of motion (such as at the top of the backswing or the end of follow-through) when patients will experience symptoms. Moreover, patients with rotator cuff disease may be weak during initial takeaway, and this could perpetuate poor swing mechanics.
Rotator cuff disease and subacromial impingement involving the lead shoulder are among the most common problems in golfers. In a review of 412 patients with golf-related injuries, 85 patients had shoulder symptoms, and 79 of these patients (93%) demonstrated rotator cuff or subacromial disease. 16 A case report has described a professional golfer with impingement occurring at the top of the backswing and the end of follow-though, associated with a partial rotator cuff tear. 18 He was treated with arthroscopic subacromial decompression and debridement of the rotator cuff, and after 3 months of rehabilitation, he was able to return to competitive play.
Another recent study 40 examined 29 recreational golfers, average age 60 years, with subacromial disease and rotator cuff tears. At an average follow-up of 3 years after undergoing acromioplasty and rotator cuff repair (approximately half of the patients had arthroscopic acromioplasty and mini-open repair), all but 3 patients returned to playing golf with no difference in handicaps or driving distance. The authors concluded that surgery to flatten the acromion and repair the rotator cuff predictably allows most recreational-level golfers to return to pain-free golf at a similar competitive level. This is in contrast to a previous report 39 suggesting that surgical treatment of rotator cuff tears in athletes, mostly throwers and pitchers, did not consistently allow these overhead athletes to return to their previous level of play.
Golfers may be able to return to play more readily because demands placed on their shoulders in terms of range of motion and rotator cuff activity are usually less than those required for true overhead athletes. Data from EMG studies mentioned previously suggest that the infra-spinatus and supraspinatus muscles demonstrate a relatively low but synchronized level of activity throughout the swing. Furthermore, modifications to the golf swing, such as shortening the backswing or abbreviating the follow-through, can occur postoperatively and may not have a significant detrimental effect on ball striking and driving distance—in fact, these changes may result in a more consistent swing.
Acromioclavicular joint disease is another common shoulder problem that affects golfers. A review of 35 professional or low-handicap golfers with shoulder pain revealed acromioclavicular joint disease (53%) to be the most common cause of the pain, followed by rotator cuff tendinitis and impingement (26%). 25 The majority of golfers experienced symptoms at the top of the backswing when the lead arm is placed in maximal cross-body adduction and when forces across the acromioclavicular joint are high. 3 All but 1 golfer were able to return to competitive golf after appropriate treatment, consisting of physical therapy, swing modification, or distal clavicle excision when nonsurgical measures had failed.
Glenohumeral Instability
To generate power during the swing, elite-level golfers will attempt to maximize their shoulder turn relative to their hip turn. 4 This maneuver often requires a great deal of shoulder flexibility, and some golfers may even demonstrate hyperlaxity. Because of overuse and repetitive microtrauma, capsular and labral structures often become injured or attenuated. 18
Mallon and Colosimo 25 described a 12% incidence of posterior instability in their series of 35 professional and competitive golfers with shoulder pain. In a recent retrospective review by Hovis et al, 13 8 elite-level golfers were noted to have posterior glenohumeral instability of the lead shoulder with associated secondary subacromial impingement. At an average of 4.5 years of follow-up, all golfers had returned to the same level of competitive play. Two patients were treated nonsurgically with physical therapy alone and returned to play within 6 weeks, whereas 6 patients were treated surgically with arthroscopic posterior thermal capsulorrhaphy and subacromial decompression when indicated, and most returned to play by 4 to 5 months. The authors noted that the golfers described a sensation of pain and instability at the top of the back-swing when the lead arm was fully adducted across the body. This correlated with physical examination findings of posterior instability during the load-and-shift test and posterior apprehension with loading. They hypothesized that posterior instability may occur because of a relative dominance of the subscapularis muscle compared to the other rotator cuff muscles, and this imbalance may render the glenohumeral joint susceptible to posteriorly directed forces, especially if fatigue of the serratus anterior muscle also occurs.
Anterior instability can also occur in the golfer. In theory, the leading arm would be vulnerable at the end of the follow through phase of the swing, when the arm is in maximal abduction and external rotation. Nonsurgical treatment with a structured therapy program of rotator cuff and scapular stabilizer strengthening will alleviate symptoms in most cases.18,24 However, surgical stabilization is indicated if symptoms persisted after unsuccessful nonsurgical management. This has been described in a case report involving a professional golfer with anterior shoulder pain and demonstrating primarily anterior instability on physical examination. 18 After a failed trial of physical therapy, an open anterior capsulolabral reconstruction was performed, and the patient resumed playing on the tour at 1 year after surgery.
Although this case illustrates that anterior instability in the golfer can be successfully treated with open surgical stabilization, as our arthroscopic techniques continue to improve, it is becoming more apparent that instability can also be managed with arthroscopic techniques. There have been numerous reports describing the arthroscopic treatment of instability in the athlete,6,7,11,23,34 but there have been no clinical studies specific to the golfing population that support these techniques. It should be noted that recent clinical studies9,10 have suggested that the use of electrothermal capsulorrhaphy as an isolated procedure to treat instability in athletes is inadequate, resulting in high recurrence rates and the inability for the athlete to return to competitive play.
Superior Labrum/Biceps Disease
Although much more common in true overhead throwing athletes,1,5,8,15 superior labrum lesions and biceps tendon disorders can also occur in golfers. Anterior and posterior superior labrum fraying secondary to internal impingement has been described in 2 case reports involving professional golfers. 18 For 1 golfer, modification to a shorter backswing completely resolved his symptoms. For the other golfer, after failed nonsurgical treatment, arthroscopic debridement of the labrum and addressing the anterior capsular laxity allowed this patient to return to competitive golf. Otherwise, there have been no studies in the literature reporting the incidence, treatment, or outcomes of superior labral anterior posterior (SLAP) lesions or biceps tendon disorders in golfers, but our personal experience confirms that these disorders do occur in both recreational and low-handicap golfers. Those with SLAP tears most often complain of pain affecting the lead shoulder during the end of the backswing or beginning of the downswing when the shoulder is loaded with the arm in the cross-body adduction position. Occasionally, there will be associated mechanical complaints of clicking or catching, and the golfer may also complain of subjective weakness, especially at ball contact during the swing. For isolated biceps tendinitis, anterior shoulder pain is most marked during the later part of the follow-through phase, when the lead arm is maximally abducted and externally rotated and the shoulder is extended. Usually, an initial treatment program of rest, physical therapy, and anti-inflammatory medication is successful in alleviating symptoms. Those golfers whose symptoms persist despite adequate nonsurgical treatment can be treated successfully with arthroscopic surgery to closely evaluate the superior labrum and biceps complex and to either debride or repair the SLAP tear in the customary fashion.5,22,35 However, to our knowledge, there are no case series in the literature reporting the results and outcomes of golfers treated surgically for SLAP tears or biceps disorders.
Arthritis
It is estimated that approximately 25% of the golfers in the United States are age 65 years or older, 37 and as our population ages, we can expect this number to increase. Degenerative joint disease is also prevalent in this age group, and many of these patients are avid golfers. 19 In the previously cited series of 35 professional and competitive golfers with shoulder pain, there was a 3% incidence of glenohumeral arthritis. 25
Glenohumeral arthroplasty for symptomatic gleno-humeral arthritis has resulted in successful outcomes in golfers. In a retrospective review of 24 recreational golfers who underwent shoulder arthroplasty, 23 patients were able to resume playing golf at an average of 4.5 months after surgery, and 18 of these patients improved their scores by almost 5 strokes at an average of 53 months of follow-up. 14 None of the patients reported significant pain or demonstrated evidence of component loosening. Interestingly, these same authors polled 50 members of the American Shoulder and Elbow Society, and most surgeons (91%) allow shoulder arthroplasty patients to resume playing golf at an average of 4.3 months after surgery and have not noticed any increased loosening of components. 14 Almost 60% of the surgeons polled felt that no limits should be placed on the patients, and more than 70% believed that component wear would not be a problem in these patients.
A review of golfers with total shoulder arthroplasty (unpublished data) revealed that most golfers are able to return to playing and are very satisfied with their return level of play. We also have not noted any increased radiographic evidence of component loosening. Although no published studies have examined the joint reactive forces on the glenohumeral joint in golfers, we have found that these patients appear to tolerate the golf swing quite well, especially if the resurfaced shoulder is the trailing arm. We allow our shoulder arthroplasty patients to eventually play golf without any limitations, provided they do not have symptoms. The early rehabilitative phase after total shoulder arthroplasty is focused on regaining motion while protecting the subscapularis muscle repair. Provided there are minimal or no symptoms, patients are allowed to reacquaint themselves with their golf game by beginning with putting at 6 to 8 weeks after surgery. This places minimal forces on the shoulder replacement and allows the patient to regain a feel for striking a golf ball. At 10 to 12 weeks after surgery, light chipping and pitching drills are permitted as the patient gains more comfort with the golf swing. By this time, the subscapularis should be well healed, and any rotator cuff activity should be well tolerated. At 3 months after surgery, provided range of motion and strength goals are met, hitting short and midiron shots can begin, initially starting from hitting from a tee and progressing to normal hitting conditions. If successful, patients can then begin hitting with long irons and woods at 4 months and begin playing a full round of golf at 5 to 6 months after surgery if they are comfortable doing so.
Rehabilitation
The management of shoulder injuries in golfers always starts with an initial period of rest from golfing and consideration for using anti-inflammatory medication if indicated. It is critical to start a focused rehabilitation program, and the majority of golfers will see improvement. The tenets of the program are often based on the biomechanical and EMG studies previously described.16,17,21,32 For example, golfers with instability, especially posteriorly, should concentrate on strengthening scapular stabilizers, especially the serratus anterior muscle, which may become fatigued from overuse.13,21,30,32 In addition, those golfers with primarily anterior instability should focus on posterior capsular stretching and rotator cuff strengthening exercises, as well as including an anterior deltoid strengthening program. 32 The strengthening program is critical to help stabilize the scapula and protect the shoulder from further injury when it is placed in vulnerable positions during the golf swing. Those golfers with subacromial impingement and rotator cuff disease may benefit from a subacromial injection of corticosteroid and should also focus on rotator cuff strengthening. Moreover, it is important to closely evaluate the golf swing in these patients because swing modifications, such as shortening the back-swing or follow-through, or adjusting their grip on the club may prevent further injury.
Working with a certified golf teaching professional to change the mechanics of the swing and to address any swing flaws can be very helpful. Amateur golfers will often demonstrate poor swing techniques and may use adaptive maneuvers to compensate, which can place excessive strains on the shoulder girdle. Simple changes such as shortening the backswing or abbreviating the follow-through can diminish forces placed on the shoulder in these positions.3,18,38 Keeping the arms and hands in front of the body as much as possible during the swing may also limit the stresses applied to the shoulder. This adjustment can be facilitated by working on trunk, hip, and leg flexibility to help achieve the appropriate shoulder turn during the backswing. In addition, consideration should be given to limiting the number of practice balls hit at the range until the swing modifications and strengthening program have been comfortably adopted. Often, the golfer may continue with putting, chipping, and short game work while participating in a therapy program. Only when symptoms improve and rehabilitation goals have been met should the golfer progress to the full swing and gradually resume a normal practice routine.
A multidisciplinary approach employing the skills of a physiatrist, physical therapist, and teaching professional has been described 31 and reported to be highly effective in returning golfers to their previous level of play and in preventing further problems. This program included a comprehensive initial evaluation by a physician and physical therapist as well as a detailed swing analysis by a certified Professional Golf Association (PGA) teaching professional. After an initial period of rest, a program of flexibility, strength, and endurance training was emphasized. Ultrasound treatment was the most commonly used modality treatment. After injury treatment, swing modifications were essential for preventing further recurrence. It is important for the golfer to maintain a structured therapy program as well as to periodically monitor the golf swing mechanics to minimize the risk of future injury to the shoulder.
Experience from the PGA Tour and Senior PGA Tour has shown that golfers have benefited from a comprehensive, golf-specific exercise program.20,33 Specifically, a regimen consisting of (1) a daily flexibility and strengthening program, including not only shoulder exercises but also focusing on trunk, core, and lower extremity training; (2) a cardiovascular and aerobic conditioning program; and (3) a consistent, preround stretching and warm-up routine has become increasingly popular. Many professional golfers have attributed their increased driving distance, better endurance, and overall more consistent play to this improved fitness program. The advent of a mobile fitness trailer that travels to each tour event has enabled these players to more conveniently adhere to their maintenance exercise program.
Summary
Golf is a sport to be enjoyed at all ages. At first glance, it is not considered a strenuous activity, but as the frequency and level of play increases, more demands are placed on the golfer, and injuries can result from overuse. In particular, the shoulder is vulnerable to injury, especially the lead shoulder, or the left shoulder for the right-handed golfer. With a good understanding of the biomechanics and the forces involved in a golf swing, one can diagnose and treat the majority of shoulder injuries sustained by both recreational and elite-level golfers. Most will respond to nonsurgical treatment consisting of rest and a supervised physical therapy program. In addition to implementing a maintenance golf-specific exercise routine, sometimes a swing modification will not only help to prevent further injury but may also enhance the golfer's performance. Those few golfers who fail nonsurgical management can benefit from surgical intervention and will often be able to return to the same level of play.