
Abstract
Background: Secure tendon-to-bone fixation is essential for successful rotator cuff repair. Biomechanical properties of devices used in rotator cuff repair should be better understood.
Purpose: To evaluate the response to incremental cyclic loading of 6 different anchor-suture complexes commonly used in rotator cuff repair.
Study Design: Controlled laboratory study.
Methods: Two absorbable anchors 5 mm and 6.5 mm in diameter and 1 metallic anchor, coupled with Ethibond or FiberWire, were tested on 5 pairs of fresh-frozen human cadaveric shoulders. An incremental cyclic load was applied until failure using a Zwich-Roell Z010 electromechanical testing machine. The ultimate failure load and mode of failure were recorded. An analysis of variance model was used for statistical analysis.
Results: The FiberWire suture coupled with both absorbable and metallic anchors provided statistically significantly stronger fixation. However, although the metallic anchors in most cases failed because of slippage of the anchor, absorbable anchors failed because of rupture of the eyelet.
Conclusions: The FiberWire seems to increase the strength of fixation devices under cyclic load using both absorbable and metallic anchors, with relevant differences in failure mode (slippage of the metallic anchor and eyelet failure in the absorbable anchor).
Clinical Relevance: Use of the FiberWire suture might change the mode of failure of the suture-anchor complexes.
Rotator cuff tears are a common cause of shoulder pain and dysfunction. Chronic tears predominantly affect patients in the fifth and sixth decades of life. Acute tears can also affect younger people. The results of nonoperative treatment of complete tears are often disappointing, with inconsistent improvement of pain and residual muscle weakness. Surgical options include debridement, acromioplasty, and repair.2,7,10 The successful surgical reattachment of torn tendons to the humerus is the aim of reparable tear treatment. Recent studies have demonstrated the anchor-suture repair technique to be significantly stronger than the bone tunnel technique.5,9 Various anchors have been described and produced since their introduction in 1985. Today, metallic and absorbable anchors have reached an adequate design to provide easy insertion and management of arthroscopic suture techniques with 1 or 2 sutures. The initial ultimate tensile strength of the anchors was widely tested, but resistance to cyclic loading provides a better simulation of the in vivo condition of fatigue of the anchor-suture-tendon complex.1,5,11 The quality of the torn tendon, the arthroscopically assisted techniques of the suture, and the junction between the anchor eyelet and suture are possible weak points of this complex. Moreover, the first choice in arthroscopic rotator cuff suture material is actually a No. 2 nonabsorbable braided suture, with characteristics of easy handling (knotting) and good strength. To increase the resistance of the suture, a new polyblend suture has been introduced with the goal of reaching the strength of superior-diameter sutures. The aim of this study is 2-fold: (1) to evaluate the influence of the new polyblend suture on resistance to cyclic loading of metallic and resorbable anchors applied in the greater tuberosity of the human humeral head and (2) to measure the resistance to the cyclic loading of a wider resorbable anchor.
Materials and Methods
We used 6 pairs of fresh-frozen cadaveric shoulders (mean age at death, 72 years; range, 65–83 years), stored at 20°C. Each of the 12 specimens was thawed at room temperature for 24 hours; all soft tissue attachments were stripped, and the greater tuberosity was prepared by partially removing the cortical bone at the superior part of the greater tuberosity on an area adjacent to the cartilage. The humerus was securely fixed in a plastic cylinder with 2 Kirschner wires. The gap between the cylinder and the humeral bone was filled with acrylic cement. This stable system was then locked in a metallic cylinder and secured with wires and screws. The cylinder was attached to the base of the testing machine using a specially designed grip at 135° so that the suture anchors could be loaded in the anatomical direction of the supraspinatus tendon 11 (Figure 1).
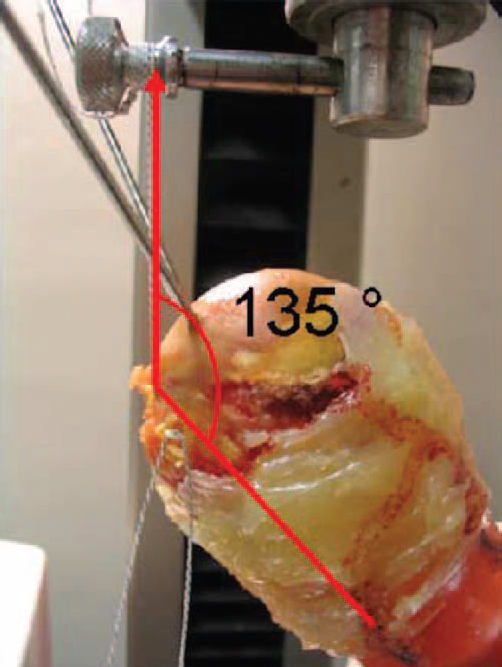
The angle between the diaphysis of the humerus and the pull direction.
From the anterior portion of the superior part of the greater tuberosity, close to the biceps tendon, we used 3 different insertion sites for the anchors: A, B, and C (Figure 2). Three different bone anchors were tested: 2 absorbable anchors of 5.0 mm and 6.5 mm, respectively (Bio-Corkscrew, Arthrex, Naples, Fla), and a metallic anchor of 5.0 mm (Corkscrew, Arthrex) (Figure 3). Coupled with the anchors, we tested 2 kinds of suture: Ethibond (Ethicon Inc, Johnson & Johnson, Somerville, NJ) and FiberWire (Arthrex). The order of introduction of the anchors into these 3 sites was regularly altered to avoid the influence of bone density at the various positions; therefore, each anchor was tested twice in the same position. The distance between the sites of insertion of the different anchors was at least 1.5 cm. Each anchor was inserted into the bone at an angle of 45° to the diaphysis of the humerus, as suggested by Burkhart, 4 such as in the surgical technique and similar to previous studies, 11 although recently some authors have shown no statistically significant differences in various angles of insertion. 8 We prepared the bone site insertion with the bone puncher of the corresponding anchor; moreover, before inserting absorbable anchors, a Biocork Tap (Arthrex) was used. Each shoulder was used to test the 3 different bone anchors with one suture, whereas the paired shoulder was tested with the other kind of suture. The anchors were introduced in the same site in each pair of shoulders.
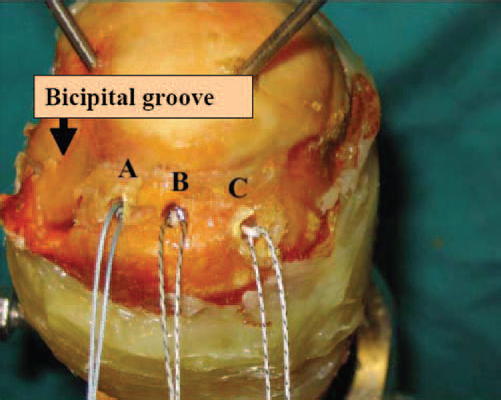
The 3 sites of the bone anchor insertions.
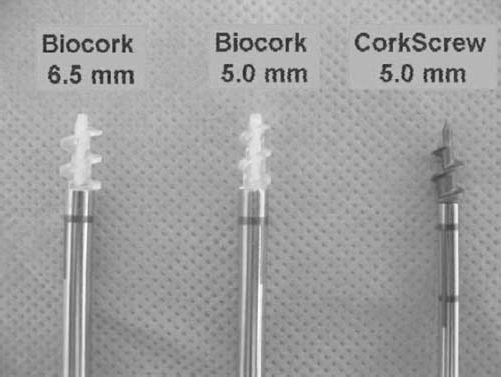
The 3 types of bone anchors tested.
To simulate the postoperative conditions, a cyclic loading was performed, similar to previous studies. 11 We set a preload of 20 N for 2 minutes; then we applied a cyclic loading, starting with a tensile load of 75 N for 50 cycles, with a crosshead extension rate of 20 mm/min. The tensile load was then increased by 25 N per 50 cycles until the failure of the anchor fixation system. The ultimate failure load (UFL), stiffness, and site and mode of failure (anchor slippage, loop of eyelet failure, and suture failure) were registered. The stiffness was calculated at the middle cycle of the second step of incremental load (the 25th cycle between 0 and 100 N) because it was reached in all tests using both Ethibond and FiberWire.
All of the tests were performed using an electromechanical testing machine (Zwick-Roell Z010, Zwick-Roell, Ulm, Germany). Data were recorded with dedicated software (Textexpert 8.1, Zwick-Roell) and evaluated with a load-displacement curve.
A statistical linear model was used to evaluate the conjoint effect of kind of suture and anchors, adjusting for site of insertion. An F test (analysis of variance) was used to test the statistical significance of the whole model and of the effects of each component of the device. The relative risk of slippage of the anchors using FiberWire was estimated for type of anchor (metallic vs absorbable).
Results
UFL and Stiffness
The mean UFL of the anchors coupled with Ethibond was 141 ± 14 N (range, 125–150 N) using the 5.0-mm Corkscrew, 150 ± 0 N using the 5.0-mm Bio-Corkscrew, and 133 ± 26 N (range, 125–175 N) using the 6.5-mm Bio-Corkscrew. In all tests, the UFL was never higher than 175 N.
The mean UFL of the anchors coupled with FiberWire was 245 ± 32 N (range, 225–300 N) using the 5.0-mm Corkscrew, 254 ± 33 N (range, 225–300 N) using the 5.0-mm Bio-Corkscrew, and 237 ± 14 N (range, 225–250 N) using the 6.5-mm Bio-Corkscrew. In 2 tests (using the 5.0-mm Bio-Corkscrew and 5.0-mm Corkscrew), the UFL reached 300 N.
The mean stiffness of the anchors coupled with Ethibond was 32 ± 8 N/mm (range, 15–33 N/mm) using the 5.0-mm Corkscrew, 29 ± 7 N/mm (range, 18–34 N/mm) using the 5.0-mm Bio-Corkscrew, and 31 ± 7 N/mm (range, 16–38 N/mm) using the 6.5-mm Bio-Corkscrew.
The mean stiffness of the anchors coupled with FiberWire was 56 ± 15 N/mm (range, 46–87 N/mm) using the 5.0-mm Corkscrew, 56 ± 14 N/mm (range, 46–84 N/mm) using the 5.0-mm Bio-Corkscrew, and 57 ± 19 N/mm (range, 40–86 N/mm) using the 6.5-mm Bio-Corkscrew.
Mode of Failure
We also evaluated the mode of failure for each test. In all tests with Ethibond, we observed the failure of the suture at a mean UFL of 141 ± 19 N. We never observed the slippage of the anchor or the failure of the loop of the anchor (eyelet).
In tests with FiberWire, we reached higher values of UFL, with a mean of 245 ± 27 N. Moreover, we found a different mode of failure between metallic and absorbable anchors: in all cases with the 5.0-mm Corkscrew, we observed the slippage and the migration of the anchors outside the bone tunnel at a mean of 245 ± 32 N (Figure 4), whereas using absorbable anchors we observed this mode of failure in only 2 cases (with the 5.0-mm Bio-Corkscrew and the 6.5-mm Bio-Corkscrew, both at an UFL of 225 N). In all the other 10 cases, we observed the failure of the eyelet of the anchors with a mean of 250 ± 26 N (Figure 5). We never observed the failure of the FiberWire suture.

Migration of the metallic anchor outside the bone tunnel.
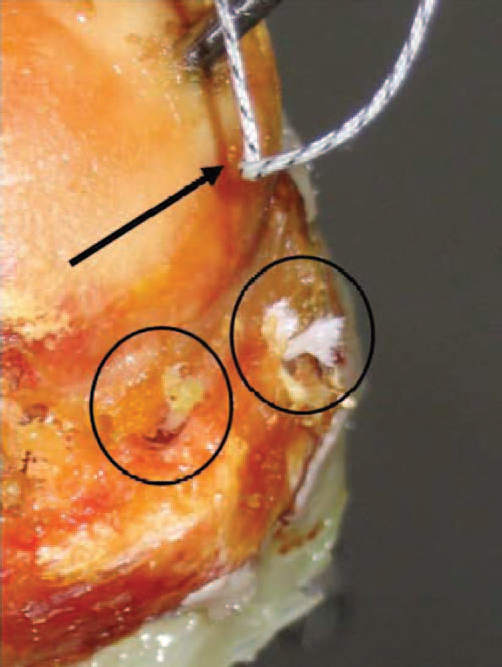
Failure of the loops of bioabsorbable anchors (6.5 mm and 5.0 mm) coupled with FiberWire (circled). It is possible to observe the FiberWire suture that did not fail (arrow).
The load-displacement curves of 2 tests with the Corkscrew coupled with either FiberWire or Ethibond are shown in Figures 6 and 7. Overall results are shown in Table 1.
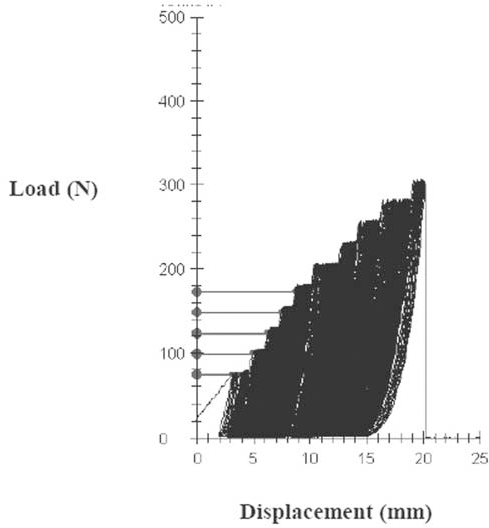
The load-displacement curve of a test of a Corkscrew anchor coupled with FiberWire.
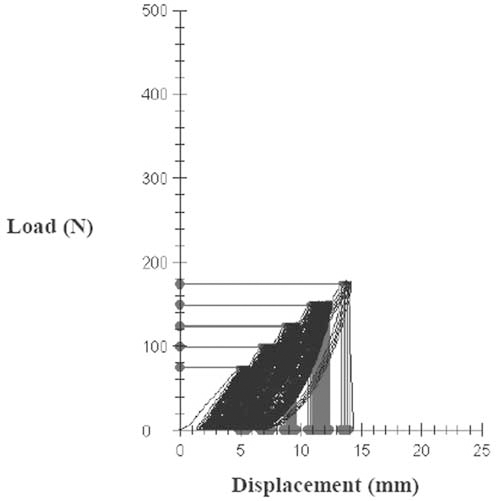
The load-displacement curve of a test of a Corkscrew anchor coupled with Ethibond.
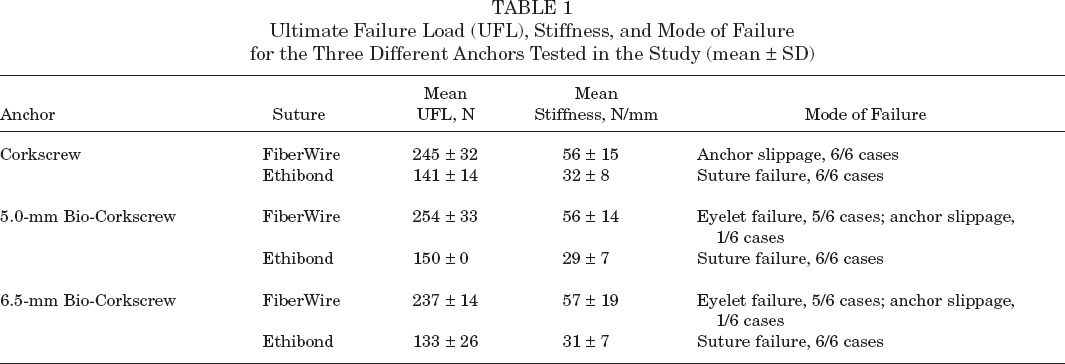
Ultimate Failure Load (UFL), Stiffness, and Mode of Failure for the Three Different Anchors Tested in the Study (mean ± SD)
Statistical Analysis
All the sutures with Ethibond failed because of suture failure, whereas sutures with FiberWire showed only anchor failure (slippage or eyelet failure).
The overall mean value of the UFL was 193.8 N. The difference among the sutures was remarkable (141.7 N for Ethibond vs 245.8 N for FiberWire; see Table 2), whereas anchors seemed to have similar values of mean UFL, from the highest value (202.1 N for the 5.0-mm Bio-Corkscrew) to the lowest (185.4 N for the 6.5-mm Bio-Corkscrew). Actually, means for each combination anchor suture showed that variability among the anchors is extremely low compared to variability among the sutures.
Mean Ultimate Failure Load Values of Different Sutures Coupled With the Anchors a
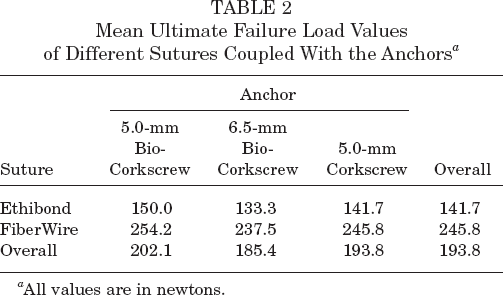
All values are in newtons.
The results for mean stiffness were similar to those for UFL: the difference seems to be important only for sutures (56.7 N/mm for FiberWire vs 31.2 N/mm for Ethibond) (Table 3).
Mean Stiffness Values of Different Sutures Coupled With the Anchors a
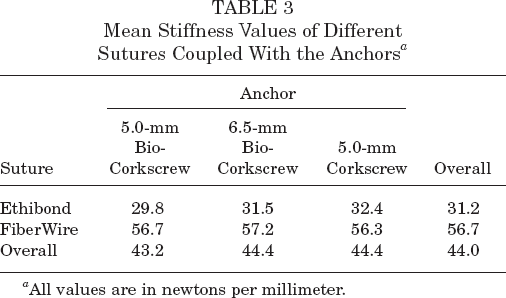
All values are in newtons per millimeter.
The linear model was estimated to take into account the variance effect of both factors (sutures and anchors). Site of insertion was considered to adjust for possible differences in bone density. Results of the model are reported in Table 4: the effect of the suture was statistically significant both for UFL and for stiffness (UFL: difference = 104.1 N, least squares difference = 14.5 N, P <. 001; stiffness: difference = 25.5 N, least squares difference = 13.9 N, P <. 01), whereas differences in response for the 3 anchors were not significant. FiberWire was estimated to increase both the resistance and the stiffness of the suture by at least 70% compared to Ethibond. On the other hand, mode of failure is to be considered in evaluating anchors used with FiberWire: each time the 5.0-mm Corkscrew was used, slippage of the anchor was observed, whereas for both types of Bio-Corkscrew, just 2 of 12 slippages occurred. The relative risk of slippage for the Corkscrew versus the Bio-Corkscrew was estimated to be 6.0 (P <. 01) (Tables 4 and 5).
Analysis of Variance: Results of the Model for UFL a
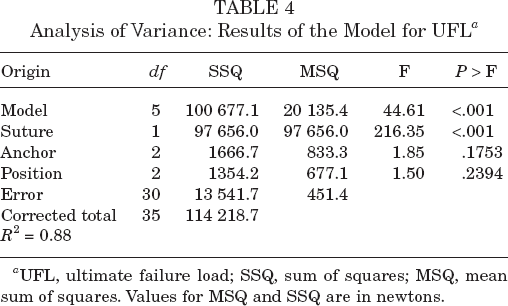
UFL, ultimate failure load; SSQ, sum of squares; MSQ, mean sum of squares. Values for MSQ and SSQ are in newtons.
Analysis of Variance: Results of the Model for Stiffness a
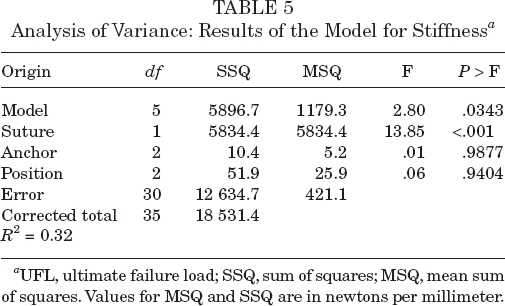
UFL, ultimate failure load; SSQ, sum of squares; MSQ, mean sum of squares. Values for MSQ and SSQ are in newtons per millimeter.
Discussion
Arthroscopic rotator cuff repair produces satisfactory results offering advantages such as a small incision, access to the glenohumeral joint, no need for detachment of the deltoid, and less soft tissue dissection. Several factors influence the arthroscopic repair: the kind of suture and anchor, the tendon suture technique 6 (simple or mattress), the insertion of the tendon to the greater tuberosity 5 (transosseous fixation or anchors fixation), and the angle of insertion of the anchors.3,4
Previous studies investigated the effect of single pull-out load on rotator cuff repair devices, 9 but this condition could not reproduce the load applied physiologically during shoulder movements. It is apparent that cyclic loading better represents the type of load to which the shoulder will be subjected after surgical treatment of rotator cuff tears.5,11 To achieve early passive range of motion, preventing postoperative stiffness, without the risk that “involuntary active” pendulum exercises (often observed among patients) might cause the failure of rotator cuff repair, suture anchor fixation should reach different goals:
high initial pull-out strength,
high UFL under cyclic loading, and
equilibrium between suture and anchor mechanical properties.
In fact, a weak suture coupled with a strong anchor will show a breakage of the suture itself, making useless the qualities of the anchor. On the other hand, a weak anchor coupled with a strong suture might cause an anchor slippage with failure of repair and loose bodies in the coracoacromial-humeral arch.
The development of new materials used for sutures yields substantial variations in response to different fixation devices to mechanical stresses. In this study, the Ethibond suture showed its weak point in the mechanical properties of the suture itself. In fact, in all cases failure occurred in the suture, at a mean UFL of 141 ± 19 N. No differences were shown between resorbable and metallic anchors in UFL or in the site of rupture.
The polyblend suture (FiberWire, Arthrex) showed significantly higher UFL (mean of 245 ± 27 N) and a different mechanism of failure: in all cases using the metallic screw, the strength of the suture caused the slippage of the anchor through the bone tunnel. In almost all bioabsorbable anchors, the weak point was the eyelet of the anchor. In any case, suture failure was observed.
Results of our study suggest the following:
The polyblend suture increases significantly the strength of fixation devices under cyclic load.
Bioabsorbable anchors coupled with FiberWire show UFL values similar to those of the metallic anchor and FiberWire combination, with important differences in the failure mode, which seems to suggest a safer use of absorbable devices in clinical applications to avoid metallic anchor slippage.
Future construction of a stronger eyelet of absorbable anchors might increase the UFL of the FiberWire-anchor complex.
There are no important differences in biomechanical evaluation between bioabsorbable anchors of the 2 different sizes tested in this study.
The first drawback of our study is that we could not evaluate the effect of the sutures on the tendons: it could be possible that a very stiff suture might cut the tendons, often of poor quality, to lower values of cyclic load than a weaker suture. Moreover, in vivo conditions of resorption of absorbable devices and modifications with time of mechanical response to load are still unclear. Further studies are needed to demonstrate that cadaveric studies and results can be applied to patients who undergo rotator cuff repair.