
Abstract
Background: Treatment of chronic, refractory biceps tendinitis remains controversial. The authors sought to evaluate clinical and functional outcomes of arthroscopic release of the long head of the biceps tendon.
Hypothesis: In specific cases of refractory biceps tendinitis, site-specific release of the long head of the biceps tendon may yield relief of pain and symptoms.
Study Design: Case series; Level of evidence, 4.
Methods: Fifty-four patients diagnosed with biceps tendinitis underwent arthroscopic release of the long head of the biceps tendon as an isolated procedure or as part of a concomitant shoulder procedure over a 2-year period. Patients were not excluded for concomitant shoulder abnormality, including degenerative joint disease, rotator cuff tears, Bankart lesions, or instability. Nine of 40 patients had an isolated arthroscopic release of the biceps tendon. At a minimum of 2 years, the American Shoulder and Elbow Surgeons; the University of California, Los Angeles; and the L'Insalata shoulder questionnaires as well as ipsilateral and contralateral metrics were used for evaluation.
Results: The L'Insalata; University of California, Los Angeles; and American Shoulder and Elbow Surgeons scores were 77.6, 27.6, and 75.6, respectively. Seventy percent had a Popeye sign at rest or during active elbow flexion; 82.7% of men and 36.5% of women had a positive Popeye sign (P < .05); 68% were rated as good, very good, or excellent. No patient reported arm pain at rest distally or proximally; 38% of patients complained of fatigue discomfort (soreness) isolated to the biceps muscle after resisted elbow flexion.
Conclusion: Arthroscopic release of the long head of the biceps tendon is an appropriate and reliable intervention for patients with chronic, refractory biceps tendinitis. Cosmetic deformity presenting as a positive Popeye sign and fatigue discomfort were the primary complaints.
Clinical Relevance: Although tenotomy is not the ideal intervention for patients of all ages with various shoulder abnormalities, data suggest that it may be an acceptable surgical intervention for a specifically selected cohort of individuals.
The treatment of chronic, refractory biceps tendinitis remains controversial. It is complicated by the uncertain function of the biceps tendon at the shoulder. Analysis using EMG has demonstrated the long head of the biceps tendon (LHBT) to be active during shoulder abduction and forward flexion. 1 In throwers, EMG studies have found that the biceps brachii serves primarily to position the shoulder and elbow, particularly during the early and late cocking stages of the pitching motion.12,13 However, Yamaguchi et al 37 found no significant increase in biceps brachii activity during isolated shoulder motion when the patient's elbow motion was controlled with a brace. They concluded that the LHBT does not play a significant role in either the rotator cuff–deficient or normal shoulder. Levy et al supported this finding in an EMG analysis of the LHBT in 10 shoulders, in which shoulder motion was isolated by using a long arm brace to lock the elbow in extension and the forearm in the neutral position. 19 They concluded that any hypothesis on bicipital activity at the shoulder must be measured with controlled elbow flexion or forearm activity, or be related to the inherent passive tension of the LHBT.
Historically, biceps tendinitis has been managed nonoperatively when possible. Rest, ice, nonsteroidal anti-inflammatory drugs, and physical therapy are generally advocated.28,30 If the patient does not respond to these treatment modalities, several authors have proposed local steroid injection into the LHBT sheath.9,28 If these modalities fail to relieve a patient's symptoms, a tenodesis has been promoted as the procedure of choice by many authors and has been performed for more than 50 years.7,10,14,20 This intervention is based on the observation that anterior shoulder pain secondary to biceps abnormality is attenuated when the LHBT is removed from its anatomical course over the humeral head and in the bicipital groove. Subsequently, other authors have performed this procedure both with and without subacromial decompression.2,3,6,8,23,25,30 However, the overall results are mixed and difficult to compare between studies. Moreover, a 6% to 40% incidence of unacceptable or poor results has been reported with tenodesis.3,7,8,23,25,30,34
Diagnosis of biceps tendinitis remains a clinical one. Standardization of diagnostic techniques and metrics is still limited. In specific cases in which physical examination is consistent with biceps pain and a diagnosis of biceps tendinitis has been attained, it is our belief that site-specific release of the LHBT may yield relief of pain and symptoms. In addition, it is our contention that biceps pain can be an isolated abnormality or part of a larger disease process such as the impingement syndrome. However, biceps symptoms can be isolated from other causes of shoulder pain, and treatments may be examined. The goal of this study was to evaluate the biceps clinically and functionally in a cohort of patients who underwent arthroscopic release of the LHBT with a minimum of 2 years of follow-up.
Materials and Methods
Fifty-four patients with a diagnosis of refractory biceps tendinitis and who had failed a course of conservative therapy underwent arthroscopic release of the LHBT between 1997 and 1999; all procedures were performed by the senior author. Forty patients were available for follow-up at a minimum of 2 years postoperatively. Patients who underwent concomitant shoulder procedures for instability, full-thickness rotator cuff tears, degenerative joint disease, labral tears, acromion abnormality, or adhesive capsulitis were not excluded from the study (Figures 1–3). Nine of the 40 patients had an isolated arthroscopic release of the biceps tendon (Table 1). Twenty-nine of the patients were men; the mean age of the patients was 48 years (range, 18–83 years). The source of symptoms was sports related in 6 patients, secondary to a motor vehicle accident in 1 patient, and of an unknown cause in 33 patients. The injury was reported to be acute in 15 of the patients and chronic in the remaining 25 patients. The distinction was based on whether the patient could recall a single event that initiated the pain within the past 30 days.
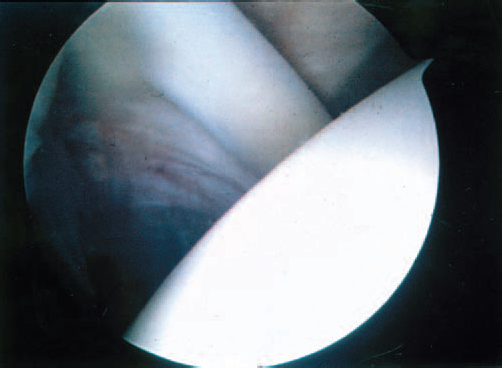
Arthroscopic view demonstrating a horizontal or flat biceps tendon with no mechanical advantage.

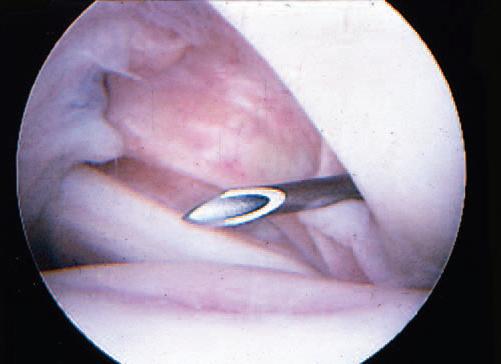
The active compression test was performed on this patient intraoperatively and demonstrated incarceration, reproducing the patient's mechanical symptoms.
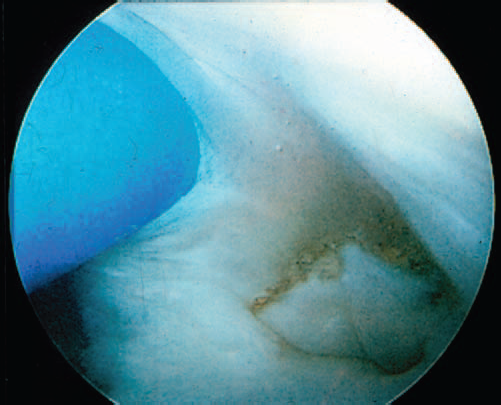
View demonstrating the chondromalacia of the humeral head due to the long head of the biceps tendon (LHBT) in a professional baseball player. The patient was given an LHBT tenotomy and returned to pain-free throwing 2 months postoperatively.
Breakdown of Concomitant Surgical Procedures
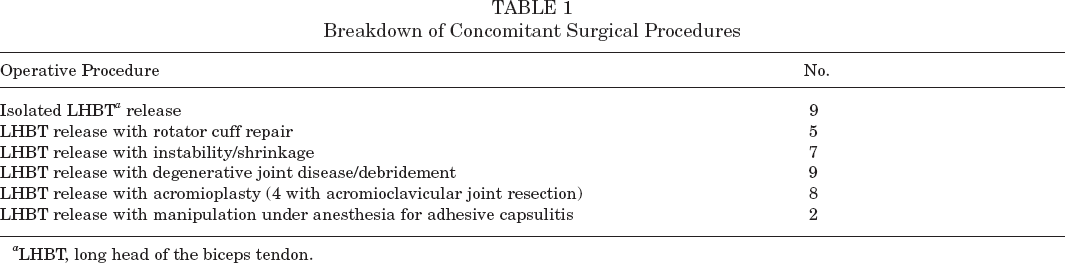
LHBT, long head of the biceps tendon.
The predominant symptom on initial presentation was pain (40). Additional manifestations included mechanical symptoms (16), clicking (7), and weakness (2). Seven patients complained of increased pain with overhead activity. Biceps tendinitis was diagnosed by the following algorithm: the patient reported a clinical history of pain in the intertubercular groove accompanied by tenderness on palpation of the groove during physical examination. These findings were frequently accompanied by some combination of the Speed, Yergason, and active compression tests. It is essential that the physical examination findings are correlated with the patient's history of symptoms. Twenty-three of 40 patients who were tested with an active compression test on initial examination had a positive sign by indicating deep pain on resisted flexion in internal rotation and relief of the pain on resisted flexion in external rotation. 24
At follow-up, the patients were evaluated clinically using the L'Insalata Shoulder Rating Questionnaire (100-point system), a physical examination that was scored using the American Shoulder and Elbow Surgeons (ASES) evaluation form (100-point system), and the University of California, Los Angeles (UCLA), shoulder evaluation test (35-point system). Patients also used a visual pain scale (0–10) and were asked to rate their overall satisfaction with the procedure at the time of follow-up. Patients were requested to complete a thorough physical examination of the upper extremity at our institution, performed by a single surgeon. Forty patients (74%) were available for clinical follow-up at a mean of 2.7 years postoperatively, with a maximum of 3.5 years and a minimum of 2.0 years. Furthermore, ipsilateral and contralateral metrics were evaluated. Patients were asked to perform isolated biceps curls with a 10-lb weight until fatigue with both the affected and contralateral arms. Patients were queried about fatigue discomfort symptoms and assessed for a Popeye sign (PS) with the elbow flexed and with the arm at the side.
Once completed, the L'Insalata questionnaire was scored according to the weighted system described. Similarly, once the physical examination was completed, the ASES questionnaire and the UCLA shoulder examination were scored. The data were then analyzed using standard methods. The data for the strength evaluation were examined using the Student t test. The data for the PS and the fatigue discomfort symptoms were analyzed by using the χ2 and Fisher exact tests.
Surgical Technique
The patient is first placed in the beach-chair position. A diagnostic shoulder arthroscopy is performed using the standard posterior portal for visualization and a superolateral portal for working. 18 The biceps anchor can be visualized when the arthroscope is placed through the superolateral portal. Tenotomy is performed arthroscopically by a simple resection as close as possible to the biceps stump at the superior labrum (Figure 4). At this time, the anterior and posterior glenoid labrum can be visualized and abnormality can be addressed. In our cohort, the surgical appearance of biceps tendinitis was varied. Common manifestations included chondromalacia of the humeral head, partial tear of the biceps tendon, synovitis (“lipstick sign”), incarceration with instability on examination, and hyper-mobility.
The distal portion of the tenotomized biceps tendon is usually situated at the edge of the glenohumeral joint postoperatively. Subsequently, this tendon may continue to slip distally, which may further contribute to the Popeye sign deformity.
Results
Forty patients were evaluated 2.7 years postoperatively (range, 24–42 months). The L'Insalata, UCLA, and ASES scores were 75.6, 27.6, and 77.6, respectively. Ranges were 29.1 to 100 (L'Insalata), 10 to 35 (UCLA), and 13.3 to 100 (ASES). Overall, 70% of patients had a PS at rest or during active elbow flexion. This was defined as any abnormal shortening or defect of the biceps muscle when the examiner compared it to the contralateral nonaffected side. Weight testing with the injured arm yielded a mean of 32.325 repetitions (range, 0-50 repetitions). Testing of the contralateral noninjured arm yielded a mean of 34.20 repetitions (range, 0-50 repetitions). Side-to-side strength difference was 1.88 repetitions (confidence interval, 0.3–3.5) with the 10-lb weight. This difference was statistically significant; however, none of the individuals older than 60 years had a difference in the number of repetitions that they were able to perform (P <. 03). The other age groups (individuals aged between 40–60 years and those younger than 40 years) thus accounted for the loss of strength that established the cumulative difference in strength between the injured arm and the contralateral side.
Overall, 68% of patients (27/40) were self-rated as good, very good, or excellent; 32% of patients were self-rated as fair (n = 6) or poor (n = 7). Of the 7 patients with a poor result, all had concomitant procedures. Three had grade 5 degenerative joint disease, 2 had rotator cuff tears, and 2 had an acromioplasty. Of these patients, 100% reported relief of arm pain at rest distally and proximally; 95% (38/40) reported relief of biceps tenderness on palpation of the bicipital groove; 37.5% (15/40) complained of fatigue discomfort (soreness) isolated to the biceps muscle after resisted elbow flexion. Of these 15 patients, 7 were younger than 40 years (7/11 in this age group), 8 were between the ages of 40 and 60 years (8/19 in this age group), and none were older than 60 years (0/10 in this group). This discrepancy represents a statistically significant difference between the age groups (P <. 01). In the group, 82.7% of the men (24/29) and 36.5% of the women (4/11) had a PS at rest, during elbow flexion, or during both, which was a statistically significant difference between the genders (P <. 02) (Table 2).
Results Breakdown by Gender and Age a
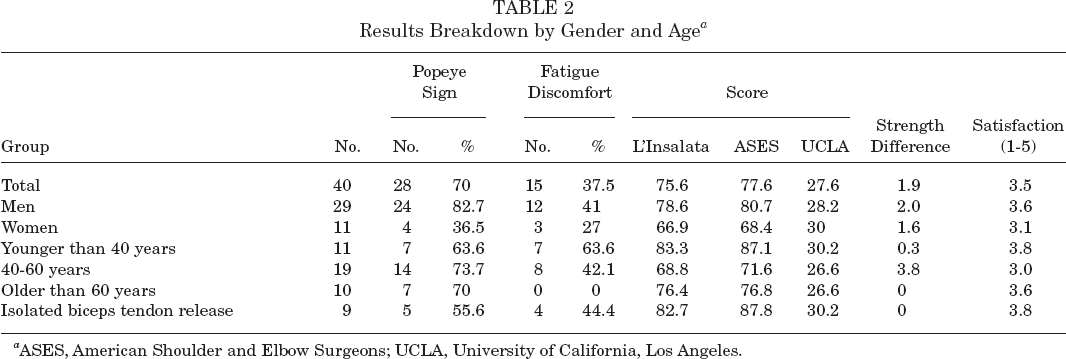
ASES, American Shoulder and Elbow Surgeons; UCLA, University of California, Los Angeles.
When an analysis of the isolated LHBT release group (9/40 total patients, all ages) was conducted, the mean L'Insalata, ASES, and UCLA scores were 82.7, 87.8, and 30.2, respectively. Nine of 11 reported good, very good, or excellent results. The 1 patient who reported poor results had grade 4 degenerative joint disease. Four (44%) reported fatigue discomfort symptoms (Table 2).
Discussion
Kumar et al reported that severing the LHBT can lead to a significant upward migration of the humeral head and a 5.1% decrease in the acromiohumeral interval. 17 They suggested that sacrifice of the intra-articular segment of the LHBT may produce instability and dysfunction. Warner and McMahon found superior migration of the humeral head with abduction in a study of 7 patients with isolated loss of the proximal attachment of the LHBT. 36 Others have confirmed the role of the LHBT in stabilizing the humeral head during abduction.15,17 Pagnani et al and Rodosky et al have suggested that the LHBT functions as a dynamic stabilizer to anterior translation.27,31 Sakurai et al 32 reported that not only is the LHBT a chief flexor of the elbow joint, but it is also a flexor and abductor of the shoulder joint and most likely a stabilizer of the humeral head.
Although the role of the LHBT has yet to be fully elucidated, most agree that the cause of LHBT abnormality may involve lesions within the tendon, specifically along its course in the bicipital groove or at its insertion on the labrum. Eakin et al classified LHBT abnormality into 3 categories: (1) biceps tendon degeneration (tendinitis), (2) origin disorders (superior labral anterior posterior lesions), and (3) tendon instability. 9 Tendon degeneration, more commonly known as biceps tendinitis, histologically results in collagen atrophy, tendon fissures, fibrinoid necrosis, and fibrocyte proliferation. 5 The predominant cause of LHBT tendinitis is thought to be secondary to mechanical irritation from the coracoacromial arch. 23 The LHBT, the rotator cuff, and the subacromial bursa fit compactly between the humeral head and the acromial arch, which includes the coracoacromial ligament, the acromioclavicular joint, and the acromion itself. Thus, lesions of the LHBT can be intimately related to abnormalities of the rotator cuff.21–23 In our cohort, 5 patients had concomitant rotator cuff tears that required surgical repair.
More recently, some authors have advocated tenotomy of the LHBT in specific patient groups.11,26,35 Several authors have reported that nonoperative treatment of spontaneous rupture of the LHBT yields good results.4,29,33 In addition, these authors reported relief of chronic biceps tendinitis symptoms subsequent to the rupture. Kempf et al have recommended LHBT tenotomy in elderly patients with significant biceps abnormality. 16 They reported on 210 patients with arthroscopically treated rotator cuff tears in which 18% had tenotomy of the LHBT. When compared with the nontenotomized group, the tenotomized group had statistically significant improvements in the level of physical activity, active mobility, and pain parameters.
Gill et al reported a series of 30 patients who had an arthroscopic biceps tendon release for treatment of bicipital tenosynovitis, dislocation, or partial rupture. In their study, 96.7% of patients did not require any pain medication at follow-up, 90% of the patients returned to their previous level of sports, and the mean ASES score was 81.8. 11
Our results with a minimum 2-year follow-up revealed a mean ASES score of 77.6, with 35% of patients with a poor result as defined by an ASES score <70. Our patient population contained several concomitant abnormalities that contributed to the patient's overall satisfaction and evaluation, as in the study of Gill et al. 11 However, the isolated LHBT release group had a mean ASES of 87.8, and a poor result was reported in only 1 patient (11%), secondary to severe grade 4 arthritis as evidenced by radiographic examination.
In our cohort, the loss of strength for biceps curls was minimal, and it was zero for individuals older than 60 years. Carroll and Hamilton reported on 75 cases of rupture of the LHBT that were treated nonoperatively. 4 In these cases, they reported no significant difference in the ability to lift weight when compared with the contralateral arm. Our series found that there was a statistically significant difference in number of biceps curls to fatigue in the older age group versus the younger age group when comparing the tenotomized arm with the contralateral arm. Similarly, none of the patients in the older age group (older than 60 years) complained of fatigue discomfort symptoms. This was also statistically significant when compared to the other age groups.
Cosmetic deformity presenting as a positive PS and fatigue discomfort during biceps curls were the primary complaints. Walch et al reported that many of their patients had little to no cosmetic deformity in the anterior arm in a series of patients with rotator cuff tears in which the LHBT was released. 35 Osbahr et al reported on the cosmetic appearance of tenotomy in 40 patients versus tenodesis in 40 patients. 26 The 2 patient groups were evaluated based on cosmetic appearance, muscle spasm, and anterior shoulder pain at 3 to 50 months of follow-up. The results revealed that there was no significant difference in the patients’ self-rated levels of anterior shoulder pain, cosmetic deformity, and muscle spasm between the 2 groups. The authors concluded that biceps tenotomy was a reasonable alternative to tenodesis in patients with refractive and chronic bicipital pain. Our results demonstrated a much higher incidence of PS (70%) and a statistically significant difference between male and female patients. Male patients had a statistically significant incidence in the development of the PS versus female patients. Osbahr et al 26 released the biceps proximally in the glenohumeral joint, which they surmised may lead to the LHBT becoming painlessly trapped in the bicipital groove and thus effectively becoming “auto-tenodesed.” In our cohort, we did not notice this “auto-tenodesis” phenomenon regularly.
Although many in our study cohort had concomitant diagnoses and procedures, we assert that pain on palpation of the bicipital groove can be attributed to the biceps tendon, particularly during overhead activities. Similarly, postoperative fatigue discomfort and the PS are 2 complications that can also be attributed to tenotomy. Based on our findings, arthroscopic release of the LHBT is an appropriate and reliable intervention for patients with chronic, refractory biceps tendinitis. The biceps tenotomy is a reliable alternative to tenodesis. This procedure is not advocated for heavy lifters (ie, physical laborers and football players) because of the 38% incidence of fatigue discomfort symptoms as well as the minimal strength difference, which has a higher incidence in younger populations. In this study, 100% of patients reported no pain isolated to the biceps muscle at rest, 95% of patients reported a significant decrease in biceps tendon pain, and 95% of patients reported a relief of tenderness on palpation of the bicipital groove. Although tenotomy is not the ideal intervention for patients of all ages with various shoulder abnormalities, it appears to be an acceptable surgical intervention for a specifically selected cohort of individuals, particularly in light of the decreased incidence of biceps tenderness when compared to tenodesis (unacceptable outcome in 6%–40% as noted in the literature).3,7,8,23,25,30,34