
Abstract
Background: The weakest points in hamstrings anterior cruciate ligament reconstruction are its points of fixation, especially on the tibial side. Methods for graft fixation to bone should be strong enough to avoid failure, stiff enough to restore load-displacement response, and secure enough to resist slippage under cyclic loading.
Hypothesis: Biomechanical properties of the interference screw can be improved by reinforcing the walls of the tunnel with a metal spiral (Evolgate fixation).
Study Design: Controlled laboratory study.
Methods: Three paired tests were performed using common digital extensor bovine tendons fixed to porcine tibias with interference screw, Intrafix, and Evolgate; critical graft fixation conditions were simulated by applying subsequent cycles to the graft before loading the graft until failure.
Results: The strength, stiffness, and resistance to slippage of the Evolgate were significantly higher than those of the interference screw; the ultimate failure load of the Evolgate was significantly higher than that of the Intrafix (1058 ± 130 N and 832 ± 156 N, respectively; P = .02). No statistically significant differences were found between Evolgate and Intrafix regarding the stiffness and slippage under cyclic load.
Conclusion: Evolgate fixation seems to be stronger, stiffer, and more resistant to slippage than is interference screw fixation of similar length, and it is stronger but not stiffer than Intrafix.
Clinical Relevance: The Evolgate provides structural properties that seem to be appropriate for an intensive rehabilitation after anterior cruciate ligament reconstruction using a doubled semitendinosus and gracilis graft.
The use of hamstring tendon grafts is becoming widespread for ACL reconstruction, largely because a multistrand graft has adequate strength and because it avoids extensor mechanism problems associated with patellar tendon harvest. Unfortunately, the fixation of tendon to bone has been considered by several authors1,18,19 to be less secure than is fixation using a bone plug. In particular, the tibial fixation of a doubled semitendinosus-gracilis graft is considered the weak point of the ACL reconstruction with hamstring tendons. In the past few years, many methods of doubled semitendinosus-gracilis graft fixation to tibia have been described and tested.12,13 In previous articles,3,5 some of us have described the Evolgate, a method that was demonstrated to improve the pull-out strength of the interference screw in tibial fixation of a doubled semitendinosus-gracilis graft. However, it is necessary for the tibial fixation device to have not only a high initial pull-out strength but also superior fatigue characteristics because various degrees of forces are repetitively applied to the graft during daily and rehabilitation activities after ACL reconstruction. The purpose of this study was to biomechanically evaluate the Evolgate fixation of the doubled flexor tendons using cyclic elongation in comparison to a conventional fixation method of an interference screw of the same length, which provides a similar, not true anatomical, fixation of the tendons inside the tibial tunnel. Moreover, because in a recent study by Kousa et al 12 the Intrafix was shown to have the highest strength under pullout and after cyclic loading, and less slippage under cyclic loading in comparison to several fixation devices, we also biomechanically compared the Evolgate and the Intrafix using cyclic loading with final pull-out tests.
Materials and Methods
The Evolgate
The Evolgate (Citieffe, Bologna, Italy) is composed of 3 components, all made of a titanium alloy: an involute (a sort of spiral, 21 mm in length, 10 mm in diameter), with a spike positioned at one extremity; a screw, 9 × 20 mm; and a washer (Figure 1). The coil (involute) reinforces the walls of the distal half of the tibial tunnel, the screw interferes with the tendons and the involute, and the washer provides a cortical grip (Figure 2). The coil is inserted into the tibial tunnel with a special impactor (also acting as an extractor should a revision be necessary), which also provides penetration of the spike in the predrilled tibial cortex. The tendons, secured at the femoral side, are pulled through the bone tunnel, and the 4 ends of the tendons, coming out from the tibial side, are properly tensioned; as the 4 bundles are kept separate, the screw is then inserted in the middle (Figure 3), interfering with the tendons and the spiral, until the washer leans against the tibial cortex. The spike prevents rotation of the spiral as the screw tightens.

The Evolgate is composed of 3 components, all made of a titanium alloy. On the left is the involute with a spike positioned at one extremity; on the right is the screw with the washer on top.
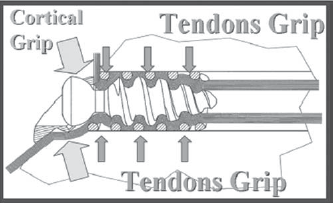
Explanation of how the Evolgate works.

An in vivo image of the Evolgate inserted inside the coil, through the tendons.
Intrafix
The Intrafix ACL Tibial Fastener (Mitek, Ethicon, Norwood, Mass) is a polyethylene screw and sheath system designed to provide intratunnel tibial fixation for soft tissue grafts. The Sheath Trial (Innovasive Devices Inc, Marlborough, Mass) was inserted into the 4 bundles of the tendons, compressing the tendons while preparing the bone tunnel for the Intrafix sheath, which was inserted into the Sheath Trial, so each tendon bundle was uniformly compressed against bone walls. Once the looped end of the graft and the tibia were secured on the testing machine, the sutures extending from each of the 4 free ends of the gracilis and semitendinosus tendons were tied together and looped over the arms of a Tie Tensioner (Innovasive Devices Inc). While the Tie Tensioner was pulled distally to equalize the tendons, the Sheath Trial was first gently tapped with a mallet to separate the tendons, and then the Intrafix sheath was inserted into the tibial tunnel. Finally, an 8- to 10-mm-diameter Intrafix tapered screw (Innovasive Devices) was inserted into the sheath.
Interference Screw
The interference screw was a titanium, fully threaded, soft tissue interference screw, 9 × 25 mm (Stryker Endoscopy, San Jose, Calif).
Biomechanical Tests
Fifteen pairs of double-looped bovine digital extensor tendons were harvested from 12- to 18-month-old bovines and were used for our tests. The bifurcated tendon has the form of a Y, so it is possible to divide it into halves by cutting the long arm (the lower) of the Y along its axis. A double-looped bovine tendon graft was prepared by placing the 2 tendons side by side and folding them in half, achieving a 4-strand graft. The tendon grafts were prepared following a standard surgical protocol until the graft passed through a 9-mm-diameter cylinder. A No.1 suture was used to sew 4 cm of both ends of each tendon using a crisscrossing stitch. Porcine tibias were used in this study because they are readily available, are inexpensive, and have been used in previous studies similar to this one.15,16 Twenty porcine tibias were prepared by removing all soft tissues and by drilling a tibial tunnel that was 9 mm in diameter and 45 mm in length using a commercially available tibial guide for ACL reconstruction. The tibia, securely fixed in a metal cylinder, was attached to the base of the testing machine using a custom-designed fixture that allowed the tibial tunnel and graft to be loaded in alignment with the motion axis of the actuator. The tendons were wrapped around a rigid bar attached to the upper portion of the materials testing machine, pulled through the tibial tunnel, properly tensioned, and fixed to the tibia using one of the selected devices. The distance from the bar to the articular surface of the tibia was kept at 5 cm to replicate the length of the intra-articular portion of the graft (3 cm) and the section within the femoral tunnel (Figure 4). All tests were performed using an electromechanical testing machine sensitive and accurate enough to measure to 0.001 mm (Z010, Zwick Roell GmbH & Co, Ulm, Germany), which sent the data to a personal computer, where these data were analyzed using a dedicated software (Text Expert 8.1, Zwick Roell GmbH & Co). Results were statistically evaluated using a Student paired t test.
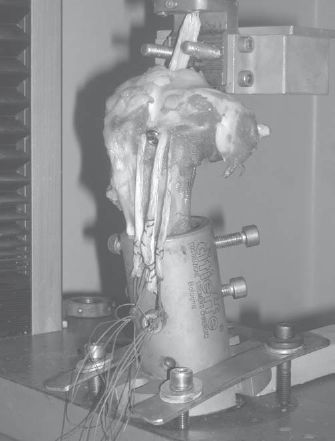
Complete testing setup.
Test 1: Evolgate versus Interference Screw
After the tendons were preloaded for 2 minutes at 20 N, 2 paired tests were performed using 5 pairs of tendons for each test. The same tibia was used in each paired test so the comparison would not be invalidated by a difference in bone density between specimens; the interference screw was always tested first, and the Evolgate was always tested second to avoid any disturbance in the test performed with the interference screw. The same tibial tunnel of the same tibia was enlarged for the distal 20 mm of its length, to perform the same test on the paired grafts fixed to the tibia using the Evolgate.
Test 1A (5 pairs)
Cyclic Test to Constant Load
Behavior under cyclic loading was first tested by load cycles between 0 and 150 N with a crosshead speed of 300 mm/min, giving a loading frequency of approximately 35 cycles per minute. The crosshead position was noted at peak load after 1, 100, 300, and 1100 load cycles following the protocol suggested by Giurea et al. 8
Test 1B (5 pairs)
Cyclic Test to 50-N Increments Load
This test was done according to the protocol suggested by Magen et al. 14 Ultimate strength and slippage of the graft fixation method–tibia complex were determined using additional grafts and tibias by applying progressively higher loads (in 50-N increments) under load control for subsequent cycles until failure. Computed as the difference between the length after each complete loading cycle (at 10 N of load) and the original length (at 10 N of load), the residual displacement measured the combined effects of tendon graft stretch and fixation slippage. Fixation slippage was the primary cause of any differences in length between fixation methods because graft stretch was assumed to be constant at a specific load. Slippage was compared at 250 and 500 N of load within the elastic region and was well below the failure load of the double-looped bovine tendon. Mode of failure and ultimate failure load (UFL) were recorded for each test.
Test 2: Evolgate versus Intrafix
Five pairs of double-looped bovine digital extensor tendons and 5 pairs of porcine tibias were used, so the devices were tested in different but paired tibias. The bone tunnel diameter was 9 mm for both the Evolgate and Intrafix. A 50-N preload was first applied to the specimens for 10 seconds. Thereafter, the graft fixation constructs were loaded for 1500 loading cycles between 50 and 200 N at a frequency of 1 cycle every 2 seconds, according to the protocol suggested by Kousa et al. 12 The loading was parallel to the long axis of the femoral tunnel. The response to loading was automatically obtained in the form of an X-Y load-displacement curve. We evaluated the displacement at 1, 10, 100, 250, 500, 1000, and 1500 cycles. After 1500 loading cycles, a single-cycle load-to-failure test was conducted on the surviving specimens, and the stiffness was calculated on this curve.
Results
Test 1A: Cyclic Test to Constant Load at 150 N
Only 1 of the interference screw constructs survived 1100 cycles, and it had an elongation of 22.2 mm. Only 2 resisted to 300 cycles with an elongation of 20.1 mm and 41.7 mm, respectively. The mean elongation of the 5 constructs resisting to 100 cycles was 28.3 mm. The mean elongation after 1 cycle was 7.1 mm. All the specimens fixed with the Evolgate resisted to 1100 cycles with an ultimate mean elongation of 3.2 mm; the mean elongation at 300 cycles, 100 cycles, and 1 cycle was 2.2 mm, 1.6 mm, and 0.4 mm, respectively.
Test 1B: Loading Cycles in 50-N Increments
The UFL was 400 ± 93 N for the interference screw and 1314 ± 217 N for the Evolgate (P <. 001); the mean stiffness of the graft fixation–tibia complexes was 122 ± 13 N/mm for the interference screw and 269 ± 15 N/mm for the Evolgate (P <. 05). The mean stiffness of the fixation method calculated as suggested by Magen et al 14 was 156 N/mm for the interference screw and 320 N/mm for the Evolgate (P <. 05). The mean slippage at 250 N was 0.7 ± 0.1 mm for the interference screw and 0.154 ± 0.01 mm for the Evolgate (P <. 05). Four of 5 of the grafts fixed with the interference screw failed to reach to 500 N, whereas the mean slippage of the cases fixed with the Evolgate was 0.24 ± 0.04 mm.
In all cases, failure occurred owing to partial breaking and then slipping of the tendons from the site of fixation. Results are summarized in Table 1. Load-displacement curves of tests 1A and 1B are shown in Figures 5 and 6, respectively.
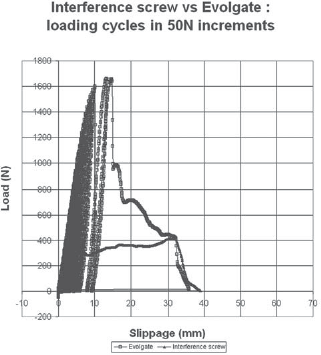
An example of the load-displacement curve of test 1B.
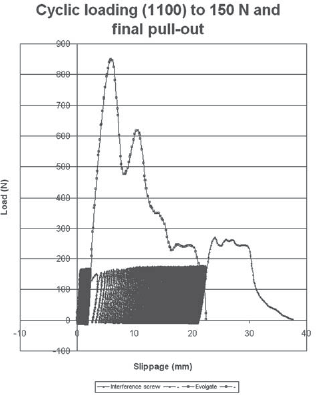
An example of the load-displacement curve of test 1A.
Evolgate Versus Interference Screw: Tests 1A and 1B a
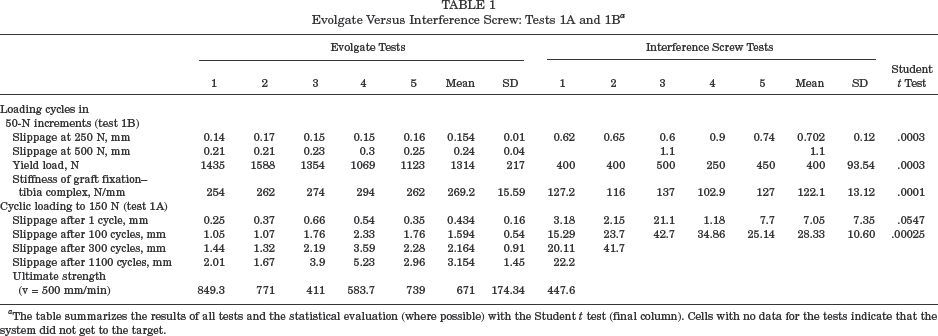
The table summarizes the results of all tests and the statistical evaluation (where possible) with the Student t test (final column). Cells with no data for the tests indicate that the system did not get to the target.
Test 2
There was no statistically significant difference in the slippage at each cycle level. The mean UFL at pullout after 1500 cycles was 832 ± 156 N for Intrafix and 1058 ± 130 N for the Evolgate (P <. 05). The mean stiffness at pullout was 269 ± 86 N/mm for the Intrafix and 247 ± 44 N/mm for the Evolgate, and this difference was not statistically significant (P >. 05). Results are summarized in Table 2. The load-displacement curve of test 2 is shown in Figure 7.
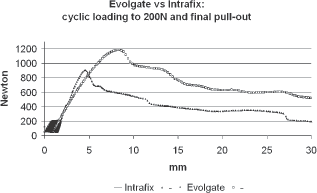
An example of the load-displacement curve of test 2.
Intrafix Versus Evolgate: Test 2 a
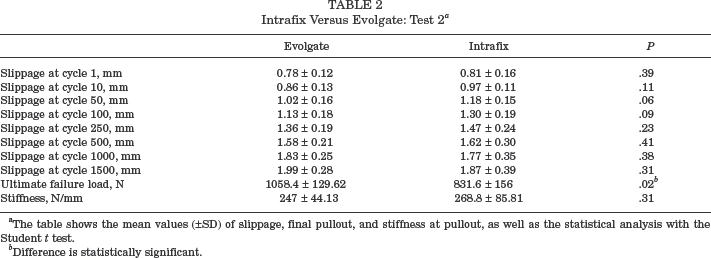
The table shows the mean values (±SD) of slippage, final pullout, and stiffness at pullout, as well as the statistical analysis with the Student t test.
Difference is statistically significant.
Discussion
Before discussing the findings from this study, a critical examination of the experimental apparatus is warranted to determine how the methods may have affected the interpretation of the results.
The first limitation of this study is that we used an animal model. Human cadaveric specimens may be the best possible model, if sufficient numbers of fresh-frozen specimens can be obtained that are harvested from young and healthy donors. However, the mechanical properties of the available human bone and tendon specimens are extremely varied, depending on many factors, including age, nutrition, and mechanical environment at the time of donation. Bovine tendons were used because the stiffness and viscoelastic behavior are not significantly different from a human doubled semitendinosus-gracilis tendon. 5 Porcine tibias were used because it has been demonstrated that the average density of porcine bone is similar to that of young human bone and significantly higher than that of elderly human cadaveric bone specimens.2,4,7,21 Therefore, we believe that the models used in this study, bovine tendons and porcine tibias, are useful for biomechanical comparison of ACL reconstruction procedures.
The second limitation is that we stretched the graft along the tunnel axis to apply cyclic elongation to the graft. Therefore, we could not obtain direct information on flexion-extension motion of the knee from this study. However, we may be unable to clarify the effect of cyclic tensile load in repetitive flexion-extension motion on biomechanical properties of the fixation site by an ex vivo study, as Graf et al 9 have reported that repetitive flexion-extension motion of the knee after ACL reconstruction resulted in a rupture of the autograft at the bone tunnel due to wear-related damage. The loading conditions of the present study can clarify the effect of cyclic elongation on the site of tibial fixation without the effect of wear-related damage to the graft.
Tohyama and Yasuda 19 demonstrated that fatigue properties of the soft tissue fixation site in ACL reconstruction do not always correspond to the failure load before cyclic loading. It is our opinion, therefore, that cyclic loading should always be a part of the evaluation of soft tissue reconstruction strength and that the ultimate strength is of limited value.
The first aim of this study was to evaluate the load elongation behavior of the hamstring tendons fixed to the tibia with the Evolgate during cyclic elongation in comparison with the interference screw. In a previous preliminary biomechanical study on the Evolgate, only the pull-out strength of the device was evaluated in comparison with an interference screw, resulting in a significantly higher strength.3,5 However, the reliability of a tibial fixation device is based more on the fatigue characteristics than on the initial pull-out strength. In this article, we have conducted a more extensive biomechanical test on the behavior of the Evolgate under both incremental and constant cyclic loading, which much more closely mimics the forces applied to the tendon device–bone complex in the postoperative period, especially if an accelerated rehabilitation is performed. Therefore, structural properties such as stiffness and slippage were included in our study, in addition to the previously studied pull-out strength,3,5 because each may affect the ability of a ligament replacement to restore and maintain stability of the reconstructed knee, especially during intensive rehabilitation.6,13
This study showed that cyclic elongation much more rapidly relaxed the flexor tendon graft when fixed to the tibia with the interference screw compared to when fixed to the tibia with the Evolgate. Our results also suggested that although the interference screw fixation allows progressive slippage of the tendons until failure, the fixation with the Evolgate allows only 2.16-mm elongation within the first few hundred load cycles, perhaps due to the tendon “bedding in” at the point of fixation. This process may include realignment of tendon fibers adjacent to the device or crushing of bone trabeculae at the point of stress concentration. In subsequent cycles up to the end of the test, the fixation with the Evolgate became very stable, allowing only minimal elongation and/or slippage of the graft. These findings clearly indicate the benefit of performing a number of knee-motion and loading cycles at operation, allowing the graft to be retensioned to recover the initial elongation before final graft fixation.
Secure graft fixation is important to the success of ACL reconstruction. The goal of the graft fixation is to prevent stretching or failure at graft fixation sites, allowing early motion and weightbearing without loss of stability. Any fixation method with poor biomechanical properties has the potential to compromise the clinical outcome, especially if an accelerated rehabilitation protocol is used in the early postoperative period. Assuming that during daily activities and accelerated rehabilitation the loads in the ACL should be about 20% of its failure capacity, it seems reasonable to consider that a fixation method should be as stiff as the normal ACL is and should function to loads of at least 500 N if a reconstructed knee is to be intensively rehabilitated.
Although several devices are now available for tibial fixation of the doubled semitendinosus-gracilis graft, in this study using bovine tendons, the Evolgate was compared with a very popular method for tibial fixation in ACL reconstruction with a doubled semitendinosus-gracilis graft, the interference screw, and with Intrafix, which is considered one of the strongest devices. We chose the interference screw because it is one of the more commonly used fixation devices in biomechanical studies. We did not use a screw combined with a staple or screw post because we compared a single-fixation device against another single-fixation device (and not double as interference screw plus staple), following previous works.12,14
Although several tests were performed with the interference screw, in test 1 it failed after fewer than 300 cycles or at a pullout of less than 500 N; all the tests performed using the Evolgate resisted up to 1100 cycles and to an ultimate pull-out strength of more than 500 N, which is considered the minimum requirement for a suitable ACL fixation device. 13
In test 1, the same bone and tunnel for each pair of tendons were used to avoid any difference in bone tunnel positioning and length and in bone density between specimens. The interference screw was always tested first, and the Evolgate was always tested second to avoid any disturbance in the test performed with the interference screw. Using a new bone and tunnel for the Evolgate possibly could have increased the strength of the Evolgate. It has been previously shown that increasing screw length improves fixation strength more than oversizing the screw diameter does.11,16,20 Moreover, the biomechanics of the interference screw fixation also could be improved significantly if the screw head engages the graft against the tibial cortex. 10
In our study, we used a screw that was 25 mm in length and 9 mm in diameter to obtain an acceptable performance from the interference screw fixation method, which was used as the control group. At this time, some surgeons size the bone tunnels in relationship to the graft diameter for interference screw fixation. We used a standardized protocol12,14 to better compare the 2 fixation devices. However, using screws of different diameters in relationship to the graft diameter could increase the pull-out strength of both methods.
The level of the fixation inside the tunnel might influence the stiffness of the graft.11,16,20 In our study, although the point of fixation level was slightly more proximal in the interference screw group, the stiffness was significantly greater in the Evolgate group. Similar to the interference screw, the Evolgate provides a nearly anatomical graft fixation close to the original ACL insertion site 7 (not true aperture fixation), which is preferable as compared with the devices that fix the tendons outside the tibial tunnel (suspended fixation). By fixing the tendons deep in the tibial tunnel, a secure fixation can be obtained even in cases in which the tendons (especially the gracilis) are very short or are accidentally cut during stripping. The interference between the screw and the involute never caused abrasion of the tendons; they always failed out of the involute.
However, although the Evolgate provides fixation of the graft deep into the tibial tunnel, as do the interference screws, it is not completely recessed inside the tunnel because the washer lies on the tibial cortex; therefore, it should be considered as a low-prominent rather than a low-profile fixation device.
The second aim of this study was to evaluate the UFL, the stiffness, and the load elongation behavior of the hamstring tendons fixed to the tibia with the Evolgate during cyclic elongation with final pullout, in comparison with the Intrafix, using coupled porcine tibia and a bone tunnel of 9-mm diameter for both the Evolgate and the Intrafix (an 8- to 10-mm tapered screw was used). The analysis of the results confirmed the very good biomechanical properties of these 2 devices. The statistical analysis showed that there is a significant difference between the Evolgate and the Intrafix only in the pull-out strength after 1500 cycles. In the study of Kousa et al, 12 the mean strength of the Intrafix, at single-cycle pullout and at pullout after 1500 cycles, was 1332 N and 1309 N, respectively. It is surprising how the pullout after 1500 cycles did not decrease in comparison to the single-cycle load-to-failure test. In our study, perhaps the mean strength was lower because we used bovine tendons instead of human tendons. However, in a previous study 5 we tested the Evolgate under single-cycle pullout using human tendons, and the mean strength was 1237 N, near to the value of the study by Kousa et al. 12
In an attempt to explain the difference between the Intrafix and the Evolgate, it could be interesting to better explain how the 2 devices work.
Whereas the Evolgate has a metal spiral inside the tibial tunnel that reinforces the walls of the tunnel to avoid the loss of fixation strength related to the low density of the cancellous bone of the proximal epiphysis of the tibia, the Intrafix optimizes the properties of the screw by the use of the Sheath Trial and the Intrafix sheath, which allow a uniform compression of each tendon and avoid the divergence between the screw and the graft. We used an 8-to 10-mm tapered screw with a 9-mm-diameter bone tunnel in the Intrafix fixation, as suggested by the product brochure for surgical technique, to optimize the properties of the device. However, the Intrafix, similar to an interference screw of the same length, purchases only in the cancellous bone, which could vary in density between tissue sources. Therefore, the properties of the Evolgate could be more independent from the quality of the cancellous bone than are those of the Intrafix. The 2 devices differ in their materials, lengths, and shapes: the Evolgate provides fixation of the graft deep into the tibial tunnel, as does the Intrafix, but it is not completely recessed inside the tunnel because the washer lies on the tibial cortex. One of the advantages of the Intrafix is that it compresses the tendons uniformly against the walls of the tibial tunnel, providing a wide area of bone-to-tendon interface. In the Evolgate fixation, a relatively small area of the tendons (about one quarter of the distal half of the tibial tunnel) is surrounded by metal work. Moreover, the Evolgate and the Intrafix differ significantly in length, as the Intrafix is longer than is the Evolgate, which occupies only about one half of the tibial tunnel length. How those differences could influence the bone ingrowth and final tendon-bone healing should be determined.
Caution should be used in extrapolating the results of our study to clinical estimates, as we cannot assume that the structural properties of fixation devices determined in animal tissue and laboratory studies predict its performance in human knees. Interference screw fixation, for example, performed significantly worse in human tissue compared with animal tissue, probably because the interference screw purchases only in cancellous bone, which could vary in density between tissue sources.17,20
In conclusion, on the basis of this biomechanical study, the Evolgate fixation seems to be stronger, stiffer, and more resistant to slippage than is interference screw fixation of similar length in the immediate postoperative period. Moreover, in the cyclic loading test, it exhibited similar slippage to that of the Intrafix, but it seemed to be stronger in providing structural properties that may be appropriate for a more intensive rehabilitation.