
Abstract
Background: Although stress radiography has been recommended for quantifying posterior tibial displacement in knees with posterior cruciate ligament insufficiency, the intratester reliability and intertester reliability of this measurement method have not been evaluated.
Hypothesis: Stress radiography is a reproducible measurement method in the assessment of posterior knee laxity in patients with posterior cruciate ligament lesions.
Study Design: Cohort study (diagnosis); Level of evidence, 2
Methods: Stress radiographs of 787 patients with suspected posterior cruciate ligament lesions taken using the Telos device were evaluated independently by 3 testers: 2 of the testers were clinically experienced in the evaluation of stress radiographs, and 1 tester was a novice tester. Change in mean, standard error of measurement with calculated confidence intervals, and intraclass correlation coefficients were determined to assess intratester and intertester reliability.
Results: There was no significant intratester change in mean. Intratester standard error of measurement was 1.03 mm; 95% confidence intervals were ±2.02 mm for a single measurement and ±2.86 mm for a change in measurement. The intratester intraclass correlation coefficient was 0.95. Intertester reliability revealed a significant change in mean between the experienced testers and the novice tester (P < .001). There was no substantial difference for the standard error of measurement of each tester. The mean intertester standard error of measurement was 1.41 mm; 95% confidence intervals were ±2.77 mm for a single measurement and ±3.91 mm for a change in measurement. The intertester intraclass correlation coefficient was 0.91.
Conclusion: Stress radiography was found to be a measurement method with a useful reliability for evaluation of posterior laxity in patients with posterior cruciate ligament lesions. The reproducibility of stress radiography may be influenced by multiple variables, and standardized methods are needed to minimize measurement error.
Knee ligament injuries have become one of the most intensively studied areas in the field of orthopaedics. However, the volume of literature devoted to the study of the ACL has far exceeded the study of the PCL. 3 Although more information has become available with respect to the anatomy and biomechanics of the PCL, many variables and controversies regarding diagnosis and treatment options still persist.3,7,16 Despite numerous clinical tests that have been described for diagnosing PCL insufficiency, objective clinical quantification of posterior laxity remains difficult, and the diagnosis is often missed at initial evaluation.1,4,7,15,17 Both arthrometer testing and stress radiography have been used to quantify the amount of tibial translation on the femur in knees with PCL lesions.2,5,8,11,14,18,20 Although stress radiography has been recommended by some authors to quantify posterior tibial displacement (PTD),8,14 the reliability of this measurement method has not been evaluated in a larger patient population. However, knowledge of the precision of a measurement method is paramount to monitor small but clinically important changes in an individual patient over time. 9 The purpose of this study was to assess intratester and intertester reliability of stress radiography in 90° of flexion using the Telos device in quantifying PTD in patients with PCL insufficiency.
Materials and Methods
Subjects
Between September 1996 and July 2003, 1163 patients with a suspected PCL injury were evaluated at our institution. Diagnosis was established through a detailed history coupled with a thorough clinical examination. The posterior drawer test, which included palpation of the tibial step-off, and the posterior sag test (Godfrey test) were used for clinical examination of the PCL. These test are considered the most sensitive tests for diagnosing PCL insufficiency.1,16,17 Assessment of the posterolateral structures was done with the tibial external rotation (dial) test in the prone position and the posterolateral external rotation test.13,21 With a suspected injury to the PCL based on history and clinical examination, posterior stress radiographs were obtained to quantify PTD. General inclusion criteria for this study included (1) a suspected PCL tear based on clinical examination, (2) no acute injury (<1 month), (3) no history of previous ACL or PCL surgeries or other capsuloligamentous stabilization procedures, and (4) no bony lesions around the knee joint. There were 787 patients who satisfied the inclusion criteria and represented the study population. The mean age at initial presentation was 29.6 ± 11.4 years (range, 6–65 years). There were 602 (76.5%) male patients and 185 (23.5%) female patients.
Stress Radiographic Technique and Measurement
Posterior stress radiographs were taken of all patients with the knee in 90° of flexion, with an applied posterior force of 15 kPa using the Telos device (Telos GmbH, Marburg, Germany). The patient was in the lateral decubitus position with the involved limb on the table. The limb was positioned in neutral rotation, and the load was applied to the anterior proximal tibia at the level of the tibial tubercle (Figure 1). A lateral radiograph was taken with the knee flexed approximately 90°. The lateral radiograph was taken from medial to lateral with a standard tube-to-cassette distance of 1.15 m. All radiographs were performed by 2 experienced orthopaedic radiologic technicians. Stress radiographs were evaluated according to a technique described by Jacobsen and Staubli using peripheral bony landmarks to determine tibial displacement relative to the femur.12,18,19 After a line was drawn across the tibial plateau, perpendicular lines were drawn tangential to the midpoint between the most posterior contours of the medial and lateral femoral condyles and tibial plateaus, respectively. The distance between these 2 points was then measured to determine skeletal displacement of the knee (Figure 2). The measurement was recorded to the nearest millimeter. We did not measure medial and lateral compartment displacement values separately. The PTD was recorded with negative numbers; anterior tibial displacement was reflected with positive numbers.

Patient positioned in the Telos device to obtain a posterior stress radiograph with an applied load of 15 kPa.
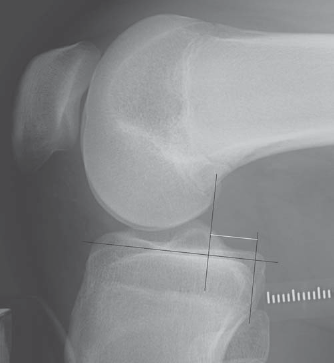
Measurement of posterior tibial displacement on posterior stress radiograph in 90° of flexion. After a line was drawn across the tibial plateau, perpendicular lines were drawn tangential to the midpoint between the most posterior contours of the medial and lateral femoral condyles and tibial plateaus, respectively. The distance between these 2 points was then measured to determine skeletal displacement of the knee (white line).
Evaluation of Intratester and Intertester Reliability
To evaluate intertester reliability, 3 testers measured all 787 stress radiographs independently. As we used a digital radiographic apparatus, paper printouts were available for each tester. Two testers (testers 1 and 2) were well acquainted with the evaluation of posterior stress radiographs, with several years of clinical experience. One tester (tester 3) was considered a novice tester, who was introduced to the measurement technique before conducting the study. To evaluate intratester reliability, one experienced tester reexamined all stress radiographs (again on new paper printouts) after 4 weeks.
Statistics
Descriptive statistics were performed for each tester. The Wilcoxon rank sum test was used for comparison of mean displacement values; P <. 05 was considered statistically significant. Retest reliability (intertester and intratester reliability) was assessed, calculating the change in the mean, standard error of measurement (SEM; ie, the typical error of measurement), and retest correlation. Single SEMs were calculated by dividing the SD of the difference scores between testers by ✓2. The mean intertester SEM was calculated from the single intertester SEMs, the squares of the individual SEMs were added and divided by the number of testers, and then the square root was taken. The SEM was used to calculate confidence intervals for a single measurement and for a change in measurement. For example, the 95% confidence limits for an individual subject's true value have a 95% chance of enclosing that subject's true value. For 2 scores to be significantly different, their values must fall outside the 95% confidence interval. Retest correlation was calculated using the intraclass correlation coefficient (ICC), which is unaffected by any shift in the mean on retest. A 2-way random effects model was used: ICC (2,1). This model allows for the results to be generalized to testers not participating in the study.
Results
Mean PTD values for each tester were determined first. The respective values are given in Table 1.
Mean Posterior Tibial Displacement (PTD) Values for the Different Raters (N = 787) a
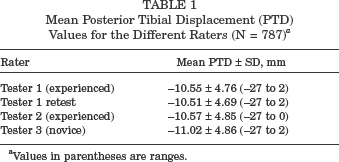
Values in parentheses are ranges.
Intratester Reliability
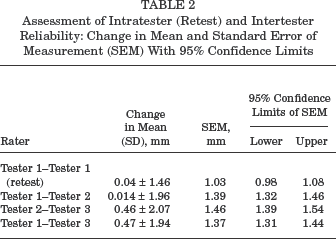
The intratester change in mean was 0.04 ± 1.46 mm. This difference was not significant (P =. 58). The SEM was 1.03 mm (Table 2). The SEM was used to calculate confidence intervals for the precision of a single measurement and the precision of a change in a measurement. The respective confidence limits for the intratester reliability are displayed in Table 3. The single-measure ICC (2,1) was 0.95.
Assessment of Intratester (Retest) and Intertester Reliability: Change in Mean and Standard Error of Measurement (SEM) With 95% Confidence Limits
Intratester Confidence Limits for a Single Measurement and a Change in Measurement a
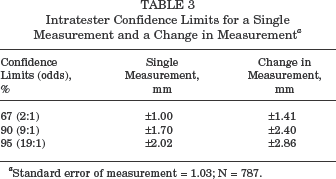
Standard error of measurement = 1.03; N = 787.
Intertester Reliability
To assess the intertester reliability, the change in mean between the 3 examiners and the SEMs with 95% confidence limits were calculated. There was no significant change in mean between the experienced testers (P =. 97). However, there was a significant change in mean between the experienced testers and the novice tester (P <. 001). There was no substantial difference for the SEM between the testers (Table 2). Based on the mean intertester SEM, which was 1.41 mm, confidence limits for the precision of a single measurement and the precision of a change in a measurement for the intertester reliability were calculated (Table 4). The single-measure ICC (2,1) was 0.91.
Intertester Confidence Limits for a Single Measurement and a Change in Measurement a
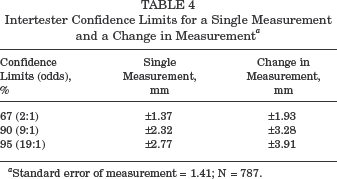
Standard error of measurement = 1.41; N = 787.
Discussion
To the best of our knowledge, no study has previously been conducted to assess the reliability of stress radiography at 90° of flexion using the Telos device for evaluation of posterior knee laxity. Recent studies reporting results after PCL reconstruction have used stress radiography to quantify PTD.2,6 However, before any device can be appropriately integrated into a patient examination, routine, or research protocol, the system's capabilities should be thoroughly understood. 23
In this series of 787 patients, we found no significant difference in mean PTD values for the intratester measurement and for the intertester measurements between the experienced testers. However, in the novice tester, mean PTD was significantly higher compared with that of the other testers. On the other hand, there was no significant difference in the variation of a subject's value from measurement to measurement between the different testers based on 95% confidence intervals for the SEM. The intratester SEM for an experienced tester was ±1.03 mm, and the calculated mean intertester SEM was ±1.41 mm. In addition, both the intratester (0.95) and intertester (0.91) ICCs as a measure of retest correlation represented a high reliability.
Although a thorough and precise physical examination coupled with patient history can be considered diagnostic in the majority of isolated PCL injuries, the objective clinical quantification of laxity is less accurate, and standardized methods for reproducibly measuring all degrees of PCL laxity are needed. 17 Stress radiography was described in 1976 by Jacobsen. 12 He examined 50 healthy subjects and reported an accuracy of ±2.4 mm for anteroposterior measurements. In another study, Hewett et al 8 found a mean relative posterior translation of 12.2 mm in patients with complete PCL tears. They reported an accuracy level of ±1.5 mm (from 90% confidence limits) for stress radiographs to determine PTD. However, the authors did not report on the details of the reproducibility of the study. 8
In this study, we calculated 3 important components of retest reliability, which refers to the reproducibility of values of a variable when measuring the same subjects twice or more: change in the mean, SEM, and retest correlation (ICC). 9 The SEM was used to calculate confidence limits to determine a range within which the true value is likely to fall. Confidence limits for a change between measurements are greater because the change involves 2 measurements, each of which has an error. 10 The corresponding 95% confidence intervals for intratester reliability were ±2.02 mm for a single measurement and ±2.86 mm for a change between measurements. Intertester reliability exhibited 95% confidence intervals of ±2.77 mm for a single measurement and ±3.91 mm for a change between measurements. In a thorough study, Huber et al 11 investigated the reliability of the KT-1000 arthrometer in the assessment of posterior laxity. They found the KT-1000 arthrometer to be a moderately reliable tool for the measurement of tibial translation in patients with PCL tears. The 95% confidence intervals of the SEM were ±2.53 mm for an experienced tester and ±2.95 mm for a novice tester to determine corrected posterior translation values. The 95% confidence interval between testers was ±3.27 mm. The ICC values for the novice, experienced, and intertester reliability were 0.67, 0.79, and 0.62, respectively, for corrected posterior translation. 11 Also, direct comparison may not be applicable. Because of a significantly larger number of subjects tested in this study, stress radiography exhibited lower intratester and intertester confidence intervals with, at the same time, higher ICC values in the assessment of PTD.
Although stress radiography has many advantages compared with physical examination and arthrometry as skeletal displacement alone is measured, which eliminates errors from compliance of the soft tissues, the accuracy of stress radiographs is influenced by multiple variables. Lack of patient relaxation may lead to quadriceps muscle activity and thus reduce posterior displacement. 4 The most problematic variable, however, is rotational errors, which can be introduced from rotation of the limb, rotation of the x-ray beam, or coupled rotation produced by the translation of the knee.4,8 Although other measurement methods have been advocated, 22 we recommend the use of peripheral landmarks to define translation values.
We did not measure medial and lateral compartmental displacement separately for several reasons. With a true lateral radiograph, the most posterior contours of the medial and lateral femoral condyles are nearly in line and easy to identify, whereas it is more difficult to determine the tibial reference point because of the variable contour, especially of the medial tibial plateau, which is larger and more squared posteriorly than the lateral tibial plateau. Therefore, the distance between the most posterior aspects of the medial and lateral tibial plateau differs considerably between patients. When evaluating the patients with the greatest within-subject variation between testers, these variations were mainly owing to a different identification of the tibial reference landmark. Also, the significantly higher mean PTD values obtained by the novice tester reflect a systematic measurement error, which in our opinion is mainly affected by a different identification of the tibial reference landmark compared with that of the experienced testers. Especially in patients with a large medial tibial plateau, this may lead to an overestimation of posterior laxity when the examiner adheres too closely to the edge of the medial tibial plateau. Greater medial tibial plateau displacement values with stress radiography have already been noted by other investigators when measured separately.8,14
Stress radiography in 90° of flexion using the Telos device exhibited a useful reliability for evaluation of PTD in knees with PCL lesions. A standardized radiographic technique and correct identification of the bony landmarks are mandatory for the precision of the measurement method.