
Abstract
Background: Injuries to the posterolateral corner of the knee are disabling. Despite improved understanding of this group of tendons and ligaments, the best surgical treatment of an unstable corner is not clear.
Hypothesis: Surgical repair of acute tears of the posterolateral corner has outcomes that are as good as those from reconstruction combined with an early motion rehabilitation protocol.
Study Design: Cohort study; Level of evidence, 2.
Methods: Sixty-three patients with 64 posterolateral corner tears were included in this study, with 39 posterolateral corner repairs and 25 reconstructions using the modified 2-tailed technique. Patients were evaluated with clinical and KT-2000 arthrometer examinations, as well as with Lysholm, International Knee Documentation Committee, and Short Form-36 scores.
Results: Fifty-six patients with 57 corner tears had minimum clinical follow-up of 24 months (range, 24-59 months). Acute primary repairs were performed on 35 patients, with 22 successful outcomes and 13 (37%) failures. Primary reconstructions were performed on 22 patients, with 20 successful outcomes and 2 (9%) failures. The difference in stability on clinical examination between repairs and reconstructions was significant (P < .05). Fourteen of 15 patients with failures of the primary posterolateral corner repair or reconstruction underwent successful revision reconstruction. The final patient with failure of the primary repair elected not to have a revision reconstruction. The final mean Lysholm knee score for both repair and reconstruction patients was 88.7 (range, 53-100). Final International Knee Documentation Committee objective scores yielded 14 (26%) normal, 28 (52%) near-normal, 9 (17%) abnormal, and 3 (6%) severely abnormal knees; the mean score was 60 at the most recent clinical evaluation.
Conclusion: Results with repair followed by early motion rehabilitation have been significantly inferior when compared with results from reconstruction using the modified 2-tailed technique. The authors now use reconstruction rather than repair in the majority of patients who sustain posterolateral corner tears after high-energy injuries.
Posterolateral instability of the knee has been noted to be a remarkably disabling condition.3,15 The structures of the posterolateral corner (PLC) are a complex combination of both dynamic and static stabilizers. It may be the least well-understood and studied region of the knee, leading to its designation as the “dark side” of the knee. 2 One reason that the diagnosis and ideal treatment of PLC injuries have remained elusive is the complexity of the anatomy. † Instability of the PLC has now been clearly associated with failure of reconstructions of both the ACL and the PCL,5,9,12,13 leading investigators to an increased interest in the diagnosis and treatment of PLC injuries.
References 5, 9, 12–14, 17, 18, 21, 22, 26.
Despite the rapidly improving understanding of the anatomy and biomechanics of the PLC, the best surgical treatment of an unstable PLC is not clear.5,12,24 Many authors recommend repair of acute tears of the PLC if the tissue quality of the torn structures is adequate.3,5,12,15 In the case of chronic PLC instability or acute tears with inadequate tissue, a wide variety of reconstructions have been advocated.1,3–8,11,12,16,19,24 However, there are few clinical outcome studies, and many are small series and/or have limited follow-up.1,4,6–8,11,16,19
The purpose of this study is to compare the results of repair versus reconstruction of the PLC of the knee. A second purpose is to describe an anatomical reconstruction technique using allograft to reconstruct the PLC using a modified 2-tailed technique.
Materials and Methods
Between December 1997 and May 2001, 63 consecutive patients with 64 tears of the PLC were included in a prospective outcome study. Thirty-nine patients underwent primary repair of their PLC tears, and 25 had primary reconstructions. Seven patients (4 repairs and 3 reconstructions) were lost to follow-up before 24 months, leaving a study cohort of 56 patients with 57 tears of the PLC. Inclusion criteria in our study included a tear of the PLC (either acute or chronic), minimum follow-up of 24 months, and confirmation of the tear both on MRI scan and at the time of surgery. Those who were excluded from the study included patients unable or unwilling to comply with postoperative rehabilitation, patients unwilling to return to our medical center for follow-up, prisoners, and mentally handicapped patients.
Patients entered into this study were not randomized with respect to the treatment of their PLCs. Patients were treated with repair of the PLC if they met 2 key criteria. The first criterion was that the index surgery on the PLC had to take place within 3 weeks of the injury. The second criterion was that the tissue at the time of surgery had to be adequate to support a repair. If the primary damage was at the musculotendinous junction or if the ligaments were markedly stretched and thinned, the injury was deemed not eligible for repair. Most of the patients in our repair population avulsed the fibular collateral ligament (FCL) and the popliteus from the femur. Poor-quality tissue and musculotendinous junction tears led to a primary reconstruction.
Data collected in our study included basic demographics, the mechanism of injury, and the Injury Severity Score (ISS). The ISS is a score that measures the severity of multisystem trauma, not the severity of the patient's skeletal injuries. It is calculated by adding the square of the 3 most severe Abbreviated Injury Scale scores, which evaluates individual systems such as thoracic, head, abdomen, musculoskeletal, and so forth. The score varies between 3 and 75, with a score of 16 or more indicating a multitrauma patient. Follow-up examinations were performed by the primary investigator and included assessment of range of motion, varus stress, and external rotation (dial test) at both 30° and 90°. We evaluated the patients for varus instability at 0° and 30° of flexion. Patients were scored on a 0 to 3+ scale, with 0 reflecting no laxity, 1+ representing 5° of laxity, 2+ representing 10° of laxity, and 3+ representing 15° or more of laxity when comparing the 2 sides. The dial test was performed with patients in a prone position when performed in the clinic and in a supine position when performed as part of an examination under anesthesia before the surgical reconstruction. The test was conducted at both 30° and 90° of flexion. Great care must be taken to keep the knees together while applying the external rotation force. Again, results were scored on a scale from 0 to 3+. Zero represented a knee with less than 5° of difference between the 2 legs, 1+ was a leg with 5° to 10° of difference, 2+ for 10° to 15° of difference, and 3+ for more than 15° of difference between the 2 legs. In both tests, a grade of 0 or 1+ represented a successful result, and a score of 2+ or 3+, on either the dial or varus stress test, was considered a failure.
All patients underwent KT-2000 arthrometer (MEDmetric Corp, San Diego, Calif) examinations as part of the follow-up protocol. Laxity in both the anterior and posterior directions was measured on both the injured and uninjured knee at both 30° and 70° of flexion. Great care was taken on examination to make certain that the knee was not sagging posteriorly before initiating the examination because posterior sag can lead to results that indicate less posterior laxity and more anterior laxity than are present. In addition, we report our results for anterior, posterior, and total anteroposterior translation. The total anteroposterior translation measurement will reflect the clinical laxity even if the knee was erroneously allowed to sag before the arthrometer examination was started. Serial Lysholm knee scores were performed at follow-up visits that were more than 6 months from the time of surgery. The International Knee Documentation Committee (IKDC) subjective and objective scores were also obtained at the most recent follow-up. The Short Form–36 (SF-36) functional outcome score was also obtained at clinic visits throughout the follow-up period.
Many patients in our series were not competitive athletes. Therefore, we also assessed them regarding return to recreational activities using our own scale. Patients were classified as a competitive athlete, a recreational athlete, participating in hobbies (eg, hunting, fishing, gardening), or sedentary. We then scored patients in terms of their ability to return to their prior levels of recreational activity. This scoring system addresses patients who have limited involvement in competitive athletics, while giving an assessment of the patients’ capabilities after PLC reconstruction. Similarly, we evaluated the patients’ employment situations and scored them as return to full-time work at the same job, return to full-time employment at a different job, return to light duty only, or unable to return to work.
Repair of the PLC was selected in patients with acute injuries and good-quality tissue. In the majority of cases, the popliteus and FCL were avulsed from the femur with no bony attachment. In that instance, the injury was directly repaired using suture anchors after decorticating bone at the site of insertion. Damage to the popliteofibular ligament, coronary ligament tears, biceps tears, and capsular tears were all directly repaired. Bony avulsions from the fibular head were repaired using open reduction and internal fixation with screws.
All reconstructions were accomplished using the modified 2-tailed technique using a tibialis anterior or tibialis posterior allograft. In this procedure, 3 critical components of the deep layer5,12,23 of the PLC are reconstructed: the popliteus, the popliteofibular ligament, and the FCL or lateral collateral ligament. Our technique involved drilling a 5-mm hole from anterior to posterior through the lateral tibia, exiting where the popliteus tendon traverses the back of the tibia. The tibial tunnel is tapped with a 7-mm tap. The allograft is trimmed to a size of 5 mm and passed into the tunnel from posterior to anterior. The graft is secured with a 7-mm bioabsorbable ligament screw. A second 5-mm drill hole is made through the proximal fibula, aimed from anterolateral to posteromedial. The isometric point on the lateral femoral condyle is then located. The isometric point lies just superior to where the FCL and popliteus cross one another on the lateral femoral condyle. A 3.2-mm drill bit is then used to drill a hole for a long 4.5mm bicortical screw going from lateral to medial. A spiked ligament washer is used with the screw. An osteotome facilitates decortication of the bone posteriorly and anteriorly around the screw, allowing the allograft to heal to the bone in the anatomical locations of the FCL and popliteus, respectively. The graft is then taken from the posterior tibia up and around the screw in the lateral femoral condyle, back down to the fibular tunnel, through the tunnel, and back to the screw and washer. The graft is tensioned with the foot internally rotated and the knee flexed 40° to 60°. The free end of the graft is anchored primarily by the spiked ligament washer but is supplemented with a No. 2 suture. The graft reconstructs the popliteus, popliteofibular ligament, and the FCL (Figure 1).
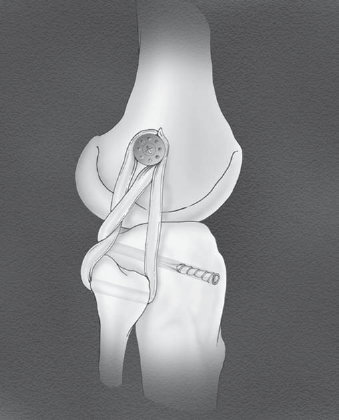
The modified 2-tailed reconstruction of the posterolateral corner after tensioning the graft.
The Compass Knee Hinge (CKH, Smith & Nephew, Memphis, Tenn) was used on some patients in this series. Indications for the use of the hinge included all patients with associated tibial plateau fractures, as well as patients who entered a randomized prospective study using the CKH for knee dislocation. Twenty-nine knees in our study received the CKH, and 28 did not have a hinge. The distribution of hinges in this study included 17 patients with the CKH and 18 with no CKH in the repair group, compared with 12 with the CKH and 10 without the CKH in the reconstruction group. There was no significant difference between the groups regarding the number of patients treated with the CKH.
The postoperative rehabilitation protocol was identical for both the repair and reconstruction groups. Our postoperative protocol included an aggressive early motion regimen beginning on postoperative day 1 in all patients with knee dislocations. These patients started range of motion from 0° to 30° on the first postoperative day using a continuous passive motion machine. The motion was gradually increased over the next few days toward a range of motion of 0° to 90°. The continuous passive motion and early motion protocols are designed to discourage motion loss due to arthrofibrosis, which is common after knee dislocations. Partial weightbearing using crutches was encouraged for the first week, with advancement to full weightbearing if their other injuries permitted. Knee rehabilitation was dictated by the cruciate ligament injuries, with concentration on early motion and closed chain exercises. Patients with an isolated PLC injury used a knee immobilizer for approximately 2 weeks and then started progressive range of motion exercises. Patients with an isolated PLC injury did not begin aggressive motion work for 10 days to 2 weeks.
When comparing continuous variables between groups, statistical significance was assessed using t tests; for categorical variables, the Fisher exact test was used. P values of. 05 (2-sided) were considered statistically significant. For the longitudinal comparison of SF-36 scores, repeated-measures analysis of variance was used.
Results
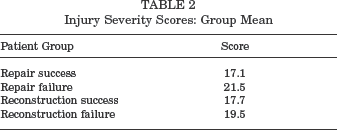
Fifty-six patients with 57 PLC tears and a minimum follow-up of 24 months were included in this series. The mean age of our patients was 33 years (range, 17–57 years). There were 35 male and 21 female patients included, with tears of 28 right and 29 left PLCs. Mean follow-up in our series was 33 months (range, 24–59 months). The majority of patients in our study were involved in high-energy trauma, frequently with associated fractures. Forty-four patients sustained multiligament knee injuries, whereas 13 had isolated PLC tears. There were 28 multiligament knee injuries and 7 isolated PLC tears in the repair group, compared to 16 multiligament injuries and 6 isolated tears in the reconstruction group. Table 1 provides detail regarding the ligaments repaired or reconstructed, whether the cruciate ligaments were staged, and the use of the compass hinge. The mean ISS was 19.2 (range, 9–50). Table 2 documents the ISS values for each of the separate groups. There was no significant difference between the groups with our enrollment, and the value was greater than the threshold of 16, which defines multitrauma for all 4 groups. Our patients sustained their ligament damage with the following mechanisms of injury: motor vehicle accident, 33; motorcycle accident, 8; athletic injury, 4; high-energy fall, 4; motor vehicle versus pedestrian accident, 4; assault, 1; boating accident, 1; and crush injury after a logging accident, 1.
Injury and Treatment a
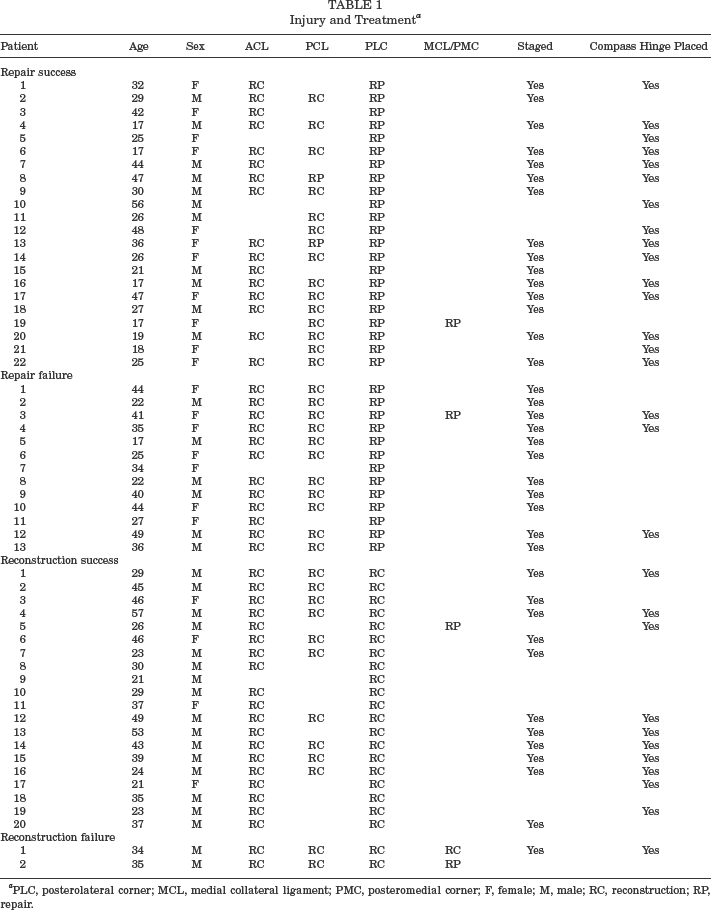
PLC, posterolateral corner; MCL, medial collateral ligament; PMC, posteromedial corner; F, female; M, male; RC, reconstruction; RP, repair.
Injury Severity Scores: Group Mean
Twenty-two patients underwent successful repairs of the PLC, compared with 13 (37%) whose repairs failed. Twenty patients had successful PLC reconstructions, whereas 2 patients had failures (9%). The difference in success based on stability on clinical examination between the repair and reconstruction groups was significant with a P value of. 03 (Fisher exact test). Twelve of the 13 patients with failed PLC repairs and both of the patients with failed reconstructions have undergone successful revision reconstruction of their PLCs. Two of the 13 failures involved the suture anchors, with 1 failure of the suture and 1 case of failure of fixation of the anchor itself. The remaining 11 cases were well fixed at the site of repair when evaluated at the time of revision surgery. The clinical failure in all 11 cases appeared to be failure (either stretch or rupture) within the ligament or tendon rather than a failure of fixation. Eleven of 28 repairs in multiligament knee injuries failed (39%), compared with 2 of 7 isolated repairs (29%). Two of 16 reconstructions failed (13%) in multiligament knee injury patients compared with 0 of 2 reconstruction failures (0%) in isolated PLC tears. When evaluated clinically (before any revision procedures) for lateral laxity with varus stress, patients had a mean of 1.0 after repair and 0.5 (scale, 0–3) after reconstruction of the PLC. Nineteen patients (54%) had grade 0 laxity to varus stress, 4 (11%) had grade 1+, 5 (14%) had grade 2+, and 7 (20%) had grade 3+ laxity after repair of the PLC. After reconstruction, 14 patients (64%) had grade 0, 6 (27%) had grade 1+, 1 (5%) had grade 2+, and only 1 (5%) had grade 3+ for laxity to varus stress. Evaluation of external rotation before revision procedures demonstrated a mean of 0.9 for repairs compared with 0.3 for reconstructions. Also, 21 patients (60%) graded at 0 for external rotation after repair of the PLC, 2 (6%) were grade 1+, 5 (14%) were grade 2+, and 7 (20%) were grade 3+. After reconstruction, the results were as follows: 19 (86%), grade 0; 1 (5%), grade 1+; 0 (0%), grade 2+; and 2 (9%), grade 3+. Clinical results after revision surgery were very similar for the 2 groups, with varus laxity of 0.2 in knees with repairs and 0.3 in knees with reconstructions, as well as external rotation of 0.1 in knees with repairs and 0 in knees with reconstructions. Knee range of motion in our patients at the most recent clinical follow-up was a mean of 128° of flexion (range, 75°-150°) and 1° of extension (range, 0°–5°). There was no difference in knee motion achieved by patients after repair of the PLC (range, 1°–128°) when compared with patients who underwent reconstruction (range, 1°–129°). The clinical results at the most recent evaluation in terms of mean laxity to varus stress and the dial test are summarized in Table 3. In addition, the mean results for clinical laxity at the time of diagnosis of PLC failure are also documented in the table.
Final Results After Revision of Failures
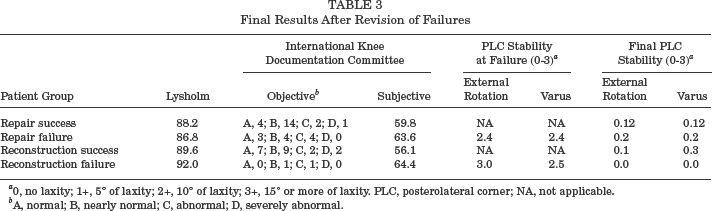
0, no laxity; 1+, 5° of laxity; 2+, 10° of laxity; 3+, 15° or more of laxity. PLC, posterolateral corner; NA, not applicable.
A, normal; B, nearly normal; C, abnormal; D, severely abnormal.
Study patients were sequentially evaluated with Lysholm knee scores at clinical follow-ups beginning 3 months after surgery. The mean Lysholm score for the whole group at the time of their most recent clinical evaluations was 88.7 (range, 53–100). Patients who had a successful repair had a final mean Lysholm score of 88.2, whereas those who had a failed repair that was revised had a final mean score of 86.8. Patients who had a successful reconstruction had a mean score of 89.6 compared with a final mean score of 92 for failed PLC reconstructions that were revised. There was no difference between the final Lysholm knee scores in the 4 groups. Before revision, the patients with failed repairs and reconstructions had a mean score of 64.6, which was significantly lower (P <. 05) than the score of 89 for patients with a successful initial repair or reconstruction. Lysholm knee scores are also summarized by patient group in Table 3.
KT-2000 arthrometer ligament examinations were performed on our patients during follow-up examinations. There were no significant differences between patients who underwent successful repairs, those with failed initial repairs with revision, those who underwent successful initial reconstructions, and those with failed initial reconstructions with successful revisions. Please see Table 4 for a summary of the displacement using maximum force.
KT-2000 Arthrometer Ligament Data, mm a
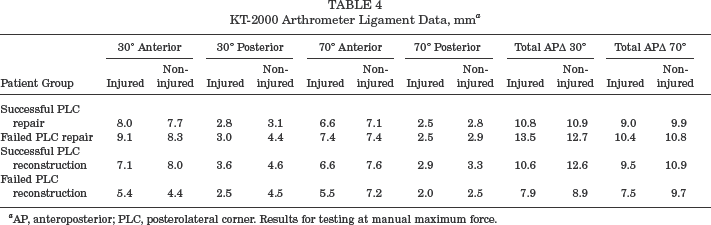
AP, anteroposterior; PLC, posterolateral corner. Results for testing at manual maximum force.
Fifty-four patients in this study were evaluated both subjectively and objectively using the IKDC scores at final follow-up. Objective scores for the whole group included 14 patients with normal knees (26%), 28 with near-normal knees (52%), 9 with abnormal knees (17%), and 3 with severely abnormal knees (6%). Seventy-eight percent of our patients had either normal or nearly-normal knees using the IKDC objective evaluation. There was no significant difference between the individual groups in IKDC scores at final follow-up. Subjective scores for the patients in this study had a mean of 60 (range, 17.2–100). Again, there was no significant difference between the groups in final subjective scores. The IKDC results are summarized in Table 3.
The SF-36 patient outcome scores were obtained from patients when they returned for clinic follow-up. There was no difference in either the Physical Component Summary (PCS) scale or Mental Component Summary (MCS) scale when comparing those who had initial repair and those who had reconstruction of the PLC. The mean PCS for patients with reconstructions was 34.1, compared with 33.9 for patients who had repairs. The mean MCS for patients after reconstruction was 48.3, compared with 46 for those who underwent repair of the PLC. There was no difference in the final mean PCS when comparing patients who had a failed repair or reconstruction and those who had a successful procedure. There was a significant difference in the MCS in those who had successful initial repairs or reconstructions (mean score, 48.1) and those who had failures (mean score, 43.1). The P value was. 01 using the Student t test. When patients were evaluated regarding the time from surgery, there was a significant improvement in PCS values (as the time from surgical reconstruction of the PLC to completing the SF-36 lengthened; P =. 02), but there was no associated improvement over time in MCS scores. When evaluating patients who underwent repair of the PLC, there were improvements over time in both the PCS (P <. 01) and the MCS (P =. 03) scores. When evaluating the scores of patients who had a successful initial PLC repair or reconstruction, there was a significant improvement in PCS over time (P <. 01) but not in MCS (P =. 7). Those who had an initial failure in their PLC procedure experienced a significant improvement in their MCS scores over time (P <. 01) but not in their PCS scores (P =. 4).
We evaluated our patients in terms of their ability to return to their preinjury employment. Thirty-seven of our patients returned to their original jobs, whereas 5 returned to full-time employment at different jobs. Five patients returned to light duty only, and 9 patients did not return to work. The breakdown of the ability of patients in the various groups to return to their jobs is detailed in Table 5. The ability to return to work was not predicted by initial failure of the PLC repair or reconstruction. However, all of the patients with failures who returned to their vocations had a successful revision procedure before returning to their jobs. Thirty-one of our patients have returned to their prior levels of activity when evaluated for recreational activities, whereas 25 have returned to lesser levels of activity. Details of the various groups are again depicted in Table 6.
Employment Status
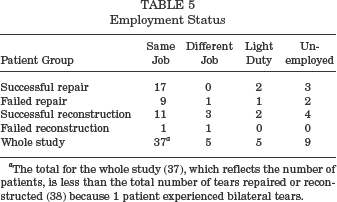
The total for the whole study (37), which reflects the number of patients, is less than the total number of tears repaired or reconstructed (38) because 1 patient experienced bilateral tears.
Recreational Activities
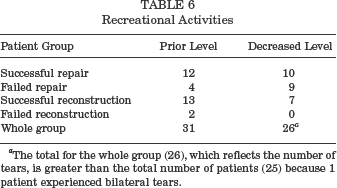
The total for the whole group (26), which reflects the number of tears, is greater than the total number of patients (25) because 1 patient experienced bilateral tears.
In addition to the failed PLC repairs and reconstructions, patients in this study experienced a number of complications. For the group as a whole, 14 patients experienced 18 complications for an incidence of 25%. There was no significant difference in the incidence of complications between the group with repairs (21%) and those with reconstructions (27%). Thirteen of the 14 patients who experienced a complication were patients who had a multiligament knee injury. The incidence of complications after multiligament injuries was 30%, compared with 8% for patients with isolated corner injuries. The complications experienced by patients in our study included arthrofibrosis, 10 patients (18%); heterotopic ossification, 2 patients (4%); hematoma, 2 patients (4%); severe osteoarthritis, 1 patient (2%); fistula, 1 patient (2%); medial femoral condyle osteonecrosis, 1 patient (2%); and iatrogenic peroneal nerve injury, 1 patient (2%).
Discussion
The PLC is a region of the knee that has generated significant interest recently, with numerous studies delineating the complex anatomy of the region.9,17,20,23,26 The PLC anatomy is divided into 3 layers, 20 with the most critical structures, including the FCL, popliteus tendon, and popliteofibular ligament, located in the second or third layer. Cadaveric studies using selective sectioning have clarified the role of the PLC in preventing opening to varus stress and preventing external rotation, as well as having a secondary role as a posterior and anterior stabilizer.9,10,13,14,17,23,26 The popliteofibular ligament has drawn attention in recent studies as a key component of the corner, resisting posterior translation, varus stress, and external rotation. Although most reconstructions do not address the popliteofibular ligament, the biomechanical data indicate that restoration of this key component of the deep layer should be included when reconstructing the PLC.18,21,22
Many authors have recommended anatomical repair of the PLC if surgery is performed within 2 to 3 weeks of injury and adequate tissue is available for repair.3,5,12,24 However, there are many variables that affect the decision to repair the PLC. The severity of soft tissue damage, associated ligamentous structures that are injured, location of the PLC tissue damage, and rehabilitation protocol may all affect the outcome of a repair. Some authors have noted that the damage to the popliteus is frequently at the musculotendinous junction, 3 which precludes repair. Despite the recommendation for repair noted above, there are few published series of PLC repairs using accepted knee scores in the recent literature.
Posterolateral corner reconstruction procedures have been reported in the recent literature. The procedures have varied, but most have not been procedures that reconstruct the anatomy of the deep layer of the PLC. Biceps tenodesis has been proposed, with variable results.4,7 One problem noted with biceps tenodesis on biomechanical testing is that it overconstrains the knee in both external rotation and varus stress. 25 Other reconstructions have included a sling procedure 1 and a Larson-type tenodesis. 8 Both of these nonanatomical reconstructions produced disappointing results. Both Latimer et al 16 and Noyes and Barber-Westin 19 have reported reconstructions using an allograft to replace only the FCL. Both reported results that were better than the nonanatomical approaches but still had significant failure rates. Interestingly, Noyes and Barber-Westin also used an immediate range of motion rehabilitation program and achieved outstanding final knee motion. 19 Finally, Clancy et al 3 have recently reported on a technique that initially reconstructs the popliteus and then reconstructs the FCL if necessary. They used Achilles tendon allograft. No results were given regarding this technique. 3 Clearly, surgeons are moving toward anatomical reconstruction of the PLC using an allograft, although none of the procedures described above reconstructs all 3 critical components of the deep layer of the PLC.
The results in our series of patients clearly favored reconstruction of the PLC over direct repair. Physical examinations, Lysholm knee scores, and IKDC objective scores obtained at the most recent clinical follow-up have been good for the majority of our patients. Patients have been able to return to work in the vast majority of cases, despite significant associated skeletal trauma in most patients. The IKDC subjective scores have not been as good as most of the other data in this study. The relatively low subjective scores may relate to the fact that most of our patients are not serious athletes. A number of the questions on the subjective questionnaire are specific to athletic activity, yielding a lower score in many of our patients despite a stable knee with good motion. The scores are also decreased by the variety of injuries these patients sustained, both to other parts of the musculoskeletal system and to other systems of the body. The only way to know how these factors relate would be to compare our results with a study of isolated PLC reconstructions in athletes. We believe the modified 2-tailed technique restores the anatomy of the deep layer to a greater degree than do most reconstruction techniques. It also provides a quality of tissue and fixation that allows for early motion of the knee. We believe early motion protocols are very desirable in patients after knee dislocation, in which arthrofibrosis is a frequent problem.
Patients in our study experienced numerous complications. There was no significant difference between repairs and reconstructions regarding the occurrence of complications. In all but 1 patient (who experienced a hematoma), the complications occurred in patients after multiligament knee injuries. The incidence of complications after knee dislocations is high in many studies in the literature. The incidence of arthrofibrosis compares favorably with the literature for knee dislocations, as does our final range of motion. The early motion rehabilitation may improve the outcome regarding arthrofibrosis and loss of motion but may increase the risk of wound-healing problems.7,8,20 Additional studies will be necessary to determine if changes in the timing of surgery, rehabilitation protocols, or other variables can favorably affect the occurrence of complications.
There are many variables that affect the outcome of repairs of the PLC. We recognize that the results might be more favorable if different techniques were employed (eg, recession or the use of a different technique for repairing the ligaments back to the femur) or if different rehabilitation protocols were used. We also recognize that staging the reconstruction of the ACL may yield a less favorable environment for the PLC repair. If the delayed ACL reconstruction is a factor contributing to failure of the PLC repairs, the staged ACL does not appear to be causing a high rate of failure in the reconstruction patients. The majority of our failures appeared to relate more to tissue quality than to failure of the repair. Despite preferentially routing the patients with the best-appearing tissue into the repair group, the tissues were not good enough to yield success on a consistent basis. The severity of the damage to the popliteus and FCL was not fully appreciated at the time of initial repair. As noted in the “Materials and Methods” section of this article, the distribution of compass knee hinge patients was similar between the repair and reconstruction groups. However, the failure rate of repairs with a compass hinge was lower (19% compared to 43%) than was the failure rate with a hinged knee brace. This result suggests that better repair techniques might lead to more successful outcomes.
Weaknesses of this study included a number of factors. Although we had the advantages of a single surgeon performing a single repair or reconstruction of the PLC with uniform postoperative rehabilitation protocols, our patients had notable variations in the associated injuries (both knee and systemic) as a result of their high-energy trauma. These variations are common in multiple-trauma patients and are unavoidable, but they make interpretation of the results more difficult. Another weakness as noted above is that patients with knee dislocations who had a PLC repair underwent our early motion rehabilitation protocol, which may have predisposed the repairs to failure. Another limitation of this study is that varus and posterolateral laxity were assessed by clinical examination only and not by more objective methods such as stress radiographs.
Anatomical reconstruction of the PLC using an allograft has yielded gratifying results in this series of patients. Long-term follow-up and larger series will be necessary to confirm the results using the modified 2-tailed technique. We strongly recommend reconstruction rather than direct repair if an immediate motion rehabilitation protocol is employed. Based on our results, we now repair the PLC only in the case of avulsions with significant bone fragments that allow internal fixation with screws.