
Abstract
Background: Symptomatic, traumatic posterior shoulder instability is often the result of a posteriorly directed blow to an adducted, internally rotated, and forward-flexed upper extremity. Operative repair has been shown to provide favorable results. Current arthroscopic techniques with suture anchors and the ability to plicate the capsule using a nonabsorbable suture may provide favorable outcomes with reduced morbidity.
Purpose: To evaluate the results of operative shoulder stabilization in patients with traumatic posterior shoulder instability.
Study Design: Case series; Level of evidence, 4.
Methods: A consecutive series of patients who underwent arthroscopic or open posterior stabilization for traumatic posterior shoulder instability were evaluated using subjective assessments, physical examinations, the Single Assessment Numeric Evaluation, Rowe score, Simple Shoulder Test, and the Western Ontario Shoulder Instability Index.
Results: Between May 1996 and February 2002, 31 shoulders (30 patients) underwent posterior stabilization (19 arthroscopically, 12 open). There were 29 men and 1 woman (mean age, 23 years). Preoperatively, all patients had a distinct traumatic cause for the instability. On physical examination, all patients had posterior apprehension and increased (2+, 3+) posterior load-shift testing. Preoperative radiographs and/or magnetic resonance imaging revealed posterior rim calcification or reverse Bankart lesions in 29 cases (94%). At arthroscopy, posterior labral injuries, reverse Bankart lesions, or humeral head defects were identified. Follow-up averaged 40 months, and the mean duration between injury and surgery was 21 months. The mean Single Assessment Numeric Evaluation, Rowe score, Simple Shoulder Test, and Western Ontario Shoulder Instability Index scores, respectively, for the entire group were 89, 87, 11, and 346; for the open group, they were 81, 80, 10.5, and 594; for the arthroscopic group, they were 92, 92, 11.4, and 190. The Western Ontario Shoulder Instability Index (P < .03) and Rowe score (P < .04) outcomes scores for the arthroscopic group were statistically better than those of the open group. Twenty-nine of 31 shoulders were rated as excellent or good.
Conclusion: In the case of traumatic posterior shoulder subluxation, posterior lesions of the labrum (“reverse Bankart”), articular edge, and capsule are observed. Surgical treatment addressing these lesions led to satisfactory results for both the open and arthroscopic treated groups. In this study, an arthroscopic technique utilizing suture anchor repair with capsular placation provided the most favorable outcomes.
Posterior glenohumeral instability is much less commonly observed in clinical practice than either anterior or multidirectional instability. It occurs in approximately 2% to 5% of all cases of shoulder instability.6,27,29 Classically, posterior glenohumeral instability has been classified into acute, chronic, or “locked,” as well as voluntary or involuntary. Traditionally, posterior shoulder instability has been described to occur in conjunction with other directions of instability and is often precipitated by minimal trauma. Generalized ligamentous laxity has been noted to be a frequent clinical hallmark feature. In contrast, isolated, traumatic posterior glenohumeral instability has been traditionally associated with high-energy trauma or the result of a seizure disorder.6,21
More recently, isolated, posterior shoulder instability has been recognized as a significant clinical problem in collision or contact athletes.20,31,35 The mechanism of injury is typically a posteriorly directed force on a forward-flexed, adducted, and internally rotated arm. Although a dislocation can occur, subluxation is more common with athletic injuries. The mainstay of treatment for patients with recurrent posterior instability has been rehabilitation of the external rotators, specifically the infraspinatus.12,25 When this treatment is unsuccessful, a variety of open posterior stabilization procedures have been employed. 21 In the past decade, arthroscopic procedures have gained in popularity, and with the advent of suture anchors, capsular plication, and thermal capsulorrhaphy, arthroscopic stabilization of this complex problem has become a viable option.2,20,22,23,35,36 The purpose of this study was to evaluate the results of open and arthroscopic stabilization for patients with traumatic, posterior shoulder instability secondary to collision and contact sports.
Methods
A retrospective review was performed to identify all patients diagnosed with posterior glenohumeral instability who underwent operative stabilization. Patients from 2 military medical centers and the University of Connecticut (when the senior author [R.A.A.] retired from the military) composed the study population. Inclusion criteria consisted of a traumatic cause for the instability, recurrent posterior subluxation precluding return to full activity or sports, and failure of a formal rehabilitation regimen. An exception to a full course of physical therapy was allowed for those patients who sustained a bony posterior Bankart lesion that required operative fixation (1 shoulder) or those patients who, after their initial injuries, could not complete the rehabilitation program because of symptoms of gross instability (2 shoulders). Exclusion criteria included generalized ligamentous laxity or multidirectional instability. Although previous attempts at posterior instability repair excluded participation in our cohort, an anterior stabilization operation (1 shoulder) and previous shoulder arthroscopy (2 shoulders) were not exclusionary.
Patient Examination
For preoperative evaluations and follow-up examinations, patients were evaluated using a standardized set of outcome questionnaires. Specifically, the Single Assessment Numeric Evaluation (SANE), Rowe score, Simple Shoulder Test (SST), and Western Ontario Shoulder Instability Index (WOSI) were used. The SANE score 34 consists of a single subjective evaluation score from 1 to 100 in which 100 is considered “normal function.” The Rowe 28 score is made up of 3 domains with a maximum score of 100. The 3 domains include function, stability, and range of motion. The SST 19 is a series of 12 yes or no questions related to function and sports activities. It is graded according to the number of positive answers. The WOSI 18 was developed as a primary outcome measure in clinical trials evaluating patients with shoulder instability. It consists of 21 questions, each response being evaluated by a 10-cm visual analog scale anchored verbally at either end. The evaluation measures disability, and therefore, a 0 to 2100 point range is possible; the lower scores reflect lesser disability and, thus, better outcomes. A subjective shoulder evaluation, as described by Wolf and Eakin, 36 for results after operative treatment of posterior instability was also used. Shoulder examinations were performed using the grading scale proposed by Altchek and Dines to assess posterior humeral translation. 1 This system grades the amount of humeral translation across the glenoid from 1+ to 3+. The amount of translation is compared to that of the contralateral shoulder, but typically a 2+ or greater posterior humeral translation is an abnormal result.
Standard radiographic evaluations and subsequent MRI or MR arthrography studies were obtained on all patients. Patients underwent a formal course of rehabilitation after their injuries or presentation emphasizing rotator cuff (especially infraspinatus) and periscapular muscular strengthening. For those patients who failed to return to full activities or continued to experience instability symptoms, a posterior stabilization operation was performed using either an open or arthroscopic technique. The choices of the operative technique and patient position were made according to the surgeon's preference. Although general endotracheal anesthesia was typically employed, for additional postoperative analgesia, most patients underwent interscalene regional blocks. An examination under anesthesia with the patient supine allowed documentation and confirmation of the grade of instability. All shoulders were then evaluated arthroscopically to confirm the diagnosis and assess the extent of capsulolabral or bony injury.
Open Reconstruction Technique
The 12 patients who experienced open repairs underwent a posterior approach to the shoulder as described by Hawkins and Janda. 13 The deltoid was split in line with its fibers, and the infraspinatus was either released from its humeral insertion or retracted superiorly to develop an interval between it and the teres minor. The posterior capsule was then incised vertically to expose the joint. The posterior labrum was repaired using suture anchors, and a capsulorrhaphy was performed to decrease capsular volume. 5 In one case, a bony Bankart was large enough to require internal fixation with an AO screw.
Arthroscopic Repair
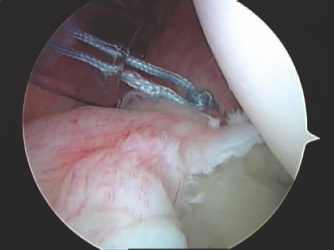
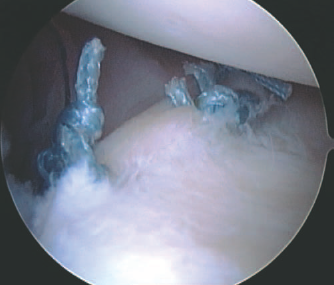
While visualizing from the anterior portal, the reverse Bankart lesion (Figure 1) was repaired with suture anchors or labral tacks.2,20 A spinal needle was used to localize the superolateral portal site (Figure 2). Dual posterior portals were used in all cases (Figure 3). Posteroinferior capsular redundancy was addressed with arthroscopic capsular plication to reduce the excessive volume (Figure 4). Crescent hooks (Linvatec Corp, Largo, Fla) were used to perform an arthroscopic capsulorrhaphy as described by Antoniou et al 2 and Wolf and Eakin. 36 Specifically, the capsule was first abraded with a nonaggressive mechanical shaver. A curved suture hook was used to pass a No. 0 polydioxanone suture (PDS, Ethicon, Somerville, NJ) that served as a suture shuttle. The suture hook pierced the capsule 1 cm lateral to the labrum. The capsule was then shifted cephalad and sutured to the labrum to effect a capsular shift (Figures 5 and 6). In 3 cases, capsular redundancy was addressed with thermal energy.
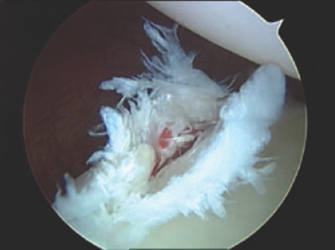
Arthroscopic image of a typical traumatic posterior (reverse) Bankart lesion visualized from an anteroinferior portal.
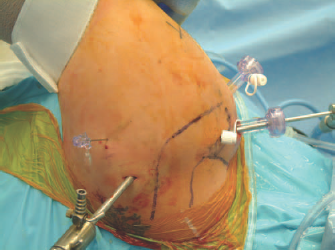
Picture of a left shoulder in the lateral decubitus position with a standard posterior arthroscopic viewing portal and a needle used to localize the superolateral accessory portal to assist in posterior Bankart repairs.
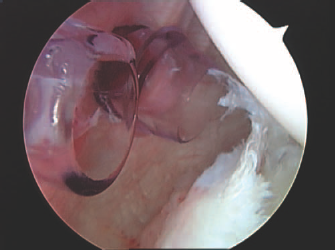
Dual posterior cannulas inserted to assist with suture passage and management during posterior Bankart repair.
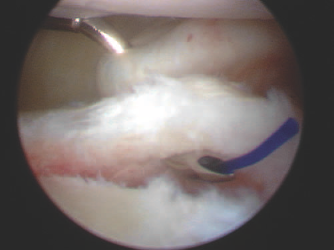
Curved (45°) suture hooks to perform a capsular plication of the posteroinferior capsule while repairing the labral defect.
Completed knot posteroinferiorly.
Completed repair of posterior Bankart.
Closure of the rotator cuff interval was also performed as described by Stokes and Savoie.30,33 The anterior cannula was backed out just outside the joint. A straighter crescent hook was used to pierce the superior capsule just anterior to the biceps tendon. A No. 0 PDS was delivered into the joint, and the hook was removed. A suture retriever was then used to pierce the middle glenohumeral ligament and retrieve the PDS. A sliding knot was used to close the interval, with the knot tied external to the capsule.
Postoperative Care
Postoperatively, shoulders were placed in a shoulder immobilizer (Cryo/Cuff, Aircast Inc, Summit, NJ) in 29 cases and a “gunslinger” brace to maintain neutral rotation in 2 cases. The patients were immobilized for 6 weeks with only pendulum exercises allowed. After initial immobilization, rehabilitation focused on restoring a full range of motion and strengthening the external rotators. Stretching of the posterior capsule by internal rotation was avoided for 4 months. Return to full activities was usually allowed at 6 to 8 months postoperatively.
Results
Between May 1996 and February 2002, 31 shoulders in 30 patients underwent posterior stabilization. There were 29 men and 1 woman. The mean age was 23 years (range, 15–39 years). All patients reported a traumatic posterior injury leading to the instability. The injury was a fall on an outstretched arm in flexion and adduction during a sports competition or a direct contact sports injury in 29 shoulders, and 3 injuries were the result of a motor vehicle accident. On initial presentation, all patients reported a feeling of instability with forward humeral elevation and internal rotation. The provocative “jerk test” had positive results in all 31 shoulders.5,22 Crepitation was often present during the posterior load-shift maneuver with the humerus in neutral or internal rotation. Examination in the clinic, subsequently confirmed under anesthesia, revealed 2+ or 3+ posterior translations that were asymmetric from their contralateral shoulders. Preoperative radiographic and MRI studies revealed reverse Bankart lesions, posterior rim fractures, or rim calcification in 30 (97%) of the cases. All but 3 patients underwent a formal course of rehabilitation before surgery. One patient had a bony Bankart lesion that required fixation, and 2 patients had gross posterior instability after injury.
The mean time between injury and surgery was 21 months (range, 1–152 months). Operations were performed with the patient in the lateral decubitus position in 17 shoulders and in the beach-chair position in 14 shoulders. Nineteen shoulders were stabilized arthroscopically and 14 by an open technique using a posterior approach. Arthroscopic stabilization was performed with suture anchors, permanent sutures, and capsular plication in 12 shoulders. Arthroscopic bioabsorbable tacks were used in 5 shoulders, with thermal capsulorrhaphy augmentation in 2 of these cases. Traditional open capsulorrhaphy with labral repair using suture anchors was performed in 11 shoulders. A posterior bony Bankart fixation was repaired with a single-screw fixation in 1 shoulder.
Four of the 31 shoulders had previous operations performed on the same shoulder. These operations included anterior stabilization procedures (Magnuson-Stack and Bankart repairs) in 2 patients and arthroscopic anterior stabilization or superior labral anterior posterior lesion repair in 2 patients. These patients had a remote history of a different episode of trauma resulting in recurrent anterior instability necessitating an anterior stabilization procedure. These patients had successful outcomes after anterior surgery until sustaining a new posterior injury requiring posterior stabilization.
The mean follow-up was 40 months (range, 24–63 months). The results of the postoperative evaluations are summarized in Table 1. The mean WOSI scores for the arthroscopic and open groups were 190 and 594, respectively (lower scores represent less disability and are therefore better outcomes). This difference was statistically significant (P <. 03). Similarly, the Rowe scores averaged 92 for the arthroscopic group and 80 for the open shoulders. This difference was also significant (P <. 04). The mean SANE and SST scores for the arthroscopic shoulders were also better than the open shoulders, but these did not reach statistical significance (P =. 06 and P =. 057, respectively).
Mean Postoperative Scores for All Patients a
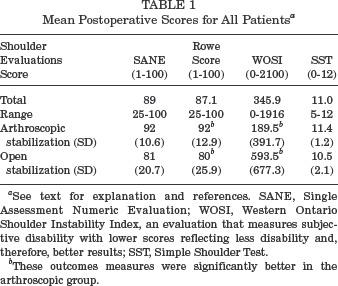
See text for explanation and references. SANE, Single Assessment Numeric Evaluation; WOSI, Western Ontario Shoulder Instability Index, an evaluation that measures subjective disability with lower scores reflecting less disability and, therefore, better results; SST, Simple Shoulder Test.
These outcomes measures were significantly better in the arthroscopic group.
Twenty-six of 31 shoulders were rated as good or excellent using the criteria of Wolf and Eakin. 36 There were 2 poor outcomes in this study. One outcome was an arthroscopic failure resulting in recurrent instability that required revision open posterior Bankart repair. This case involved tack fixation of the labrum with electrothermal capsulorrhaphy augmentation. There was 1 case of recurrent instability in the open group. There were 3 fair results in the study, 1 in the open group and 2 in the arthroscopic group, repaired with a bioabsorbable tack in one and suture anchors in the other. These fair outcomes were secondary to limitations in activity and subjective pain.
Discussion
Occurring much less commonly than anterior instability, posterior glenohumeral instability has been reported to occur in 2% to 5% of all patients with shoulder instability.11,12,21 As reviewed by Bell and Noble 3 more than a decade ago, posterior shoulder instability has been described as one of the more complex shoulder problems confronting surgeons. Posterior shoulder instability has been classified into acute and chronic by Hawkins and Belle,12,13 with chronic posterior shoulder instability being subdivided into locked (missed), recurrent voluntary, and recurrent involuntary subluxation. 21 The acute subgroup was further divided into those with and those without an impression defect (reverse Hill-Sachs lesion). Those patients with multidirectional instability or an underlying condition of ligamentous laxity, inherent or acquired, as is the case of an overhead-throwing athlete whose primary direction of instability is posterior, represent another type of patient presenting with posterior instability.4,5,25
The classic literature has reported an increased recurrent instability rate, postoperative pain, and a significant decrease in functional level after surgical treatment of posterior instability when compared to operative treatment for the more commonly seen anterior instability.11–13,25,26 In addition, as stated, the presenting symptoms in patients with posterior shoulder instability can be extremely varied. This variation has made the diagnosis and subsequent treatment complicated and has led to an appropriate degree of caution and nonoperative management. When rehabilitation fails, however, a number of surgical techniques have been used to address this problem. Except in the rare instances of bony abnormalities of the glenoid, the mainstay of operative treatment for recurrent posterior subluxation has been to reduce capsular laxity by shifting and augmenting the thin, patulous posterior capsule.4,5,7,11–16,35,36 Historically, reports of surgical treatment for this problem have indicated a low incidence of posterior labral, articular, or rim lesions. However, this incidence has been challenged by more recent reports and has been noted to be even more applicable in patients who present with a history of trauma or athletic injury.2,20,31,32,35
Fifteen years ago, Tibone and Ting 31 recognized a subset of athletes with posterior instability who presented with a definite history of trauma and whose pathoanatomy at surgery was similar and analogous to the abnormalities found in patients with anterior instability but located posteriorly. 31 These patients were treated with open posterior staple capsulorrhaphy. Although these patients had a 30% recurrence rate, this series described a unique presentation of patients with posterior shoulder instability not yet appreciated in the sports medicine community.
Hawkins and Janda 13 reported on 14 patients treated with an open posterior “capsulotendinous tensioning” procedure for recurrent posterior instability. Although 7 of these patients reported a history of trauma precipitating the instability symptoms, only 1 of the 14 had a labral detachment posteriorly that required repair. Other types of posterior labral abnormality were not described. Postoperatively, these patients reported mild to moderate pain with work or sports; however, 13 of the 14 stated they would have the surgery again. It would appear that although half the patients reported a traumatic onset, the underlying abnormality in this series was capsular laxity.
Bigliani et al 4 described their results of open posteroinferior capsular shift in 34 patients with recurrent posterior glenohumeral instability. The authors classified the instability into 3 types, with only 6 shoulders being unidirectional and posterior; 7 classified as bidirectional, posterior, and inferior; and 22 classified as multidirectional, posterior, and anterior. Although identifiable trauma was reported in 27 patients, only 13 patients had labral lesions, and complete detachment was noted in just 4 cases. The authors concluded that capsular redundancy and excessive capsular volume were the primary abnormalities, which were treated with a procedure that eliminated a patulous capsule.
In stark contrast to several of the previously cited works, Mair et al 20 described a homogeneous group of 9 patients who presented with posterior shoulder pain after a posteriorly directed load to a forward elevated, adducted upper extremity in collision athletes. They proposed the labral injury occurred with the arm forward elevated and adducted, creating a shear force. The authors stated that none of their patients had any laxity. All these cases had frank labral detachments with no appreciable asymmetric posterior translation when compared with the normal shoulder. The shoulders were successfully treated with bioabsorbable tack fixation of the posterior labral detachment alone. No capsulorrhaphy was performed. Mair et al 20 reported excellent results in this small series.
Misamore and Facibene 24 also reported on 14 athletes with unidirectional posterior instability. Their purpose was to report their results of open posterior shift in a small group of athletes with a specific pattern of posterior instability. They described a single episode of trauma that resulted in the instability in 11 patients and a gradual onset with repetitive axial loading in 3 patients. At surgery, fraying or splitting of the posterior labrum was noted in 7 patients, no abnormality in 3 patients, and only 1 patient with a so-called reverse Bankart lesion. With an open posterior capsular shift procedure, 13 of 14 patients had no instability or residual apprehension. Antoniou et al 2 described a group of 41 patients with posterior shoulder instability. Seventy-eight percent of their patients described an injury that led to recurrent instability. These patients had posterior apprehension, pain with posterior stress, and a characteristic “jerk” test with the arm at 90° of forward elevation and internal rotation. These patients were a mixed group of athletes and laborers but had “glenolabral concavity” lesions in common. Antoniou et al 2 described 4 types of lesions, including labral tears/splits, detachments, and articular defects, which were observed in 83% of their cases. The shoulders were all treated with arthroscopic repair of their labral lesions and “capsulolabral augmentation,” which involved using a suture hook and monofilament suture to perform a capsular plication to the labrum. Based on their own laboratory work, the authors reasoned that by combining capsular shift to the repair or augmentation of the labrum, it would deepen the posterior glenoid concavity, thus enhancing postoperative stability. Thirty-five patients had improved stability, and there were significant improvements in the SST and Short Form–36 scores. They concluded that posteroinferior instability can be associated not only with capsular laxity but also with well-defined lesions of the glenolabral concavity.
Williams et al 35 recently reported on a series of 26 patients with traumatic posterior instability whose mechanism of injury and pathologic findings were very similar to ours. They reported elimination of pain and instability in 92% of patients repaired with arthroscopic bioabsorbable tacks. Most recently, Kim et al 17 reported on 27 patients with posterior instability treated with arthroscopic stabilization. Based on the University of California, Los Angeles, rating score, 8 26 of 27 patients (96%) were rated as good or excellent. It is clear from the existing literature that the clinical problem of posterior shoulder instability can present with a wide spectrum of instability patterns. Mode of onset, physical examination characteristics, and observed gross pathologic lesions can vary. From a review of the operative series pertaining to this topic, many reports involve patients with different types of posterior instability, including those with bidirectional and multidirectional instability. This difference may explain why the results of surgery, with some authors reporting a failure rate as high as 50%, have not been as favorable as results of anterior instability surgery.
We believe, as do others, that traumatic posterior shoulder instability that develops after athletic or low-energy trauma represents yet another mode of presentation within the spectrum of patients with posterior instability. In contrast to the traditional classification previously reviewed, our patients reported a distinct history of trauma. In our study, it was typically a posteriorly directed force on the forward-flexed, adducted upper extremity. It has been reported that the patient with traumatic posterior instability often describes vague pain or weakness with this provocative position rather than true apprehension or a feeling that the shoulder is “coming out of the joint.” In contrast, we noted posterior apprehension in all of our patients who underwent operative repair. Provocative tests to assess posterior stability should be included and were helpful in making the diagnosis in our series. The jerk test and the posterior stress test were employed to elicit posterior instability.2,12–14,20,21 Zarins and Rowe21,27 suggested that an examination under anesthesia or fluoroscopic examination may be of benefit in establishing a diagnosis. However, with the addition of MRI, posterior capsulolabral injuries can be diagnosed with a great degree of accuracy. In our series, MRI was helpful in confirming the diagnosis of posterior labral lesions.
No patients with a diagnosis of multidirectional instability were included in our study. In addition, none of our patients reported a history of posterior dislocation or subluxation before their index injuries. However, in our group of collision and military athletes, there were 4 patients who had a history of trauma to their shoulders leading to prior anterior stabilization or superior labral repair that was successful. This study featured a group of patients with a distinct traumatic cause leading to recurrent posterior instability and dysfunction. Furthermore, preoperative imaging to include plain radiography, MRI, and arthroscopy disclosed posterior labral tears, detachment, and humeral head lesions in 91% of our cases. These pathologic findings are very consistent with the report of Tibone and Ting, 31 in which all 10 patients had posterior labral detachments, and closely follow the previously described work by Antoniou et al, 2 who used arthroscopy to confirm an 83% incidence of lesions of the glenolabral concavity. In addition, the recent reports of Williams et al 35 and Kim et al 17 corroborate our findings.
The surgical treatment in our series focused on the pathoanatomy of posterior labral lesions and on addressing capsular laxity. Early in this series, patients were treated with open surgical techniques. As we gained experience with the arthroscopic technique and were convinced that we could perform labral repair and capsular plication in a manner similar to open surgery, arthroscopic reconstruction became the procedure of choice. The advent of arthroscopic techniques that permit the placement of suture anchors with nonabsorbable sutures and plication of the capsule similar to that which is done in the open technique may lead to improved results with less morbidity. We agree with the concept of capsulolabral augmentation by restoring the glenolabral anatomy while performing an arthroscopic capsular plication. Furthermore, as Wolf and Eakin 36 described, arthroscopy permits excellent visualization of the joint and all pathologic lesions, which may lead to improved surgical precision. In addition, arthroscopic methods permit closure of the rotator cuff interval. The structures of the rotator cuff interval, the coracohumeral and superior glenohumeral ligaments, have been studied and have been determined to be important in providing posterior glenohumeral stability.9,10 The ability to restore tension in the coracohumeral ligament and superior glenohumeral ligament by closing the interval, a difficult task through an open posterior approach, may be an advantage to the arthroscopic technique. Future research and long-term follow-up of this arthroscopic technique will be necessary to validate this concept.
One of the strengths of this study includes the use of several different shoulder outcomes instruments to assess our patients’ shoulder function preoperatively and after surgery. It is our opinion that surgical results after shoulder instability should be more comprehensive and extend beyond the single-outcome measure of postoperative instability. Most of these measures were developed to assess function and stability after anterior procedures; however, we applied them to assess results for posterior instability as well. The WOSI is a validated and reproducible instrument used to assess shoulder stability. 18 To our knowledge, this measure has not been previously applied to posterior instability.
We readily acknowledge the inherent limitations of this retrospective review. The number of patients was relatively small, representing the infrequent occurrence of these injuries compared to anterior instability. Our goal was to present the results of posterior stabilization in a definable subgroup of patients with traumatic, recurrent posterior instability. Although not as favorable a surgical treatment for anterior instability, posterior stabilization for traumatic posterior instability led to a favorable outcome in the majority of cases of young military athletes and soldiers, a group with extremely high demands.
In summary, patients with traumatic posterior instability often describe a collision or fall with the arm in a forward-flexed, adducted, and internally rotated position. This is a common position for blocking linemen or throwers in their follow-through phase. In our study, this problem was observed in other collision sports, such as lacrosse and hockey, or after a fall in cadets during the military obstacle course. In addition, we found several patients in our series who were injured during motor vehicle accidents and who recalled injuring their shoulders when attempting to brace themselves during a collision with the arm in a flexed, adducted, internally rotated position. With a clear, distinct history of trauma, supported by a provocative examination, these patients will have definable lesions involving the posterior capsulolabral complex. Surgery focused on anatomical repair of these lesions, leading to improved results and allowing most of our patients to return to preinjury levels of activity.