
Abstract
Background: Researchers have investigated the performance of face mask removal tools for spine injury management in football but not the effects of football equipment design.
Hypotheses: Various styles or designs of football helmet equipment (helmets, face masks, loop straps) affect face mask removal efficiency. A cordless screwdriver performs more efficiently than do cutting tools.
Study Design: Controlled laboratory study.
Methods: Nineteen certified athletic trainers were randomly assigned to group 1 (cordless screwdriver and the FM Extractor) or group 2 (cordless screwdriver and the Trainer’s Angel). Subjects randomly performed face mask removal for 6 conditions composed of helmet (3), face mask (3), and loop strap (5) combinations. Time, head movement, perceived difficulty, and success rates were measured.
Results: Multiple significant differences were found in time, movement, and perceived difficulty between the 6 helmet equipment conditions. The Shockblocker loop strap was consistently superior in all variables regardless of the tool used or the helmet it was attached to. The cordless screwdriver created less movement (mean range from any one plane, 2.8°-13.3°), was faster (mean range, 42.1-68.8 seconds), and was less difficult (mean rating of perceived exertion range, 1.4-2.9) compared to cutting tools (ranges, 4.4°-18.4° in any one plane, 71-174 seconds, rating of perceived exertion, 2.8-7.7). Trial failure was more common with cutting tools than with the screwdriver.
Conclusion: Differences in football helmet equipment affect face mask removal. The cordless screwdriver is more efficient than the FM Extractor and Trainer’s Angel.
Clinical Relevance: Professionals responsible for the care of football athletes must be knowledgeable in the types of equipment used and the best option available for effective airway access.
Because of the potentially catastrophic and life-altering consequence of spine injury (SI), there is understandable concern regarding the evaluation, prehospital management, and care of the cervical spine–injured athlete. Sports medicine professionals who are presented with an SI must manage the situation in a safe and effective manner, in as short a time as possible. This management becomes even more critical in the athlete who participates in equipment-intensive sports such as football, in which there are barriers to obtaining immediate access to the athlete's airway. Because the removal of football helmets has been shown to take the cervical spine out of neutral alignment,9,21,26 it is recommended that helmet and shoulder pads remain in place and that the face mask be removed to obtain airway access. 15 In such situations, today's standard procedures involve cutting the loop straps that attach the face mask to the helmet. 15 The objective in removing a face mask is to cut the loop straps in as short a time as possible while minimizing movement of the head and neck. Research is limited in this area, having primarily focused on the cervical spine position when equipment is removed9,21,26 or the performance of face mask removal tools.12,16,22,24,25
Football helmets must meet specific standards set forth by the National Operating Committee on Standards for Athletic Equipment (NOCSAE). These standards have been set in an effort to reduce head trauma. However, it is that same protective equipment (the helmet, face mask, and loop straps) that impedes airway access after a potentially catastrophic injury. To our knowledge, no research has reported whether the design of football equipment (ie, different brands, styles, or designs) has a deleterious effect on the ability to gain airway access during an SI. In addition, with recent changes and modifications in helmet and face mask design, it is imperative to determine if the design itself will hinder proper and efficient management of a suspected SI.
In 2001, the Inter-Association Task Force for Appropriate Care of the Spine-Injured Athlete (IATF) provided clinicians with specific recommendations regarding face mask removal. 15 These recommendations were based on the research available at the time. Unfortunately, previous research reported findings based on tool performance in only one helmet, face mask, and loop strap combination. Realistically, there are dozens of possible combinations of shells, face masks, loop straps, and associated hardware that an athlete may wear. This variation creates countless possibilities and unforeseen emergency situations for the sports medicine professional for which generic recommendations may not be suitable.
Therefore, the purpose of this study was to analyze the efficiency (ie, time, movement, and difficulty) of face mask removal using various styles of helmets, face masks, and loop straps. In addition, 3 styles of face mask removal tools were used to determine which tool(s) should be used for specific component combinations. Grip strength, hand width, and hand length were also recorded to identify any relationships between these subject characteristics and face mask removal performance.
Materials and Methods
Subjects
Subjects consisted of 19 (12 men, 7 women) National Athletic Trainers’ Association Board of Certification certified athletic trainers (ATCs) from the local community. The mean age of participants was 31.7 ± 9 years, and the mean level of experience as an ATC was 7.9 ± 7.7 years. All subjects signed an informed consent form approved by the university's Institutional Review Board. All subjects were healthy and without upper extremity injury or neuromuscular dysfunction.
Instrumentation
A Motion Analysis Inc (Santa Rosa, Calif) 6-camera (60–240 Falcon), EVa Hi-Res three-dimensional (3D) kinematic motion capture system with a sampling rate of 120 Hz was used to collect the movement data for this investigation. Using a conventional X, Y, Z laboratory coordinate configuration, the motion capture system tracks the 3D movement of retro-reflective markers in a calibrated volume. The 6 cameras were strategically placed surrounding a 3 × 7-m motion capture volume at a height of approximately 2.5 m to decrease the likelihood of markers being obscured from view during data collection. Before each data collection session, the volume was calibrated using a cube and wand calibration technique. The Motion Analysis Inc system has been widely used for scientific and technical purposes, and the reliability and validity have been established and reported in the literature. 23 Kinematic data were smoothed using a fourth-order 2-pass Butterworth filter (7 Hz). Orthotrak 4.21 (Motion Analysis Inc) software was used to measure the movement produced during the task.
Hand measurements were assessed using a Lafayette Instrument Co caliper (Lafayette, Ind). Hand length was defined as the distance from the distal crease of the wrist to the distal aspect of the third finger on the palmar aspect. Hand width was quantified as the distance across the hand at the second through fifth metacarpophalangeal joints. Grip strength was evaluated using a Lafayette Analog Grip Tester (Lafayette Instrument Co). Time for task completion was measured using a digital stopwatch. Trials were videotaped using standard camcorders from both lateral and frontal views for subjective observation after data collection.
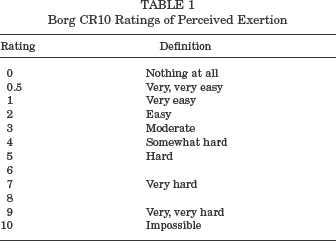
The Borg category-ratio CR10 scale was used to assess the difficulty of each condition (Table 1). The CR10 is a scale for measuring the intensity of sensation and subjective somatic symptoms, and it provides a general method of measuring most kinds of perceptions and experiences, including pain and perceived exertion. 3 A rating of perceived exertion (RPE) is commonly determined in clinical diagnostics, therapy and rehabilitation, fitness and performance enhancement training, and epidemiologic evaluations of exercise intensity and daily physical activities.5,6,10,14
Borg CR10 Ratings of Perceived Exertion
Three tools were used for face mask removal (Figure 1). The cordless screwdriver (SD; Black and Decker, Towson, Md), the FM Extractor (FM; Sportsmedicine Concepts Inc, Rochester, NY), and the Trainer's Angel (TA; Trainer's Angel, Riverside, Calif) were selected for use in this investigation, secondary to their prevalence in previous research12,16,22,24,25 and wide use in the field.
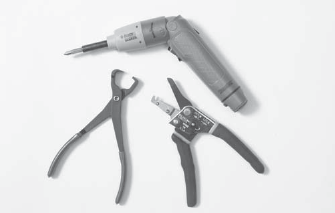
Face mask removal tools, counterclockwise from the top: cordless screwdriver, Trainer's Angel, and the FM Extractor.
Two major manufacturers of football helmets were contacted to identify the helmets and face masks that are most commonly used and purchased by football programs across the United States and, therefore, the most likely styles that medical personnel would come in contact with in an emergency situation. Also included in the study were several new products expected to become more prevalent among football programs. The 3 helmets included were the Schutt Air Advantage (Schutt Sports, Litchfield, Ill), the Riddell VSR-4 (Riddell, Elyria, Ohio), and the Riddell Revolution. Standard face masks and loop straps were chosen to match each manufacturer's helmet. In addition, numerous types of loop straps are commonly used in place of the standard manufacturer's loop straps. The Shockblocker (Maxpro, Marietta, Ohio) and Stabilizer II (Innovative Co, Cleveland, Ohio) loop straps are unique in design and were therefore included in this investigation in addition to standard manufacturer's loop straps (Figure 2).
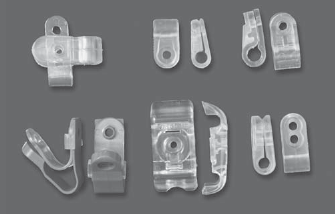
Face mask loop straps, clockwise from top-left: Stabilizer II for thin-wire mask, Revolution top straps, Schutt Armorguard Elite, Riddell standard, Revolution side-slotted straps, and Maxpro Shockblocker.
Each helmet used for data collection was adjusted and properly fit to a laboratory assistant based on manufacturer's guidelines. The assistant also wore a properly fitted pair of shoulder pads (Air Pac AP57, Riddell) and served as the model for all data collection. Each of the helmets used was permanently fitted with a video marker set consisting of 3 metal brackets that extended from the helmet's shell in a triangular fashion and supported reflective markers (Figure 3). This arrangement of markers allowed the motion capture system to track the 3D movement of the head relative to the laboratory coordinate system.

Helmet marker setup.
Procedure
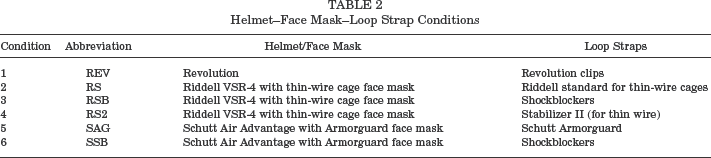
Subjects were randomly assigned to 1 of 2 groups using a Latin square. Group 1 (n = 9) used only the FM to cut the loop straps, and group 2 (n = 10) used only the TA to cut the loop straps. Both groups used the cordless SD to remove the screws. We decided to use a between-groups design after pilot testing. Using 4 subjects (1 of the authors, 2 student athletic trainers, and 1 ATC), it was discovered that having subjects perform the necessary number of trials for all conditions using all 3 tools was extremely difficult. Subjects reported fatigue, delayed soreness, and blisters. By removing one of the cutting tools and separating the trials out over 2 sessions, subjects were able to complete the trials without fatigue in a timely manner. An analysis of variance confirmed baseline similarity of the groups, showing no significant difference in age, years of experience, grip strength, hand width, or hand length (P > .05). All subjects completed the face mask removal tasks over 2 separate data collection sessions to reduce fatigue. The 2 sessions were separated by a minimum of 48 hours and no more than 7 days. Six helmet, face mask, and loop strap combinations created the conditions for testing (Table 2). The order of the 6 testing conditions was randomized and counterbalanced using a Latin square. Group 1 (FM and SD) was presented with 12 face mask removal conditions. Group 2 (TA and SD) was presented with 11 face mask removal conditions, 1 fewer because the TA cannot cut the Riddell Revolution side loop straps.
Helmet–Face Mask–Loop Strap Conditions
During the initial data collection session, the study and procedures were explained to the subject. On fully understanding the study, the subject signed the informed consent document. Subjects then completed a demographic questionnaire, and hand length, hand width, and grip strength were assessed. Subjects were then asked to read the manufacturer's instructions for each of the specialized face mask removal tools and, when available, instructions provided by the helmet manufacturer regarding removal of the face mask.
Subjects practiced the task of face mask removal for each of their assigned conditions under direct supervision of a researcher who provided feedback to improve face mask removal efficiency. Subjects continued to practice until they demonstrated comfort and proficiency with the SD and cutting tool in each of the conditions. After demonstrating proficiency, subjects were required to rest for 15 minutes.
After the 15-minute rest period, each subject performed 2 trials of face mask removal for each of the conditions randomly assigned to that testing session. The laboratory assistant, wearing the appropriate helmet–face mask–loop strap combination, lay supine in the designated video-collection volume. Each subject was provided a new tool at the beginning of testing, and that tool was used by the subject throughout data collection for all cutting tasks. A fully charged battery was inserted into the SD at the start of each session. The appropriate tool for each trial was placed to the side of the model's head, and the subject was positioned with the knees stabilizing the helmet. Subjects were instructed to cut or unscrew the side loop straps first and finish with the top 2 loop straps. The subjects were also instructed to stabilize the head and complete the task as quickly and with as little movement as possible. Timing of each trial began when the subject picked up the tool and ended when the face mask was completely removed from the helmet. After each trial, new loop straps were installed for each cutting tool trial, and new stainless steel screws, T-nuts, and washers (Schutt helmets only) were installed for each SD trial. Each screw was installed using a 7.2-V, heavy-duty, adjustable torque cordless SD (model DW920, Dewalt, Co, Baltimore, Md) set at a standard torque setting (No. 7) throughout the study. Motion data were collected for 60 seconds during the SD trials, 75 seconds during the FM trials, and 101 seconds during the TA trials. These times were identified in previous studies to be the mean time required for each tool to remove a standard face mask and loop strap combination.12,22,24,25 Trials were kept to a 4-minute maximum to decrease the potential effects of fatigue. In addition, it has been shown that resultant brain injury is time dependent, and if a victim has not been resuscitated after 4 to 5 minutes after the cessation of blood circulation, irrecoverable brain damage is likely.2,13 We felt that medical personnel would resort to alternative means (helmet removal, intubation, or pocket mask insertion) in this situation. Hence, allowing our subjects to attempt face mask removal for longer than 4 minutes was not deemed appropriate. On completion of each trial, the subject was asked to rate the difficulty of the task by providing the investigator with a number from the CR10 scale (0–10; see example in Table 1). The above-described procedure continued for all conditions assigned to session 1. During the second data collection session, subjects again practiced and performed face mask removal for each of the conditions assigned to that session in the same manner as for session 1.
Three primary variables were analyzed for the study: (1) time to complete the task, (2) the range of motion (ROM) created in 3 planes (lateral flexion, flexion-extension, and rotation) during the task, and (3) a rating of difficulty for the task (RPE). The ROM was calculated as the difference between maximum and minimum angles produced in all 3 planes. In addition, we recorded the number of times a trial failed and classified each failure into 1 of 4 categories. The 4 categories of failure were defined as follows: (1) exceeding the 4-minute maximum, (2) helmet equipment failure (screw and T-nut spinning or screw head stripped), (3) tool failure, and (4) other/miscellaneous.
Statistical Analysis
An a priori sample size analysis was performed based on the conditions as follows: a level of .05, power level of .80, and expected effect sizes ranging from 0.75 to 1.0. This analysis produced a recommended sample size of 11 to 16 trials per condition. A single-factor multiple analysis of variance for repeated measures was used to test for the main effects for each of the helmet/face mask conditions within each tool type and for each of the tool types across each helmet/face mask condition. Post hoc tests were performed as needed with Bonferroni correction. Significance was accepted at a level of P < .05. Pearson product moment correlation coefficients were performed to explore any relationship between grip strength, hand width, and hand length and the dependent variables. Significance was accepted at an a level < .05. All statistical analyses were performed on SPSS version 11.0 (SPSS Science Inc, Chicago, Ill) for Windows.
Results
All 19 subjects reported to both data collection sessions for the study. One hundred percent of the assigned TA conditions (50/50) and 97% (50/54) of the assigned FM conditions were attempted. The 4 conditions not attempted for the FM were due to failure of the tool, which precluded subjects from performing trials for the remaining FM conditions assigned. Because all subjects from both groups were assigned to perform all conditions using the SD, there were twice as many SD conditions assigned as there were for the cutting tools. For logistical reasons only, such as subject time constraints, it was necessary to randomly drop SD conditions from the data collection. This exclusion made the total number of the SD conditions attempted to be 89, considerably more than those attempted for the TA and FM and sufficient to meet the a priori goal for the statistical comparisons even though the original Latin squares assignment called for 114 SD conditions. In addition, the subsample size (n) of 89 for the SD, or 100% of the SD conditions attempted, was the basis for the calculation of success rates.
For the comparison of helmet–face mask–loop strap conditions within each tool type, the analysis of the SD revealed statistically significant differences in lateral flexion ROM and flexion-extension ROM (Table 3). The remaining dependent variables, time and RPE, had nonsignificant differences among the conditions. The analysis of the FM showed statistically significant differences between helmet–face mask–loop strap conditions in time to completion and RPE (Table 4). There was no significant difference for movement variables between the conditions when the FM was used. The analysis of the TA across all helmet conditions demonstrated statistically significant differences in time to completion and RPE (Table 5). The movement variables showed nonsignificant differences among the conditions when the TA was used.
Means ± SDs and Effect Sizes for Time to Complete Task, Rating of Perceived Exertion, and Movement Variables for All Conditions Using the Cordless Screwdriver
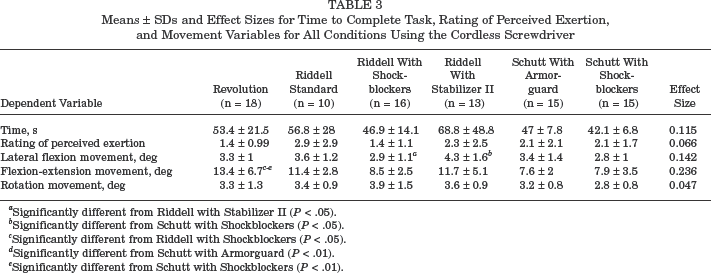
Significantly different from Riddell with Stabilizer II (P < .05).
Significantly different from Schutt with Shockblockers (P < .05).
Significantly different from Riddell with Shockblockers (P < .05).
Significantly different from Schutt with Armorguard (P < .01).
Significantly different from Schutt with Shockblockers (P < .01).
Means ± SDs and Effect Sizes for Time to Complete Task, Rating of Perceived Exertion, and Movement Variables for All Conditions Using the FM Extractor
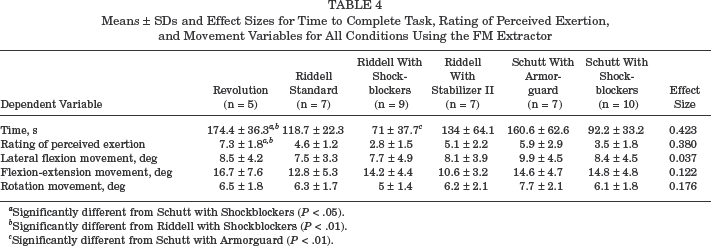
Significantly different from Schutt with Shockblockers (P < .05).
Significantly different from Riddell with Shockblockers (P < .01).
Significantly different from Schutt with Armorguard (P < .01).
Means ± SDs and Effect Sizes for Time to Complete Task, Rating of Perceived Exertion, and Movement Variables for All Conditions Using the Trainer's Angel
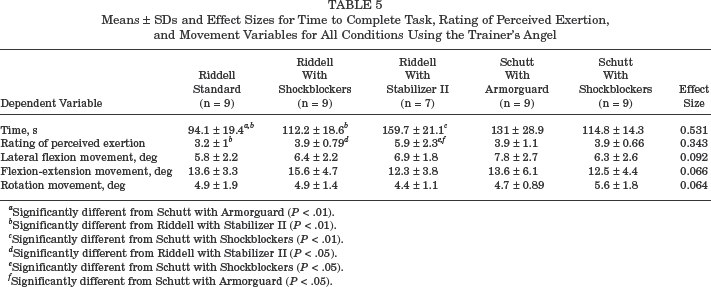
Significantly different from Schutt with Armorguard (P < .01).
Significantly different from Riddell with Stabilizer II (P < .01).
Significantly different from Schutt with Shockblockers (P < .01).
Significantly different from Riddell with Stabilizer II (P < .05).
Significantly different from Schutt with Shockblockers (P < .05).
Significantly different from Schutt with Armorguard (P < .05).
The analysis of the 3 tools for each condition indicated that the SD had the shortest time to completion compared to the FM and/or the TA for all the tested conditions. The SD had the lowest RPE for all the conditions and was significantly less than at least one of the cutting tools in all conditions except for the Riddell standard helmet and loop strap (RS) condition. The SD produced the least lateral flexion ROM and the least rotational ROM in all 6 conditions, and it produced the least flexion-extension ROM in 4 of the 6 conditions. Means and standard deviations of all the tools for each condition, the comparisons, and the corresponding effect sizes are summarized in online Appendices 1 through 6 (available in the online version of this article at www.ajsm.org/cgi/content/full/33/8/1210/DC1).
The mean grip strength for all subjects was 44 ± 10 kg, the mean hand width was 8.3 ± 0.7 cm, and the mean hand length was 18.3 ± 1.2 cm. No significant correlations were found between grip strength, hand length, and hand width and the dependent variables (P > .05). Ranges for grip strength correlations with the dependent variables were r = –0.13 to –0.16; for hand length, r = –0.003 to –0.22; and for hand width, r = –0.025 to –0.32.
The success rate for all of the trials was tracked, and the reason for failure to complete a trial was tallied (Table 6). A total of 384 trials were attempted. Of these 384 trials, 344 or 89.6% were successfully completed. The most common reason for trial failure was exceeding the 4-minute time limit. This occurred 25 times or 6.5% of the total number of trials; all 25 time-limit failures involved cutting tools. Nineteen of those 25 failures involved either the Revolution–Revolution loop strap (REV) condition or the Riddell VSR-4 helmet–Stabilizer II loop strap (RS2) condition. Conditions involving the use of the SD failed on 8 (2.1%) occasions mainly because of stripping the head of the screws or the T-nut spinning with the screw, thus preventing removal.
Description of Trial Failure: Causes, Rates, and Conditions (N = 384)
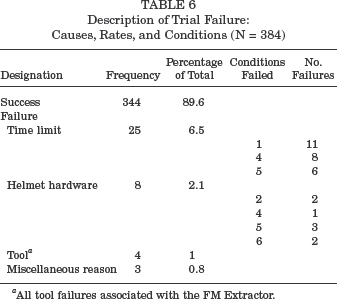
All tool failures associated with the FM Extractor.
Discussion
The primary objective of this investigation was to determine if different football equipment affects the ability to remove a face mask. Negative effects could be categorized as increased time or difficulty to complete the task or increased movement produced, with a potential consequence of worsening the patient's condition. Our results clearly demonstrated that certain helmet conditions (helmet, face mask, and loop strap combinations) were consistently easier, were faster, and produced less movement than other conditions and that the SD was a superior tool for the face mask removal task compared to the TA and FM. Finally, for some helmet conditions, the FM was more efficient than the TA, whereas in others, the reverse was the case.
The importance of avoiding or reducing negative sequelae associated with the management of injuries in the helmeted athlete makes it important to attempt to identify the causes for differences in movement, time, and difficulty of face mask removal. On careful observation of videotaped trials after completion of our study and careful inspection of the characteristics in the design of each helmet component, we can speculate with a fair degree of confidence why certain conditions allowed for more efficient removal than did others. For example, there was a significant difference in the time and difficulty in removing the face mask using the FM in the REV condition compared to the Riddell VSR-4 helmet with Shockblockers (RSB) and the Schutt with Shockblockers (SSB) conditions and a significant difference in flexion-extension ROM when using the SD in the REV condition compared to the RSB, SSB, and the Schutt with Armorguard loop strap (SAG) conditions. One possible explanation for the negative effects identified in the REV condition is the location of the Revolution helmet lateral loop straps relative to the shoulder pads. The increased proximity of the loop straps to the shoulder pads in this helmet–face mask combination made it exceedingly difficult for subjects to position the tool to unscrew or make an effective cut through the manufacturer's cutting slots (Figures 4A and B). Furthermore, in the case of subjects using the FM, each lateral Revolution loop strap requires a minimum of 4 cuts because of its design characteristics, whereas in traditional loop straps, it is possible to successfully cut through the strap in 1 attempt. In other words, a traditional helmet and loop strap design may be removed with as few as 4 cuts, whereas the REV condition requires a minimum of 10 cuts—4 per side and 1 cut for each of the top 2 loop straps. A similar situation may have been the reason the Stabilizer II loop strap was most difficult and took the most time when removing the face mask with the TA. A Stabilizer II loop strap has 2 separate attachments to the face mask bar, resulting in the necessity of performing a minimum of 6 cuts for the removal of the face mask. On the other hand, subjects took less time and felt the Shockblocker loop strap was less difficult to remove when using the FM compared to all other conditions. The unique design of the Shockblocker (2 thin layers: a soft inner layer and a rigid outer layer) is likely the reason for the quick and efficient cuts.
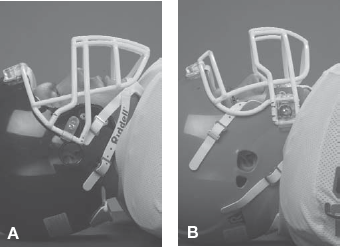
A, traditional-style helmet and location of the lateral loop straps relative to the shoulder pads. B, Riddell Revolution helmet and location of the lateral loop straps relative to the shoulder pads.
We are unaware of previous research that has specifically investigated the design of football helmets and associated equipment, as well as the effect these variables might have on the ability to remove a face mask; therefore, no comparison to the literature on that issue is possible. However, our results for tool comparisons were in general agreement with the literature.12,16,22,24,25 Although previous research has used varied instrumentation techniques and the majority have investigated face mask retraction (in which only 2 loop straps are cut or removed and the face mask is rotated up) as opposed to full removal, there are pertinent studies that have included analyses concerning the movement, time, and difficulty associated with the face mask removal (or retraction) task.
It is desirable to minimize head and neck motion as much as possible because it is not possible to predict a permissible amount of motion during cervical SI management. Thus, there have been studies that have attempted to quantify motion associated with the face mask removal task. In studies that have included a manual or cordless SD, it was found to be superior to cutting tools in minimizing movement created during the task.12,16,22 An early study on airway access techniques for the spine-injured football player compared the movement created between a manual SD, a cordless SD, and the TA. 22 Bike Air Power helmets (Bike Athletic Co, Knoxville, Tenn) were used in the investigation; the type of loop strap was not provided. Using an optoelectronic motion system, the investigators found that the TA created significantly more motion than did the SD; the results of our investigation were in agreement with these findings. Similar conclusions were reached in a study that fixed a standard helmet with Bike Athletic loop straps to a force plate and compared the torque applied to the helmet during face mask retraction between a TA, FM, SD, and a screw with a quick-release mechanism. 12 Because the helmet was fixed to the force platform, no movement was possible, and therefore we are unable to directly compare these data to our movement data. However, the investigators concluded that the SD was superior to the cutting tools because it created less torque at the head during the retraction process. 12 After the 2001 IATF Spine Injured Athlete document recommended full removal of the face mask rather than retraction, 15 researchers had 29 ATCs fully remove the face mask from a Riddell helmet with Armorguard loop straps using the FM, the TA, an anvil pruner (AP), and a PVC pipe cutter (PVC). 25 This study appears to be the only other 3D analysis using full face mask removal, as in our investigation. No differences were noted in ROM between these cutting tools, 25 similar to the findings in our study in which there was a significant difference found (rotation ROM) between the FM and TA in only 1 condition (SAG).
Vying for importance with the movement created during face mask removal, and clearly more immediately important with an anoxic athlete, is the time required to gain access to the airway. In the current study, the SD consistently demonstrated superior performance compared to the FM and TA across all 6 conditions. As is the case with movement comparisons, manual and cordless SDs have also been found to be either equal or superior to cutting tools in other research concerning the time associated with this task.12,16,22 Although our study included the SD in the analysis of full face mask removal, the first to do so, it is important to compare our findings with those of other studies that have investigated only cutting tools because the currently recommended face mask removal procedure calls for their use. 15 In a study using Schutt Armorguard loop straps fixed to a Riddell helmet, 24 4 tools (FM, TA, AP, PVC) were compared during face mask retraction. These researchers found the PVC and TA took significantly longer to complete the task than did the FM. 24 In a recent study comparing the times during retraction, the authors found the FM was significantly faster than the TA. 12 Finally, in another study in which subjects removed, rather than retracted, the face mask from a Riddell helmet with Armorguard loop straps, results indicated that the FM and AP were faster than the TA and PVC. 25 Our current findings for the cutting tools were consistent with the literature in that the FM was faster than the TA in 3 of the 5 helmet conditions, but at the same time, the results were inconsistent because in our study, the TA was faster than the FM for the SAG condition.
Another variable investigated through this study was the issue of the perceived difficulty of the task, quantified using the modified RPE. Gaining an understanding from subjects on their perceptions of the difficulty of the task provides another important perspective on the overall challenge faced during face mask removal. A type of preference rating, or satisfaction, has been a component of previous face mask removal research,16,24,25 although it has typically been specific to the subject's rating of the tool, rather than rating the difficulty of the entire task, which takes into account both the helmet condition and tool used. Regardless of the helmet and tool used, subjects generally felt the Shockblocker strap was the least difficult to remove except in 2 conditions (SSB and RS), in which there were no differences in the RPE scores. Also, when comparing RPE scores between tools for each condition, the SD was superior to the cutting tools, demonstrating the ease of completing the task with the SD. In 3 of 5 conditions, the FM was less difficult than the TA was. Results for this type of measurement have been consistent throughout the literature.16,24,25 Why subjects are more satisfied, prefer, or feel one condition is less difficult than another has not been established. It appears, both from our results and from the literature, that the most preferred tools or helmet conditions are those performing the best in time and movement variables, although this factor has not been demonstrated scientifically.
Finally, our findings for hand size and grip strength contradicted the commonly held theory that individuals with less grip strength and smaller hands will struggle more with cutting of the loop straps and removal of the face mask. Grip strength has been evaluated in activities such as climbing,8,11,20,31 bowling,28,29 sailboarding, 1 tennis, 17 judo, 27 and handgun marksmanship. 7 Each of these investigations found no relationship between grip strength and successful task performance. Our results agreed with the previous research, and we speculate that there are many variables that affect successful performance of the task. We suggest that technique, training, practice, body position, wrist position, 19 and familiarity with the equipment will all have a combined effect on successful performance of the task.
Recommendations
We recommend that an emergency responder choose to use a cordless SD as the primary option when face mask removal becomes necessary. In the event that the SD fails to remove one or more of the screws, a backup cutting tool must be available. It is vital, however, that the medical professional realize that the cutting tool that will perform the best will differ according to the specific football equipment in use. For example, cutting Revolution clips requires a tool with specific attributes, and this specificity precludes the TA from being the backup tool for Revolution helmets. Furthermore, although it is possible to cut the Revolution strap with the FM, the FM did not perform ideally, as the time to completion was excessive (mean time, 174 seconds; 4 trials > 4-minute maximum). For athletes wearing the Riddell standard, however, it appears the backup tool of choice should be the TA because the FM took slightly longer (24 seconds) and was rated as slightly more difficult. The FM also created significantly more lateral flexion ROM and rotation ROM compared to the SD. The choice of the TA as a backup tool for athletes wearing the RS2 combination could be defended but only with respect to the movement created, as the TA was slightly more difficult and took longer compared to the FM. In the 3 remaining conditions (RSB, SAG, and SSB), the backup tool of choice would be the FM.
When considering loop strap attachment options, we recommend the use of Shockblockers for the lateral attachments. This recommendation is based on the consistent ability of subjects to remove the face mask faster, with less difficulty, and with less movement compared to the other loop straps used in this study. We would not recommend using the Stabilizer II loop strap with respect to face mask removal. Currently, the only option for the Revolution helmet is the standard lateral Revolution loop straps. Because of the difficulty associated with cutting these loop straps, medical personnel should practice the technique of helmet removal as a backup to screw removal to ensure their ability to gain airway access for athletes wearing this helmet.
Finally, because there exist other possible combinations of helmets, face masks, straps, and cutting tools, both currently and to come in the future, sports medicine personnel at a given institution should practice removing the particular face mask–strap–helmet combinations that their team is using to decide what tools and techniques work best.
Limitations
In this study, the movement that was analyzed was that of the helmet. We make the assumption that this motion of the helmet results in comparable motion of the head 32 and that changes in head position result in significant changes in the space surrounding the spinal cord. 30 Although researchers have found a significant displacement of injured cervical segments in cadaveric specimens as a result of an airway management process,4,18 the exact relationship between head and cervical spine movement is unknown, and therefore, we can only speculate how motion of the head during face mask removal corresponds with movement of the cervical spine.
Our results only apply to the SD, TA, and FM and may not be generalized to other tools or other versions of these tools. Our study only included a sample of helmet equipment combinations, and therefore, results and recommendations may not be generalized to other equipment or equipment combinations. All of the helmets and associated equipment in this study were provided new and unused by the manufacturers. New loop straps and helmet hardware (stainless steel screws, T-nuts, and washers) were installed before each trial. This condition does not represent the actual status of helmets and associated hardware throughout a season. There is a commonly held belief that the possibility of screw failure will become more likely with increased use and environmental exposure, although research on used equipment has not been published to support or refute this contention. The potential impact from use and the environment throughout the course of a season on the quality of the equipment and its resultant effect on the variables and failure rates are unknown. This lack of knowledge further supports the importance for athletic trainers to regularly inspect helmet hardware and be prepared with an equipment-matched backup cutting device.
Conclusion
The results of this study revealed that variations in helmets and associated equipment can negatively affect the ability to gain access to the airway. The SD was less difficult to use and allowed subjects to perform face mask removal in less time and with less movement compared to the TA and FM. The Shockblocker loop straps allowed for more efficient face mask removal. Grip strength and hand size did not affect face mask removal efficiency.
Current guidelines suggest that face mask removal by cutting loop straps is the recommended technique to be used in the event airway access is deemed necessary. 15 Based on our results, face mask removal, particularly with a cutting tool, is a highly variable and sometimes impossible task to perform. Face mask removal by cutting alone may not be a clinically safe and reliable means of gaining airway access on an injured football player. The time required for unscrewing the face mask is reasonable, but questions about the reliability of screw function persist. Specific research is needed to determine the actual impact of use and the environment on the ability to remove screws from used helmets using an SD. Regular inspection and replacement of helmet hardware should be conducted. More research is also necessary to create specific guidelines and recommendations for face mask removal and equipment specifications. Likewise, governing authorities or organizations such as the National Collegiate Athletic Association, National Athletic Trainers’ Association, American Academy of Orthopaedic Surgeons, American Equipment Managers Association, or NOCSAE might consider implementing standards for football equipment as it relates to face mask removal. This implementation would provide for consistency and improved efficiency in the immediate treatment provided by physicians, athletic trainers, and first responders in the management of seriously injured helmeted athletes.