
Abstract
Background: During the past decade, bioabsorbable interference screws have become increasingly popular in endoscopic reconstructions of the anterior cruciate ligament. With these screws, there is no need for a second operation for removal and no complicating factor if later revision surgery is necessary. Several pullout studies have found similar results between metal and bioabsorbable interference screws; however, few studies have investigated the clinical outcome.
Hypothesis: There is no difference in the clinical outcome of bioabsorbable interference screws compared with metal screws.
Study Design: Randomized controlled clinical trial; Level of evidence, 1.
Methods: Forty-one patients were randomized for the use of either metal interference screws (20 patients) or bioabsorbable poly-L-lactic acid screws (21 patients). The patients were followed with clinical examinations at 6, 12, and 24 weeks and at 1 and 2 years postoperatively.
Results: Subjective knee function was better in the patients in the metal screw group; they had less pain at rest, a higher Tegner score, a higher Lysholm score, and better subjective knee function at 2 years compared to the bioabsorbable screw group. However, there was no difference in stability between the groups.
Conclusion and Clinical Relevance: Because of the inferior results in the bioabsorbable screw group in our study, and until larger studies show otherwise, we do not find the advantages of using bioabsorbable screws sufficient to warrant the routine use of poly-L-lactic acid screws in anterior cruciate ligament reconstructions.
Keywords
The great majority of patients with nonoperative ACL injuries find that giving way of the knee is a problem.
10
Reconstructions of the ACL using bone–patellar tendon–bone (BPTB) grafts have been the standard, with metal screws used for graft fixation. Because these screws will remain in the femur and may cause problems if later adjustments are required, different bioabsorbable screws made from polyglycolic acid (PGA), poly-
When bioabsorbable screws are used, there is usually no need for a second operation to remove them, and later revision surgery, if necessary, is easier. Postoperative MRI evaluation is also easier without metal artifacts. However, some authors8,25 report synovial reaction to biodegradable rods and screws.
This prospective, randomized clinical trial compared the clinical outcome of the PLLA screw with that of the metal cannulated interference screw. The aim of this study was to compare the clinical outcomes using either bioabsorbable interference screws or metal screws for ACL reconstruction.
Materials and Methods
Subjects for this study were selected during the period from June 6, 2000 to November 21, 2001. Patients with isolated ACL ruptures or ACL ruptures with additional minor meniscal lesions and minor cartilage lesions (Outerbridge grades I and II) were included.
All ACLs were reconstructed with a BPTB graft procedure using the endoscopic technique. After a diagnostic arthroscopy, the patients were assigned randomly to treatment with either the BioScrew (Linvatec, Largo, Fla) or a metal interference screw (Linvatec). The patients were followed with regular clinical examinations, including the Lysholm function score, 15 Tegner activity score, 26 modified Cincinnati score, 19 Lachman test, pivot-shift test, KT-1000 arthrometer (MedMetric Corp, San Diego, Calif) examination, 5 and clinical measurements of swelling at 6, 12, and 24 weeks and at 1 year and 2 years (24–35 months) postoperatively. In addition, the patients themselves assessed their subjective knee function as excellent, good, fair, or poor at every follow-up.
Surgery was carried out at our hospital by 4 experienced ACL surgeons. The follow-ups were carried out by the first author.
Surgical Technique in ACL Reconstruction with BPTB Grafts
The reconstruction procedure was carried out under epidural or general anesthesia under tourniquet control. After a diagnostic arthroscopy with assessment and, if necessary, treatment of the menisci, a notchplasty was performed. The graft was then harvested through 2 short horizontal incisions from the middle third of the ligamentum patellae, with a bone block of 1 × 1 × 2.5 cm from the patella and from the tibial tubercle. The bone blocks were trimmed to fit snugly into a tunnel 9 mm in diameter.
A Kirschner (K)–wire was brought in from the outside to the center of the original insertion of the ACL on the tibia using a Howell tibial guide. The K-wire was overdrilled with a 10-mm cannulated reamer, and the intra-articular entrance of the tunnel was chamfered to avoid sharp bony edges. With the femur guide on the posterior side of the femur, a K-wire was drilled into the femur at the 11-o'clock position in the right knee and the 1-o'clock position in the left knee. The K-wire was overdrilled with a 9-mm cannulated bur to the desired depth (usually 25 mm). For the BioScrews only, an eccentric notching device was entered along the tunnel to create an initiation notch for the BioScrew. The entry notch was then tapped to make the insertion of the BioScrew easier. The graft was brought into place by pulling it through the tibial tunnel and into the femoral tunnel. The femoral bone block was fixed from the inside with a cannulated PLLA or metal interference screw of 7 × 25 mm. The knee was cycled several times, and the graft was pretensioned with approximately 4 kg of tension. The bone block in the tibial tunnel was fixed with an interference screw of 8 or 9 × 25 mm with the knee in extension. With the arthroscope in place, the knee was then brought through a full range of motion to assess the graft tension and to check that there was no impingement of the graft in the notch with the knee in full extension.
Rehabilitation
The rehabilitation program was the same in both groups 23 and was supervised by the same 2 physical therapists. Immediately after the operation, the patients started knee movement, and full passive extension of the knee was carried out several times a day. No brace was used. Full weightbearing was allowed as soon as tolerated. Closed kinetic chain exercises with full extension and flexion of the knee were allowed as early as possible, but extension against resistance from 0° to 30° was not allowed during the first 6 weeks. Jogging began after 10 to 12 weeks. After about 6 months, the patients were allowed to return to all sporting activities, provided the strength of the thigh muscle on the operated side was at least 85% of the strength on the contralateral side and that controlled functional training had been carried out without difficulty.
Statistics
A power of 0.9 was selected for sample size estimation. We wanted to observe a KT-1000 arthrometer maximum manual force difference of less than 2 mm. From previous studies, the standard deviation was calculated to 1.33 mm. Based on this information, we calculated that we needed 10 patients in each group to be able to observe this difference. The number of patients was doubled so we could observe differences in other variables as well. The Mann-Whitney, Pearson χ2, and independent samples t tests were used for statistical analysis. The significance level was set to P < .05.
Results
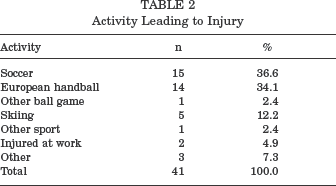
Forty-one patients (22 women and 19 men) were prospectively randomized for reconstruction with either metal interference screws (20 patients) or bioabsorbable PLLA screws (21 patients). The average age of the patients at the time of surgery was 26 years (Table 1). There were no statistically significant differences between the 2 groups in any measured parameter before surgery. The activities leading to the injuries in both groups combined are shown in Table 2.
Preoperative Comparison of the 2 Groups
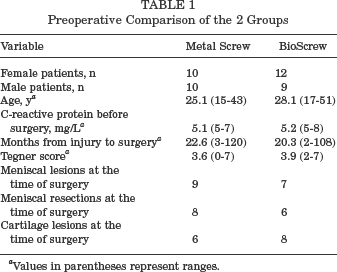
Values in parentheses represent ranges.
Activity Leading to Injury
One patient in the metal screw group suffered a rupture of the ACL in the contralateral knee 6 months postoperatively and was excluded from the study. Three patients in the BioScrew group were lost to follow-up at 2 years. One patient in the metal screw group had a purulent infection postoperatively; however, he was successfully treated with antibiotics. One patient in the BioScrew group had a resection of the medial meniscus performed 8 months after the ACL reconstruction. These last 2 patients were included in the follow-up.
Subjective Knee Function
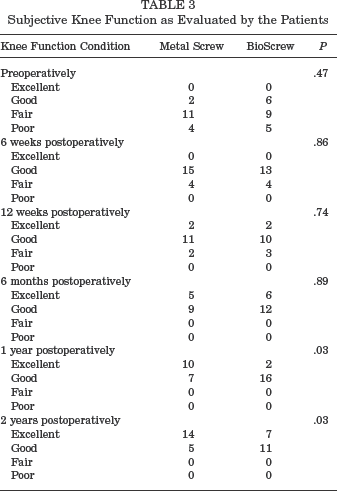
The patients’ subjective assessments of their knee function are shown in Table 3. There was no statistically significant difference between the 2 groups concerning subjective knee function up to 6 months after surgery. At the 1- and 2-year follow-ups, there was a statistically significant difference between the 2 groups in favor of the metal screw group (P < .05). At the 6-week follow-up, 4 of the patients in the BioScrew group, but none in the metal screw group, reported pain over the distal part of the medial collateral ligament (P < .05), and 4 of the patients in the BioScrew group, but none in the metal screw group, reported pain at the level of the medial joint line (P < .05).
At the 1-year follow-up, the mean pain score at rest on the modified Cincinnati score (0 = no pain to 10 = unbearable pain) was 0.27 in the metal screw group and 0.84 in the BioScrew group (P < .05). At the 2-year follow-up, the mean values were 0.04 in the metal screw group and 0.81 in the BioScrew group (P < .005).
Subjective Knee Function as Evaluated by the Patients
Activity Level
There was no statistically significant difference between the 2 groups concerning the Tegner activity score (Figure 1) at any time except for at the 2-year follow-up (P < .005). The mean Tegner activity score in both groups increased from 3.8 before surgery to 7.1 after 2 years (P < .001).
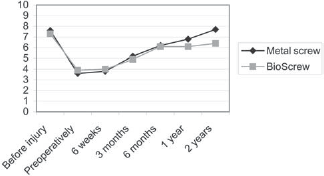
Mean Tegner activity score in the 2 groups.
Functional Level
Knee function at 2 years compared to before injury was evaluated on a scale from 0 (same function as before the injury) to 10 (very bad knee function compared to before injury). The mean values were 0.93 in the metal screw group and 2.19 in the BioScrew group (P < .05). The mean Lysholm scores (Figure 2) were 84 in the metal screw group and 78 in the BioScrew group at 6 weeks (P < .05), and 97 and 94, respectively, at 2 years (P < .05). The mean Lysholm score in both groups increased from 68 before surgery to 95 after 2 years (P < .001).
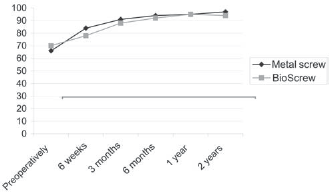
Mean Lysholm functional score in the 2 groups.
Range of Motion
Six patients in the BioScrew group had an extension deficit between 5° to 10° after 3 months, compared to only 1 patient in the metal screw group (P < .05). There was no statistically significant difference between the groups concerning range of motion at any other time.
Stability
Table 4 shows the measurements of stability in the 2 groups. The repair was considered to have failed when the results of the Lachman and pivot-shift tests were at least 2+ and the KT-1000 arthrometer demonstrated a laxity of 3 mm or greater on the tested side compared with the contralateral side.
Measurements of Stability in the 2 Groups
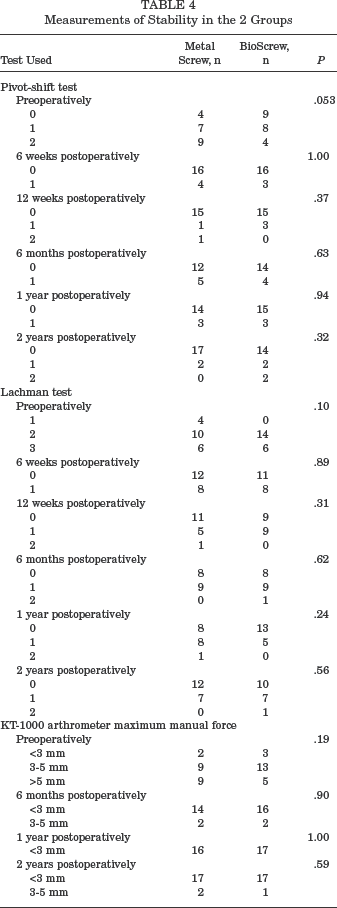
At the 2-year follow-up, there were 2 patients with a pivot-shift result of 2+ in the BioScrew group and none in the metal screw group. One patient had a Lachman test of 2+ in the BioScrew group, whereas there were none in the metal screw group. The mean KT-1000 arthrometer maximum manual force preoperatively was 4.3 mm in the BioScrew group and 5.5 mm in the metal screw group. The corresponding values after 2 years were 0.3 mm and 0.9 mm. The decrease in KT-1000 arthrometer values for both groups together was statistically significant (P < .01). The KT-1000 arthrometer measurements showed 1 patient in the BioScrew group and 2 patients in the metal screw group with a laxity of 3 mm or greater.
We found no statistically significant difference between the groups in stability measured by pivot-shift test, Lachman test, or KT-1000 arthrometer at any time.
Swelling
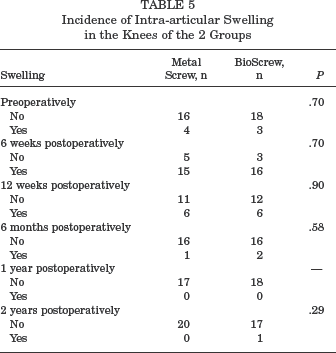
Table 5 shows the incidence of intra-articular swelling in the knees in the 2 groups. One of the patients in the BioScrew group had intra-articular swelling at the 2-year follow-up. There was no significant difference between the groups at any time.
Incidence of Intra-articular Swelling in the Knees of the 2 Groups
Discussion
The bioabsorbable screws in this study were made from PLLA and are resorbed. In one study, 16 71 sheep underwent tendon reconstruction to compare graft security using a titanium or an absorbable polyglyconate interference screw. Overall, the absorbable screws performed as well as the metal screws. Several other studies showed no statistical difference in pullout tests using bioabsorbable or metal screws.1,4,11,13,22
Polyglyconate interference screw fixation for patellar tendon grafts 9 has not been found to be associated with increased clinical complications or significant osteolysis, and it provides clinical results comparable to those obtained with titanium screws. In a study of young cadaveric knees, 21 the mean failure load for the metal screws was found to be significantly higher than that for the absorbable screws. In our study, the mechanical properties of the BioScrew seem to be sufficient. We found no statistically significant difference in stability measured by pivot-shift test, Lachman test, or KT-1000 arthrometer at any time between the groups. The failure rates of the reconstructions, measured by these tests, were between 0% and 10%. This finding is in accordance with previous studies.6,17 Several studies2,3,9,12,14,16 have shown no statistical difference between clinical results using either the bioabsorbable interference screw or the metal screw. In our study, we found that at the 1- and 2-year follow-ups, there was a statistically significant difference between the 2 groups concerning subjective knee function in favor of the metal screw group. The BioScrew patients had significantly more pain at rest, both at the 1- and 2-year examinations, and they also had a significantly lower Tegner score after 2 years. In addition, the subjective knee function assessment at 2 years, compared with before injury, and the Lysholm score at 6 weeks and 2 years were significantly lower in the BioScrew group. This result may be due to a dissolving of the screws and activation of the complement system causing an inflammatory reaction with pain (J.O. Drogset, unpublished data, 2004).
McGuire et al 17 could not find any significant differences between 32 patients with PLLA screws and metal screws in any parameter measured at 4 years. However, 12 PLLA screws broke during insertion, albeit without any adverse effects. In our study, none of the BioScrews broke during insertion.
Freehill et al, 7 in a retrospective study of 52 patients who underwent arthroscopic shoulder stabilization with an average of 2.2 PLLA tacks per patient, showed that 10 patients developed adverse effects at an average of 8 months after surgery, including pain in all 10 patients and progressive stiffness in 6. Several other studies have also shown inflammatory reactions after the use of biodegradable implants.8,24,25 In our study, the measurements of increased pain and decreased subjective knee function may be explained by an increase in inflammatory parameters in some patients in the BioScrew group (J.O. Drogset, unpublished data, 2004), although we could not detect any difference in intra-articular swelling between the groups. The differences in the parameters found in this study are numerically small but statistically significant. The clinical significance of these findings is uncertain.
Because of the inferior results in the BioScrew group in our study, and until larger studies show otherwise, we do not find the advantages of using bioabsorbable interference screws compared to metal screws sufficient to warrant the routine use of PLLA screws in ACL reconstructions.