
Abstract
Background: Injuries to the popliteomeniscal fascicles of the lateral meniscus are difficult to identify from physical examination and magnetic resonance imaging scans. To our knowledge, there have been no described physical examination techniques to identify symptomatic isolated popliteomeniscal fascicle tears. The popliteomeniscal fascicles have been demonstrated to be important for lateral meniscus stability, and it has been reported that tears can lead to painful symptoms.
Hypothesis: Popliteomeniscal fascicle tears cause symptomatic lateral compartment knee pain and can be diagnosed by physical examination. Surgical repair can improve patient function.
Study Design: Case series; Level of evidence, 4.
Methods: Six patients with isolated tears of the popliteomeniscal fascicles, which caused lateral joint line knee pain, were identified by positive figure-4 test results.
Results: All patients were found to have replication of their symptoms while placing the affected knee in the figure-4 position and were found to have lateral meniscal hypermobility due to tears of the popliteomeniscal fascicles on arthroscopic examination. All patients had an open repair of the popliteomeniscal fascicles of the lateral meniscus with complete resolution of their symptoms at a mean follow-up of 3.8 years postoperatively.
Conclusions: The figure-4 test was found to be useful in identifying the source of lateral compartment knee pain due to popliteomeniscal fascicle tears. Open repair of isolated popliteomeniscal fascicle tears was also found to be effective in resolving lateral compartment knee pain due to popliteomeniscal fascicle tears.
Symptomatic lateral compartment knee pain due to isolated injuries involving the popliteomeniscal fascicles of the lateral meniscus may be routinely missed on physical examination. 11 This situation is largely due to the lack of consistent clinical or MRI findings in an otherwise stable knee with no obvious meniscal or articular cartilage abnormality.6,8,11 It is known that a high percentage of knees with acute and chronic ACL and/or posterolateral injuries have concurrent damage to the popliteomeniscal fascicles.6,12 It has also been reported that patients with an isolated popliteomeniscal fascicle injury, also called a hypermobile lateral meniscus, have this disability because of a failure to properly diagnose and treat the injury.5,6,8,10,11 The purpose of this study was to describe the presenting history of symptomatic isolated injuries to the popliteomeniscal fascicles of the lateral meniscus and to report a clinical test to diagnose this condition. In addition, we wished to report on the surgical treatment and outcome in this case series.
Materials and Methods
Clinical Population
Between May 1997 and May 2000, 6 patients were found to have isolated unstable tears of the popliteomeniscal fascicles of the lateral meniscus, which were symptomatic, with no other source of intra-articular knee abnormality (Table 1). The first 2 patients were National Collegiate Athletic Association (NCAA) Division I varsity wrestlers who noted significant pain and an inability to compete when their affected knees were placed in the figure-4 position during an attempted takedown maneuver. The initial MRI scan on the first patient demonstrated no obvious lateral compartment disorder other than a suspicion of increased size of the popliteal hiatus at the level of the lateral meniscus. A tear of the popliteomeniscal fascicles’ attachment to the lateral meniscus was suspected and confirmed by the demonstration of meniscal subluxation into the joint during arthroscopic probing. An open repair of the popliteomeniscal fascicles’ attachment to the lateral meniscus was performed, and the patient had complete resolution of his symptoms and returned to varsity wrestling. Similar findings in the second patient resulted in our adding the figure-4 test when examining patients with lateral knee pain and no other obvious articular cartilage degeneration or lateral meniscal tears, to assess for the possibility of an unstable tear of the popliteomeniscal fascicles. All patients were referred for treatment because of vague, symptomatic lateral compartment–based knee pain during a normal MRI scan.
Data for 6 Patients With Isolated Unstable Symptomatic Popliteomeniscal Fascicle Tears to the Lateral Meniscus
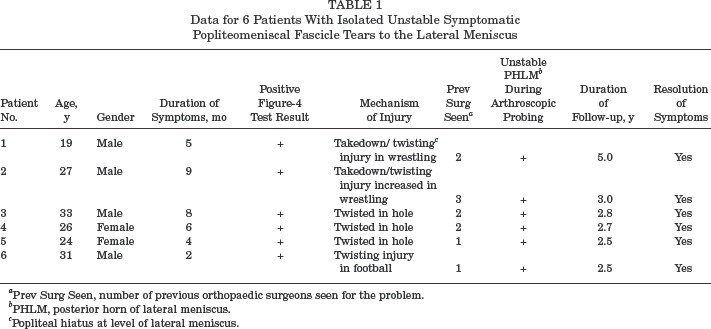
Prev Surg Seen, number of previous orthopaedic surgeons seen for the problem.
PHLM, posterior horn of lateral meniscus.
Popliteal hiatus at level of lateral meniscus.
Standard clinical testing for lateral and posterolateral knee pain and instability did not reveal any evidence of abnormality in these 6 patients. These tests included lateral-based posterior knee pain with maximal knee flexion, lateral joint line pain due to forced varus stressing at 30°, and palpation of the lateral epicondyle, fibular collateral ligament–biceps bursa, iliotibial band, and common peroneal nerve.2,3,7,8,9 All patients had previously been seen by an orthopaedic surgeon, had an apparently normal MRI scan on initial reading by a radiologist, and continued to have lateral knee joint line pain and functional limitations with activities.
The Figure-4 Test
The figure-4 test places the affected knee in flexion, varus, and external rotation. In an uninjured knee, this configuration produces tension on the posterolateral structures of the knee as the intact popliteus complex and popliteomeniscal fascicles act to prevent medial displacement of the lateral meniscus.4,10,12,14 However, if the popliteomeniscal fascicles are disrupted, the normal peripheral hoop tension on the lateral meniscus is lost, a circumstance that can result in the lateral meniscus displacing medially into the joint.10,12
To perform the figure-4 test, the patient is placed supine on the examination table. Next, the affected knee is flexed to slightly more than 90°. The foot of the affected extremity is then placed over the contralateral knee as the hip is externally rotated. Finally, a varus stress is applied to the medial side of the affected knee, creating the shape of a figure-of-4 (in the right knee) when the examiner pushes the affected knee toward the examining table (Figure 1). A positive test result occurs when pain that reproduces the patient's symptoms develops at the lateral joint line of the knee at the popliteal hiatus. It is important to contrast this result with the unaffected contralateral knee to verify the location of pain and to confirm that it reproduces the patient's symptoms.
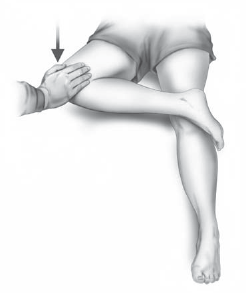
Illustration of the figure-4 test for the assessment of symptomatic disruption of the popliteomeniscal fascicles of the lateral meniscus in the right knee.
Surgical Approach
After an examination under anesthesia, a standard arthroscopic evaluation of the knee with a specific emphasis on the lateral compartment was performed. 6 In addition to an assessment of meniscal and articular cartilage lesions, the integrity of the popliteus tendon's femoral attachment, the meniscotibial and meniscofemoral portions of the midthird lateral capsular ligament, and the coronary ligament of the posterior horn of the lateral meniscus were assessed. While the knee was flexed to 20° and placed in slight valgus, the 30° arthroscopic cannula was placed in the lateral gutter at the popliteus hiatus, and the integrity of the anteroinferior, posterosuperior, and posteroinferior popliteomeniscal fascicles was assessed.12,13,15 If they were found to be torn, it was observed that when a varus stress was placed on the knee, the lateral meniscus subluxated medially into the lateral compartment when viewed from the lateral gutter. 12 The arthroscope was then placed into the lateral compartment, and a surgical probe was used to hook the bare area of the lateral meniscus at the popliteal hiatus. 12 This step was undertaken in an attempt to displace the lateral meniscus medially (Figure 2) to determine if subluxation of the body of the lateral meniscus occurred medially into the lateral compartment. If the meniscus was found to be unstable and subluxated into the joint with probing, an open repair was then performed.
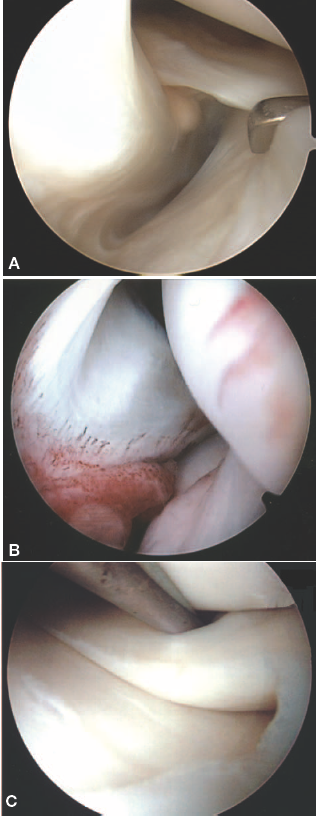
A, arthroscopic view, lateral gutter, right knee, with normal popliteomeniscal fascicles (medial traction applied). B, arthroscopic view, lateral gutter, right knee, of torn popliteomeniscal fascicles. C, arthroscopic view of disruption of the popliteomeniscal fascicles of the lateral meniscus in a left knee. Significant subluxation of the lateral meniscus can be demonstrated by medial traction applied by a surgical probe.
After it was confirmed that the popliteomeniscal fascicles were torn and the lateral meniscus was unstable, an open direct repair was then performed. An 8- to 10-cm long laterally based skin incision, centered over the midportion of the superficial layer of the iliotibial band, was made. 15 The iliotibial band was then split in line with its fibers, and the edges were retracted anteriorly and posteriorly to expose the lateral capsule and midthird lateral capsular ligament. Two vertical capsular arthrotomy incisions were then made (Figure 3). The first incision was 1 cm anterior to the fibular collateral ligament and was directly over the femoral popliteal sulcus 12 and through the meniscofemoral portion of the midthird lateral capsular ligament. 15 This incision allowed access to the anteroinferior popliteomeniscal fascicle8,12,15 and its attachment to the lateral meniscus (Figure 4). The second incision was made through the meniscofemoral portion of the posterolateral capsule between the fibular collateral ligament and lateral gastrocnemius tendon (Figure 5). Through this incision, the 2 posterior popliteomeniscal fascicles and their attachment to the lateral meniscus were approached.
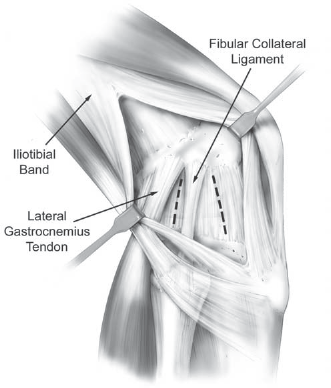
Illustration (lateral view, right knee) demonstrating the capsular incisions necessary to approach the torn popliteomeniscal fascicles. The superficial layer of the iliotibial band is retracted anteriorly and posteriorly to expose the lateral capsule. The anterior incision is through the midthird lateral capsular ligament and allows access to the popliteus tendon's femoral attachment and the anteroinferior popliteomeniscal fascicle. The posterior incision is through the posterior meniscofemoral capsule between the fibular collateral ligament and lateral gastrocnemius tendon and allows access to the posterosuperior and posteroinferior popliteomeniscal fascicles.
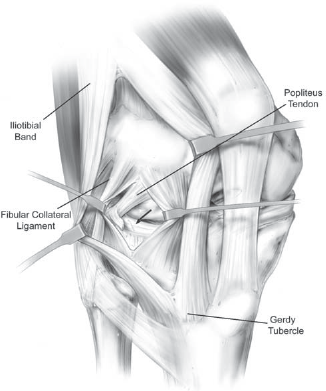
Illustration (lateral view, right knee) demonstrating the anterolateral capsular arthrotomy incision, with the midthird lateral capsular ligament retracted anteriorly and posteriorly, and demonstrating the tear of the anteroinferior popliteomeniscal fascicle (arrow) of the lateral meniscus.
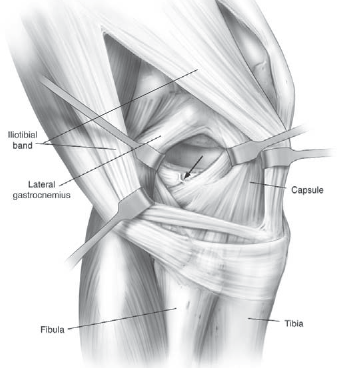
Illustration (lateral view, right knee) demonstrating the posterolateral capsular arthrotomy incision, with the meniscofemoral portion of the posterior capsule retracted between the fibular collateral ligament and lateral gastrocnemius tendon to expose a torn posterosuperior popliteomeniscal fascicle (arrow).
After open identification of the tears, horizontal mattress nonabsorbable 0 sutures were used to repair the lateral meniscus back to the popliteomeniscal fascicles and popliteus tendon complex. After verification that full range of motion could be achieved without undue tension on the surgical repair, the capsular and iliotibial band incisions were closed. The skin incision was closed with a subcuticular stitch, and an immobilizer was applied in full extension. Patients were not allowed to bear weight for 6 weeks after surgery. During this time, they were instructed to perform straight-leg raises in the immobilizer only and to work on unrestricted active and passive knee motion outside of the immobilizer 4 times daily. Patients were allowed to participate in full weightbearing and a progressive exercise regimen at 6 weeks, with a full return to activities at 4 months postoperatively if their strength and function allowed.
Results
Six patients with symptomatic isolated tears of the popliteomeniscal fascicles of the lateral meniscus were identified from May 1997 to May 2000 (Table 1). All patients were referred to the senior author (R.F.L.) for the evaluation of posterolateral knee pain, with no obvious lateral compartment abnormality identified on MRI scanning. All were noted to have lateral joint line pain that was accentuated by putting the knee in the figure-4 position (Figure 1). None of these patients had complaints of locking or catching in the lateral meniscus and they were able to fully squat with minimal lateral compartment knee pain. After arthroscopic verification that the lateral meniscus was unstable to probing, an open repair was performed.
At an average of 3.8 years postoperatively, all patients were noted to have a resolution of their symptoms. Both NCAA Division I varsity wrestlers returned to unrestricted activities and competition by the next season. At the time of the last follow-up, no patient experienced any pain while placing the affected knee in the figure-4 position (Table 1).
Discussion
There are 3 popliteomeniscal fascicles (anteroinferior, posterosuperior, and posteroinferior),12,13,15 which combined with the popliteus tendon form a peripheral hooplike attachment to the lateral meniscus at the popliteal hiatus of the knee. The popliteus complex functions, at least in part, to provide added stability via the popliteomeniscal fascicles to the otherwise nontethered section of the lateral meniscus within the popliteal hiatus. Providing both a static and dynamic connection between the lateral meniscus and the popliteus tendon, the popliteomeniscal fascicles are important in controlling the motion of the lateral meniscus during flexion and extension of the knee.1,10,12,14 Stäubli and Birrer 12 reported in their clinical observations that increased lateral meniscal motion, as well as a loss of the lateral retraction of the lateral meniscus with a varus stress applied to the knee, occurred when these fascicles were torn. Biomechanical studies by Simonian et al 10 verified these clinical observations, demonstrating that lateral meniscal motion almost doubles when both the posterosuperior and anteroinferior popliteomeniscal fascicles are disrupted compared to a meniscus with intact popliteomeniscal fascicles. 10 Moreover, these authors and others suggested that with the variable loads involved in normal activity, one would expect mechanical symptoms such as locking and giving-way episodes, as well as lateral compartment knee pain,11,12 because the lateral meniscus could potentially become trapped in the joint, contributing to pain and functional limitations in patients when the popliteomeniscal fascicles were torn. Our clinical study verified that these patients do have vague lateral compartment knee pain with activities. To prevent mechanical symptoms and posterolateral knee pain in patients, we agree with Simonian et al 10 that isolated, unstable popliteomeniscal fascicle injuries should be surgically repaired.
It was fortuitous that our first 2 patients were NCAA Division I intercollegiate wrestlers who noted significant lateral-sided pain when their knees were placed into varus and flexion with hip external rotation (the figure-4 position) during an attempted takedown maneuver. This observation was then applied to other patients who were evaluated with undiagnosed lateral knee pain. The figure-4 test result, as described here, was noted to be positive (it reproduced the patient's symptoms) in the affected knee and negative in the normal contralateral knee, in all patients during the physical examination. Positioning of the knee during the figure-4 test places increased stress on the popliteus complex and its attachment to the peripheral aspect of the lateral meniscus at the popliteal hiatus.10,11,12 Further stressing of these popliteomeniscal attachments occurs with the clinician pushing the knee into further varus. The cause of the patient's pain appears to be the entrapment of the lateral meniscus due to the medial translation seen with popliteomeniscal fascicle tears11,12 when the knee is placed in this figure-4 position. After surgical repair, no patients were noted to have lateral compartment pain postoperatively during figure-4 testing in the affected knee.
We noted that in our study, the initial MRI scan results of the lateral compartment were felt to be normal. Simonian et al 11 also reported that popliteomeniscal fascicle tears were difficult to diagnose from MRI scans. In their study, in 3 patients who were found to have unstable popliteomeniscal fascicle tears at the time of surgery, all were felt to have normal knee MRI scan results initially. The authors were able to demonstrate the normal MRI appearance in a cadaveric specimen and to correlate it to the cryosection anatomy in the study by Stäubli and Rauschning. 13 Only after a careful review, similar to that conducted by Simonian et al, 11 were we able to identify popliteomeniscal fascicle tears on the MRI scans of the patients in our study.
Tears of the popliteomeniscal fascicles are well visualized on knee arthroscopy.6,8,12 With the knee in neutral rotation and flexed to 20°, a standard 30° arthroscope allows for excellent visualization of the hooplike attachment of the popliteomeniscal fascicles to the lateral meniscus. 6 However, it is also important to verify concurrent lateral meniscal hypermobility via arthroscopic probing to confirm the need for surgical repair of popliteomeniscal fascicle tears because we postulate that some tears may not be clinically significant if they do not result in increased meniscal motion. Although our study assessed the results of open repair, we postulate that an arthroscopic or arthroscopically assisted lateral meniscal repair that restores the integrity of the popliteomeniscal fascicles and capsular attachment to the lateral meniscus would also be successful.
In conclusion, the figure-4 test of the knee was found to be clinically useful to diagnose unstable popliteomeniscal fascicle tears that cause symptomatic lateral compartment knee pain. Although we have not observed this test to produce positive results in patients with other lateral compartment knee abnormality injuries, it is important to verify arthroscopically, by direct observation and probing, that these structures are torn and the lateral meniscus is unstable before performing open surgical repair. A formal study of a larger group of patients with a variety of diagnoses would be necessary to document the overall accuracy of this test. Open surgical repair of an unstable lateral meniscus due to popliteomeniscal fascicle tears was found to improve patient function and resolve lateral compartment knee pain.