
Abstract

The tibia is the most common site of stress fractures in athletes. 9 Anterior cortex midshaft tibial stress fractures are often associated with significant morbidity, including delayed union, nonunion, and complete fracture.1,2,7,11 Stress fractures of the posteromedial tibial shaft and proximal tibial metaphysis are common and have been reported to heal readily with rest.3,4,6,7 Although there are reports of isolated stress fractures of the medial or lateral tibial plateau,5,10 there is little mention in the literature regarding stress fractures of the anterior proximal tibial metaphysis.1,8 We report on a basketball player with a recurrent, complete stress fracture of the proximal tibial metaphysis.
Case Report
A 21-year-old Division I college basketball player with a history of bilateral knee pain was evaluted with increasing pain in the tibial tubercle region. His medical history was significant for a right ankle fracture in grade 9 that was treated nonoperatively. He began developing symptoms consistent with bilateral patellar tendinitis in grade 11 and had increasing right ankle pain consistent with ankle impingement in grade 12. Before his entrance to college, he underwent ankle surgery to remove “bone spurs.” In college, he was evaluted with a varus hindfoot and continued limitations in dorsiflexion and subtalar motion. Passive range of motion of his right ankle was 0° of dorsiflexion, 30° of plantar flexion with the knee extended, and no change in passive dorsiflexion with knee flexion. He complained of pain in both knees, and there was tenderness to palpation over his tibial tubercles, which was greater for the left knee. Because of his increasing left knee pain, an MRI scan was obtained that confirmed patellar tendinitis. No MRI was obtained on the right knee. The athlete continued to engage in practices and games with no complaints to the athletic trainer or team physician of pain in either knee.
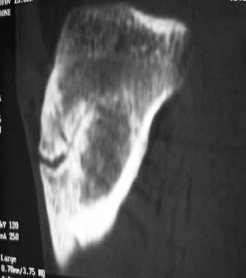
While leaping for a rebound during a game, the athlete experienced acute pain on takeoff, suffering knee/leg collapse on landing. Subsequent examination and plain radiographs revealed a proximal tibial fracture with some sclerosis at the proximal tibial cortex (Figure 1). This finding was thought to be suspicious for a previous stress reaction, and a CT scan was ordered that revealed sclerosis at the fracture site (Figure 2). These findings were consistent with acute completion of a proximal tibial stress fracture at the level of the tibial tubercle. Although the growth plates were closed, the pattern of injury seemed to follow the anatomy of the proximal tibial physis/apophysis.

Plain radiograph revealing a proximal tibial fracture with some sclerosis about the fracture.

A CT scan after initial injury revealing sclerosis about the fracture, which was consistent with a stress fracture.
The patient underwent open reduction and internal fixation with 3 screws (Figure 3). This type of fixation was chosen by the operating surgeon, a board-certified traumatologist, for 2 reasons. First, it provided adequate reduction of the fracture with no motion at the fracture site with intraoperative radiographic stressing. Second, there was a concern that more rigid forms of fixation (plate and screws) might be associated with a higher incidence of tibial pain when the athlete returned to jumping or high-impact sports.

Initial postoperative radiograph revealing reduction and fixation of the fracture with 3 screws.
Four months postoperatively, the patient returned to some conditioning activities with no discomfort but did not resume jumping or running. Routine radiographs and a CT scan revealed a persistent anterior cortical lucency (Figure 4). At this time, it was midsummer, 4 months before the start of formal basketball practice, and an autologous iliac crest bone grafting procedure was performed to maximize the potential for healing over the next 2 to 3 months (Figure 5). Two to 3 months after the bone grafting, the patient was pain free, with decreased but persistent lucency noted only anteriorly, and was allowed to progress to full sporting activity as tolerated (Figure 6).
A CT scan 4 months postoperatively revealing persistent lucency. The screws were still in place but not visible on this particular image.

Intraoperative plain radiograph showing localization of the fracture with a needle. Autogenous bone grafting and removal of a prominent screw were performed at this time.

Plain radiograph 3 months after the bone grafting procedure revealing consolidation of the posterior portion of the original fracture and persistent anterior lucency.
The athlete returned to full workouts commensurate with the formal start of the season (mid-October). He competed fully in all practices and games without any complaints of pain, discomfort, or disability. In February, after nearly 5 months of full competition, the patient sustained a refracture through the proximal tibial tubercle region during a noncontact, power-takeoff maneuver (Figure 7). He then underwent a repeat open reduction and internal fixation with a plate and lag screw technique. This procedure led to complete union, as shown on radiographs, and the patient was able to return to basketball activities 5 to 6 months postoperatively. There were no further sequelae at the most recent follow-up of 3 years postoperatively (Figure 8).

Plain radiograph revealing a refracture of the proximal tibia.

Anteroposterior (A) and lateral (B) radiographs revealing complete healing of the fracture 3 years after rigid open reduction and internal fixation with a plate and lag screw technique.
Discussion
The tibia is reported to be the most common location for stress fractures in athletes. 9 Proximal metaphysial tibial stress fractures are typically posteromedial (compression side) in location and heal readily with activity modification and rest.3,4,6,7
Stress fractures of the anterior cortex in the mid-diaphysis are much less common than those of the proximal posteromedial tibia.2,6,7,11 There have been several reports of delayed union, nonunion, and complete fracture as a result of these anterior tibial stress fractures.1,2,7,11 Rettig et al 11 evaluated 8 patients with middle-third anterior cortex tibial stress fractures, and all patients participated in basketball activity. The middle third of the tibia is under tension rather than compression as a result of forces caused by the large posterior muscle groups, and this tension is thought to lead to prolonged healing times.2,6,7,11 Anterior cortex stress fractures often require surgical intervention such as excision and bone grafting or intramedullary nailing to achieve union.2,7
Although there have been several reports of isolated medial and lateral tibial plateau stress fractures,5,10 there is little in the literature with regard to anterior proximal metaphysial tibial stress fractures. There are 2 reports of basketball players with anterior proximal tibial stress fractures just distal to the tibial tuberosity.1,8 One of these fractures resulted in a complete fracture that healed with immobilization, 8 and the other healed after open reduction and internal fixation with a plate and screws. 1 Although these fractures were more distal than was the level of fracture in the current case, they suggest a relationship between repetitive jumping activity and anterior cortex tibial stress fractures.
The persistent restrictions for dorsiflexion and subtalar range of motion, combined with repetitive jumping, may have predisposed the patient to this injury. It is also interesting to note the pattern of injury that seemed to follow the anatomy of the proximal tibial physis/apophysis. It may be that the increased stresses across the physis resulted in incomplete closure and stress reaction through the growth center. This reaction may have then led to complete fracture. Although we have no radiographs before injury of the right knee to verify incomplete closure of the physis/apophysis or chronic stress injury, the timing of the ankle injury and development of knee pain would coincide with the time of growth plate closure.
In retrospect, the technique of initial fixation and persistent anterior tibial lucency may have contributed to the recurrent fracture. Initial internal fixation of maximal rigidity and complete healing, as shown on radiographs, may be critical to prevent the development of a nonunion or recurrent injury with this unusual fracture pattern.
Proximal metaphysial tibial stress fractures can be difficult to diagnose because of their proximity to the knee joint and its surrounding structures. The diagnosis in the current case was initially delayed because of the fracture's location at the tibial tuberosity, with a long history of bilateral patellar tendinitis. We are not aware of any other reports of a complete tibial stress fracture at the level of the tibial tuberosity.
Conclusion
The current case shows the difficulties in managing this fracture and that a high index of suspicion may be important in making an early diagnosis. Chronic restriction of ipsilateral ankle dorsiflexion and subtalar range of motion in this case may have been a contributing factor. Only after rigid internal fixation was achieved did the fracture heal. We believe that it is essential to obtain complete healing of this fracture before a return to competitive jumping activities. Rigid internal fixation of maximum rigidity appears to be optimal to achieve union with this particular fracture.