
Abstract
Background: To date, the morphological, biochemical, and biomechanical characteristics of articular cartilage in osteochondral allografts that have been stored have not been fully described.
Hypothesis: Osteochondral allografts procured and stored commercially for a standard period as determined by tissue banking protocol will have compromised chondrocyte viability but preserved extracellular matrix quality.
Study Design: Controlled laboratory study.
Methods: Unused cartilage from 16 consecutive osteochondral allografts was sampled during surgery after tissue bank processing and storage. Ten grafts were examined for cell viability and viable cell density using confocal microscopy, proteoglycan synthesis via 35SO4 uptake, and glycosaminoglycan content and compared with fresh cadaveric articular cartilage. Biomechanical assessment was performed on the 6 remaining grafts by measuring the indentation stiffness of the cartilage.
Results: The mean storage time for the transplanted specimens was 20.3 ± 2.9 days. Chondrocyte viability, viable cell density, and 35SO4 uptake were significantly lower in allografts at implantation when compared to fresh, unstored controls, whereas matrix characteristics, specifically glycosaminoglycan content and biomechanical measures, were unchanged. In addition, chondrocyte viability in the stored allografts was preferentially decreased in the superficial zone of cartilage.
Conclusion: Human osteochondral allografts stored for a standard period (approximately 3 weeks) before implantation undergo decreases in cell viability, especially in the critically important superficial zone, as well as in cell density and metabolic activity, whereas matrix and biomechanical characteristics appear conserved. The exact clinical significance of these findings, however, is unknown, as there are no prospective studies examining clinical outcomes using grafts stored for extended periods.
Clinical Relevance: Surgeons who perform this procedure should understand the cartilage characteristics of the graft after 21 days of commercial storage in serum-free media.
Articular cartilage lesions of the knee, including chondral and osteochondral defects, are a frequent and challenging cause of morbidity in the orthopaedic patient. The exact prevalence of these lesions is unknown, but a large study by Curl et al 9 showed that 63% of 31 516 patients undergoing knee arthroscopies had chondral lesions. Several treatment options have been used to repair articular cartilage lesions, including subchondral drilling, microfracture, autologous chondrocyte implantation, mosaicplasty, allograft transplantation, and prosthetic arthroplasty.6,19 Recently, there has been a growing interest among orthopaedic surgeons in the use of fresh-refrigerated human osteochondral allografts that have been stored at 4°C for the treatment of large chondral lesions, osteochondritis dissecans, osteonecrosis, and posttraumatic reconstruction of the knee.2,7,13,14,23
The first reported clinical use of osteochondral allografts was by Erich Lexer 15 in the early 1900s. The initial success of these surgeries was limited by several factors such as revascularization failure, immune reaction to donor tissue, and technical difficulties. The practice was subsequently abandoned for the next 50 years. In the 1970s, renewed interest in allograft transplantation occurred after musculoskeletal tumor surgeons had success with frozen grafts.17,25 The freezing process has been shown to minimize graft immunogenicity and to prolong storage times, but at the cost of chondrocyte viability. In more recent years, these strategies have been employed by surgeons to replace focal articular cartilage lesions. Fresh-refrigerated osteochondral allografts are ideal for these lesions because they contain architecturally mature hyaline cartilage with living chondrocytes on an osseous scaffold that provides support for the articular cartilage. The long-term clinical outcome of osteochondral allografts has been good, with successful outcomes in 60% to 80% of cases at 10 years.8,10,18
Recent safety concerns have necessitated strict guidelines regarding microbiologic and serologic testing before implantation, resulting in a minimum 7- to 14-day period for completion, compared to the traditional practice of implanting allografts within 1 week of harvest. Although previous in vitro studies have demonstrated a decrease in chondrocyte metabolic activity and viability after 14 days of storage, the cartilage quality of osteochondral allografts at the time of surgical implantation has not been thoroughly studied. Therefore, the purpose of this study was to characterize commercially available allografts at the time of surgery by assessing the biochemical and biomechanical characteristics of cartilage when compared to freshly procured allograft tissue.
Experimental Method
Graft Preparation and Storage Conditions
Sixteen consecutive specimens were collected from the distal femur or tibial plateau at the time of osteochondral allograft surgery. Ten grafts were used for testing chondrocyte viability, viable cell density, proteoglycan synthesis, and glycosaminoglycan content, whereas 6 grafts were used for the biomechanical analysis. All grafts were prepared and stored at an outside tissue bank that supplies osteochondral allografts to the University of California, San Diego, according to the guidelines set forth by the American Association of Tissue Banks (Allosource, Centennial, Colo). The tissue was initially retrieved within 24 hours of donor death. Donors were screened using a medical-social history for malignancy, autoimmune disease, and high-risk behavior. At the time of retrieval, the knee joint was recovered en bloc and transferred sterilely to the tissue bank, where they were stored between 1°C and 10°C. The final processing was then performed at the tissue bank within 72 hours of donor death. Before storage, the specimens were cleansed aseptically with saline pulse lavage to remove blood and fat from the cancellous bone. The specimens were stored in serum-free media supplemented with antibiotics and maintained at a temperature between 2°C and 8°C. Every 7 days, the storage media was changed under sterile conditions. Blood and tissue cultures were obtained at the time of final processing, including screening for human immunodeficiency virus 1 and 2, hepatitis B and C, cytomegalovirus, human T-lymphotropic virus I and II, and syphilis. Microbial cultures using a 14-day resistant organism culture technique were performed, and tissue was not released until all results were negative. The tissue bank's shelf life for all osteochondral allografts was 4 weeks from the date of donor death. Inclusion criteria in this study matched current allograft guidelines, that is, age of 15 to 45 years, Noyes and Stabler 22 grade IA cartilage, and negative serologies and cultures. Ten control specimens that were of identical quality and processed in the same fashion as the experimental tissue were used in this study. The tissue was shipped to our laboratory directly from the tissue bank after the final processing was complete, which averaged 3 days.
Chondrocyte Viability and Viable Cell Density
Full-thickness cartilage was removed from subchondral bone and sectioned into approximately 1-mm-thick coronal slices. These slices were then placed into a solution containing 2′,7′-Bis(2-carboxyethyl)-5(6)-carboxyfluorescein, acetoxymethyl ester (BCECF-AM, Calbiochem, San Diego, Calif), which stains viable cells green, and propidium iodide (Calbiochem), which stains nonviable cells red. The BCECF-AM is a fluorescein derivative that is metabolized by nonspecific esterases in living cell membranes to a green fluorescent product. Propidium iodide is normally excluded from living cells by the intact cell membrane, but it penetrates nonviable cells and intercalates with the DNA and fluoresces red. The specimens were placed in a 5% CO2/95% O2 incubator at 37°C for 30 minutes and then viewed with a laser confocal scanning microscope equipped with a krypton and argon laser (Zeiss LSM 510, Carl Zeiss, Thornwood, NY). Three coronal slices were imaged at 3 random locations within each of the superficial, middle, and deep cartilage regions, for a total of 9 images per plug, which were then averaged to produce a single data point. Images were obtained at multiple random locations within the cartilage slice with use of laser scanning systems software (Zeiss LSM 510). Viable and nonviable cells were then tabulated with use of computer software (Image-Pro Plus 4.1, Media Cybernetics, Silver Springs, Md). The confocal laser microscope was programmed to obtain an image at multiple, defined focal depths. These images were then reconstructed with use of an image processing and analysis program (NIH Image 1.6, National Institutes of Health, Bethesda, Md). This produced a 3-dimensional image cube with an optical section dimension of 0.7 × 0.7 mm and a reconstructed focal depth of 0.025 mm (volume = 0.7 × 0.7 × 0.025 mm = 0.01225 mm3). The viable cell density (viable cells per unit volume) was determined by calculating the number of viable cells within this known volume, and the results were expressed as cells per cubic millimeter. 20
Proteoglycan Synthesis
Full-thickness cartilage was removed from subchondral bone and sectioned into approximately 0.2 × 0.2-mm pieces. These specimens were immediately placed in 10 mL of medium containing 5 μCi/mL of 35SO4 (Perkin Elmer Life Sciences, Boston, Mass) and incubated at 37°C in 5% CO2/95% O2 for 48 hours. Specimens were then dialyzed in deionized water to remove unincorporated 35SO4 and lyophilized. The tissue was then weighed and hydrolyzed. The hydrolysate was analyzed in a liquid scintillation spectrometer for quantification of 35SO4 incorporation. 1
Glycosaminoglycan Content
Full-thickness cartilage was removed from subchondral bone and sectioned into approximately 0.2 × 0.2-mm pieces. The specimens were then washed in deionized water and hydrolyzed, and the amount of glycosaminoglycan was determined and reported as the percentage of hexosamine per unit of dry tissue. 1
Biomechanical Analysis/Indentation Stiffness
An arthroscopic probe (ACTAEON, OsteoBiologics, San Antonio, Tex) was used to determine the indentation stiffness of the intact articular cartilage of each specimen. Each osteochondral plug was clamped at the bone to stabilize the sample. The probe was held in a standardized fashion, and 15 stiffness measurements at 5 different sites per sample were performed and averaged. At each test site location, the probe was triggered consecutively 3 times and provided a stiffness measurement on a scale of 0 to 99. The probe was calibrated to the American Society for Testing and Materials Type-A Durometer Standards (ASTM International, West Conshohocken, Pa). On this scale, a relatively low value indicates a relatively soft sample.3,4,21
Statistical Analysis
For statistical analysis, t tests were used to compare control and experimental values, and analysis of variance was used to compare cell viability of cartilage zones. Significance was set at P =. 05 for all tests.
Results
Demographic Data and Gross Grading of Cartilage
All cartilage from both the stored and control samples was Noyes and Stabler 22 grade IA. The mean storage time for the stored specimens was 20.3 ± 2.9 days, and the mean donor age was 29 ± 9 years (range, 16–40 years). The mean age of the donors for the fresh (not stored) specimens was 29 ± 7 years (range, 16–34 years). All osteochondral grafts were from male donors.
Chondrocyte Viability and Viable Cell Density
Chondrocyte viability measured by confocal microscopy was significantly (P <. 05) lower in the commercially stored group (82% ± 5%) versus the control group (99% ± 1%) (Figure 1). Preferential cell loss was also observed in the superficial zone relative to the middle and deep zones after storage (P <. 05) (Figures 2 and 3). The mean chondrocyte viability in the superficial zone was 75% ± 8% compared to the middle and deep zones, which were 84% ± 3% and 87% ± 5%, respectively. Interspecimen variability in chondrocyte viability in the superficial zone was significant, ranging from 62% to 92% in the 10 specimens analyzed. Viable cell density was 13 600 ± 2600 cells/mm3 in allografts at implantation and was significantly lower than that of controls (16 200 ± 2000 cells/mm3) (Figure 4).
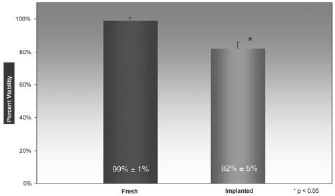
Chondrocyte viability expressed as a percentage. The results are shown as mean values with SD error bars. There was a significant decline in chondrocyte viability in stored allograft at the time of surgical implantation compared to fresh allograft (P <. 05).
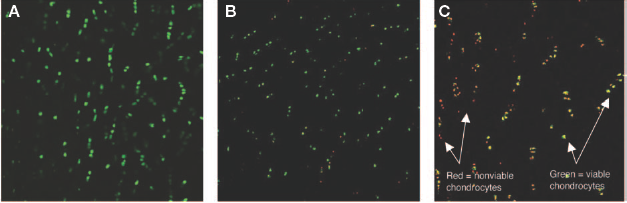
Confocal microscope images of the superficial layer of cartilage from fresh osteochondral allograft (A) versus implanted allograft after 21 days of storage (B, C). The scale of the image from border to border is 600 mm. The green-stained cells signify viable chondrocytes, whereas the red-stained cells signify nonviable cells. After 21 days of storage, the number of nonviable cells had increased significantly, and the viable cell density had decreased. In addition, the variability in chondrocyte viability in the superficial layer between specimens had increased significantly, as depicted in B and C, whereas the percentage of viable cells ranged from 62% to 92% and averaged 75% ± 8% as illustrated in Figure 3.
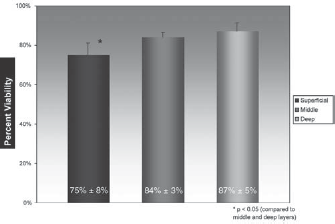
Chondrocyte viability by layer of surgically implanted allograft expressed as a percentage. The results are shown as mean values with SD error bars. There was preferential death of chondrocytes in the superficial zone relative to the middle and deep zones at the time of surgical implantation (P <. 05).
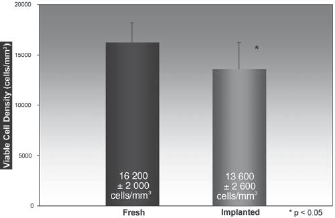
Viable cell density in cells per cubic millimeter. The results are shown as mean values with SD error bars. There was a significant decline in viable cell density in the stored allograft at the time of surgical implantation compared to the fresh allograft (P <. 05).
Proteoglycan Synthesis
The 35SO4 uptake, which measures proteoglycan synthesis and indicates metabolic activity, was significantly reduced after storage, with a mean value of 252 ± 75 cpm/mg dry cartilage, when compared to a mean control value of 395 ± 170 cpm/mg (P <. 05) (Figure 5).
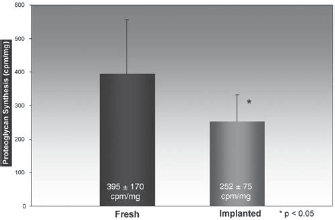
Proteoglycan synthesis measured by 35SO4 uptake in counts per minute (CPM) per milligram dry weight of cartilage. The results are shown as mean values with SD error bars. There was a significant decline in 35SO4 incorporation at the time of surgical implantation compared to the control (P <. 05).
Glycosaminoglycan Content
The glycosaminoglycan content was 3.9% ± 0.7% in the stored allograft group, which did not significantly differ from the control group value of 4.1% ± 0.8% (Figure 6).
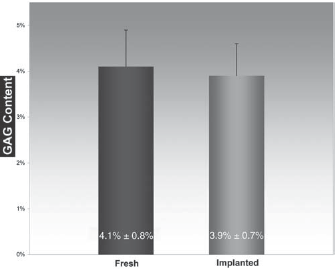
Glycosaminoglycan (GAG) content as a percentage of hexosamine per unit dry weight of cartilage. The results are shown as mean values with SD error bars. At the time of surgical implantation, the GAG content had remained stable in the stored allograft relative to the fresh allograft.
Biomechanics
Indentation stiffness was not significantly different between stored allografts and controls. The mean indentation stiffness for the implantation group was 59 ± 5 and 57 ± 10 for the control group (Table 1).
Chondrocyte Viability, Viable Cell Density, Metabolic Activity, and Articular Cartilage Indentation Stiffness and GAG Content in Transplanted Osteochondral Allografts a
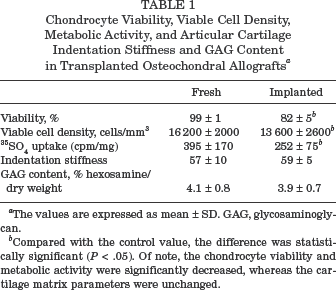
The values are expressed as mean ± SD. GAG, glycosaminoglycan.
Compared with the control value, the difference was statistically significant (P <. 05). Of note, the chondrocyte viability and metabolic activity were significantly decreased, whereas the cartilage matrix parameters were unchanged.
Discussion
Fresh osteochondral allografts have been used effectively for the treatment of osteochondral defects of the femoral condyle and the tibial plateau with a high rate of long-term clinical success. Traditionally, osteochondral allograft tissue has been transplanted within 1 week and often within 72 hours of procurement. Because of safety concerns due to bacterial contamination and the potential for disease transmission, commercial tissue bank protocols have extended the time between graft recovery and its release for clinical use. Currently, most allograft tissue in the United States is transplanted after 2 to 4 weeks of tissue bank storage, but this period may be as long as 40 days. The clinical impact of this newly increased storage period is unclear and has led to questions related to the effects of storage on graft viability and the quality of implanted tissue.
The effects of prolonged storage on osteochondral allografts have been examined previously, and although the physical integrity of articular cartilage is maintained over time, chondrocyte viability and metabolic activity decrease after 14 days.5,26 The application of these studies has been limited because of the unknown clinical relevance of these findings. Moreover, laboratory storage conditions likely vary from conditions in outside tissue banks. Therefore, we believe it is important to evaluate osteochondral allograft tissue that has been stored commercially at the time of implantation to better determine cartilage characteristics such as chondrocyte viability, metabolic activity, and matrix quality.
In this investigation, stored allograft was evaluated, on average, after 3 weeks of storage (20.3 ± 2.9 days). At this time, approximately 80% of chondrocytes were viable; however, this finding represented a statistically significant decline in chondrocyte viability, viable cell density, and proteoglycan synthesis when compared to tissue evaluated immediately after harvest. The graft matrix was preserved during the storage period, as measured by glycosaminoglycan content and indentation stiffness. These findings parallel those of Williams et al, 26 who showed that a significant decline in chondrocyte viability, viable cell density, and proteoglycan synthesis occurred between 2 and 4 weeks of storage in a laboratory environment. Although the loss of chondrocyte viability and metabolic activity at the time of surgical implantation was statistically significant, it is unclear whether these changes were clinically significant. An in vivo study is needed to evaluate the clinical relevance of these findings.
Recently, a study was published by Pearsall et al 23 examining chondrocyte viability and ultrastructure in osteochondral allografts at the time of surgical implantation. In their study, allografts were implanted and analyzed after 30 days of storage. The chondrocyte viability measured using flow cytometry was 67% ± 13%, a value similar to that seen in our study. Two limitations of their study were that they did not evaluate the metabolic activity of the chondrocytes or the mechanical properties of the articular cartilage, both of which were assessed in our study. Another major difference between the studies was that their grafts were stored in fetal bovine serum, a media that has potential clinical risks including infectious disease transmission, namely bovine spongiform encephalopathy, and immunologic considerations. The grafts in our study, on the other hand, were stored in a defined serum-free media circumventing these potential clinical concerns while still preserving chondrocyte viability and the graft's extracellular matrix.
Based on allograft retrieval studies, successful long-term survival of the articular cartilage likely requires viable chondrocytes present in the graft to sustain the extracellular matrix.11,12 For this reason, steps have been taken to optimize allograft chondrocyte viability by manipulating the storage environment. Previous studies have shown that freezing limits chondrocyte viability, such that fresh allografts are now stored at 4°C.16,17 In addition, Ball et al 5 showed that improving storage media from lactated Ringer's solution to a serum-free culture media increased cell viability and metabolic activity. Therefore, measures that improve allograft storage conditions can improve graft viability and may have a beneficial clinical effect.
Regional variation in chondrocyte viability was shown to exist in our study, such that preferential chondrocyte death occurred in the superficial zone when compared to the middle and deep zones. A similar trend was seen by Ball et al, 5 who observed decreased superficial viability in allografts as early as 7 days into the storage period. These findings suggest that an early insult, perhaps at the time of recovery, may be responsible for this regional variation. Alternatively, this metabolically active zone may be more sensitive to external stimuli such as air exposure, which has been previously observed by Speer et al. 24 Given the importance of the superficial zone in resisting shear stress and minimizing joint friction through the expression of lubricin, the effects of superficial chondrocyte loss in this region cannot be underestimated. Of note, there was significant variability between specimens with respect to chondrocyte viability, particularly in the superficial zone. The source of this variation is unclear at this time, but possible explanations include donor factors such as age, gender, or activity; the intrinsic susceptibility of cartilage to retrieval techniques and storage conditions; or other unknown factors.
In summary, the findings of this investigation comparing osteochondral allograft articular cartilage at the time of surgical implantation with fresh controls show maintenance of matrix and biomechanical characteristics but a decrease in chondrocyte metabolic activity and viability. These findings are similar to those observed by previous authors examining allografts stored in a laboratory environment. In addition, our study showed preferential cell loss in the critically important superficial zone. Although at this time the clinical ramifications of these findings are unknown, in vivo studies examining the relationship between chondrocyte viability and clinical outcome are warranted.