
Abstract
Background
In double-bundle anterior cruciate ligament reconstruction, overloading either 1 of the 2 grafts should be avoided to decrease the risk of graft failure.
Hypothesis
Overloading of the posterolateral graft may occur when it is fixed at 30 ° of knee flexion because the posterolateral bundle is elongated as the knee approaches extension.
Study Design
Controlled laboratory study.
Methods
Ten human cadaveric knees were tested at (1) intact, (2) anterior cruciate ligament–deficient, (3) double-bundle anterior cruciate ligament reconstruction with the anteromedial and posterolateral grafts fixed at 60 ° of flexion and full extension, respectively (fixation 60/FE), and (4) double-bundle anterior cruciate ligament reconstruction with both grafts fixed at 30 ° of flexion simultaneously (fixation 30/30). Two external loading conditions simulating clinical examinations were used: (1) 134-N anterior tibial load and (2) combined rotatory loads of 10 N·m valgus and 5 N·m internal tibial torques. Data on knee kinematics and in situ forces in the 2 bundles of the intact anterior cruciate ligament and the respective grafts were obtained.
Results
In response to 134-N anterior tibial load, knee kinematics and in situ force in the grafts were similar to the intact knee for both fixation protocols. The force in the anteromedial graft for fixation 60/FE was 34% higher, whereas the posterolateral graft for fixation 30/30 was 46% higher, compared with the intact anteromedial and posterolateral bundles, respectively. In response to combined rotatory loads, the posterolateral graft for fixation 30/30 carried 67% higher load than did the intact posterolateral bundle.
Conclusion
Fixation 30/30 overloaded the posterolateral graft, whereas fixation 60/FE overloaded the anteromedial graft.
Clinical Relevance
In double-bundle anterior cruciate ligament reconstruction, even though overall forces in the graft are the same as intact anterior cruciate ligament, the force distributions may not be the same as the intact bundles, and overloading of 1 of the 2 grafts may occur.
Keywords
Although ACL reconstruction procedures have been commonly performed to restore knee stability, 15% to 25% of patients still experience less than satisfactory postsurgical results as reported by both short-term and long-term clinical studies.2,4,5,22,30 One possible cause could be that current single-bundle procedures cannot realistically reproduce the complex anatomy of the ACL, especially the different functions of its anteromedial (AM) and posterolateral (PL) bundles at different angles of knee flexion.13,18,32,37 Laboratory studies have clearly shown that even under the simplest external loading conditions, the force distribution between the 2 bundles can vary greatly. The PL bundle is the primary carrier of the load when the knee is near extension, whereas the AM bundle carries the majority of the load at higher flexion angles.12,29
Previous studies from our research center have further demonstrated that an anatomical double-bundle ACL reconstruction (DB-ACLR), using 2 femoral tunnels placed at the anatomical insertions of the 2 bundles of the ACL, has biomechanical advantages over single-bundle procedures creating a single femoral tunnel at either the AM or PL femoral insertion.40,41 The knee kinematics and graft function for DB-ACLR are closer to those for the normal ACL. Concomitantly, there has been a significant increase in interest of DB-ACLR in Europe, Japan, and, more recently, the United States. Even though the surgical technique varies greatly, especially for graft fixation protocols, these surgeons believe that the knee with DB-ACLR has better rotatory stability.1,7,14,25,26,33,42
As the DB-ACLR procedure involves the use of 2 separate grafts, it raises the following question: What would be a suitable range of angles of knee flexion for graft fixation to avoid overloading either 1 of the 2 grafts? Clearly, an elevated or imbalanced force distribution between the AM and PL grafts could predispose 1 or both of the grafts to a higher risk of failure. The PL graft especially may have a higher risk of graft failure because it is smaller in diameter as well as shorter in length than the AM graft.7,33,42 Thus, a small error in length would result in higher changes in the percentage of elongation in response to external loads.
Although some authors have advocated fixation of the 2 grafts at one angle of knee flexion, ranging between 10° and 90°,1,14,26,42,43 other authors have recommended graft fixation at different knee flexion angles for each graft that correspond to those used in laboratory studies.7,40,41 Thus, the objective of this study was to measure the in situ forces and force distribution of the AM and PL grafts for 2 different fixation protocols in DB-ACLR and compare them with those of the AM and PL bundles of the intact ACL. This information will help the surgeon choose suitable angles of knee flexion for graft fixation so that overloading of the graft will not take place. The hypothesis under study is that overloading of the PL graft may occur when it is fixed at a knee flexion angle of 30° because the PL bundle is elongated as the knee approaches extension.3,6
Human cadaveric knees were tested using a robotic/universal force-moment sensor (UFS) testing system. Both anterior tibial and rotatory loads were applied between full extension and 90° of knee flexion, and the 5 degrees of freedom (DOF) kinematics and in situ forces of the 2 bundles of the intact ACL, as well as those of the 2 grafts in DB-ACLR, were measured and compared.
Materials and Methods
Ten fresh-frozen human cadaveric knees (43.3 ± 8.1 years; range, 29-52 years) were used in this study. Each specimen was screened for bony abnormalities and osteoarthritis by using radiographs. Specimens were stored in airtight plastic bags at –20°C until 24 hours before testing, at which time, they were thawed at room temperature.38,39 The femur and tibia were then cut approximately 20 cm from the joint line. The semitendinosus and gracilis tendons were harvested from each knee to be used as the ACL replacement graft. The surrounding skin and muscles more than 10 cm away from the joint line were removed so that the bones were exposed. The fibula was rigidly fixed to the tibia with a cortical screw to maintain its anatomical position. Throughout the experiment, the specimens were kept moist with 0.9% saline solution. The femur and tibia were each secured within custom-made aluminum cylinders by using an epoxy compound (Fibre Glass-Evercoat, Cincinnati, Ohio) with transfixing bolts. The specimen was then mounted in a robotic/UFS testing system.10,11,23,28 To best simulate clinical examinations used to diagnose ACL deficiency, the femur was rigidly mounted to the base of the robotic manipulator (PUMA Model 726, Unimate Inc, Danbury, Conn), and the tibia was fixed to the end-effector of the robotic manipulator (Model 4015, JR3 Inc, Woodland, Calif) (Figure 1). The position and orientation repeatability of the robotic manipulator are less than 0.2 mm and 0.2°. 28 The UFS can measure 3 forces and 3 moments along a Cartesian coordinate system and has a repeatability of 0.2 N for forces and 0.01 N·m for moments. 28
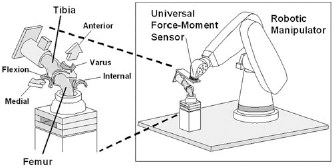
The robotic/universal force-moment sensor testing system with a cadaveric knee specimen.
The experimental protocol and data acquired are outlined in Table 1. First, the path of passive flexion-extension of the intact knee was determined from full extension to 90° of flexion by moving the tibia in 1° increments of flexion while the forces and moments at each flexion angle were minimized (within 0.5 N and 0.2 N·m). This path served as the reference position from which knee kinematics were measured and provided the starting position at each angle of flexion for the application of external tibial loads for the remainder of the tests.19,24,35,40 With the robot, the following external loading conditions were applied to the tibia: (1) a 134-N anterior tibial load at full extension, 15°, 30°, 60°, and 90° of knee flexion and (2) combined rotatory loads of 10 N·m valgus and 5 N·m internal tibial torques at 15° and 30° of knee flexion.24,40 These loading conditions were designed to simulate clinical examinations used to diagnose ACL deficiency, such as the Lachman, anterior drawer,27,31,34 and pivot-shift tests.9,16,21 The resulting 5 DOF kinematics of the intact knee, including anterior-posterior, medial-lateral, and proximal-distal translations, as well as internal-external and varus-valgus rotations, were determined in response to both external loading conditions.
Experimental Protocol and the Corresponding Data Acquired a
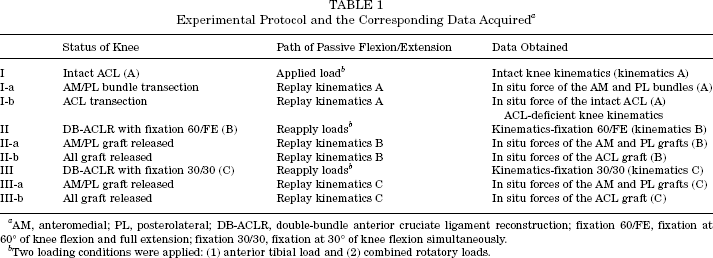
AM, anteromedial; PL, posterolateral; DB-ACLR, double-bundle anterior cruciate ligament reconstruction; fixation 60/FE, fixation at 60° of knee flexion and full extension; fixation 30/30, fixation at 30° of knee flexion simultaneously.
Two loading conditions were applied: (1) anterior tibial load and (2) combined rotatory loads.
The in situ forces of the ACL, that is, the tension that each bundle experiences in its original anatomical position during knee motion, and the force distribution between the AM and PL bundles were determined in the following manner. After we carefully separated and transected 1 bundle of the ACL through a medial miniarthrotomy, 29 the 5 DOF kinematics of the intact knee were replayed (for 1 bundle transaction and then the other), and the resulting forces were measured for the 2 different knee states: bundle-deficient and ACL-deficient. On the basis of the principle of superposition, the vector differences in forces between the intact and the ACL-deficient knees represented the in situ force in the ACL. 19 Similarly, the force distribution between the AM and PL bundles was determined as the vectorial difference between the bundle-deficient and the ACL-deficient knee states. To assess changes in knee kinematics associated with ACL deficiency, the same external loading conditions were again applied to the ACL-deficient knee in force-control mode, and the resulting 5 DOF kinematics were determined.
Next, the anatomical DB-ACLRs were performed using 2 femoral tunnels and a single tibial tunnel.40,41 A looped semitendinosus tendon was used for the AM graft, and a looped gracilis tendon was used for the PL graft. The mean diameter of the proximal end of the AM and PL grafts was 7.2 ± 1.3 mm (range, 6-8 mm) and 5.5 ± 1.0 mm (range, 5-7 mm), respectively. Both the AM and PL femoral tunnels were positioned using a Kirschner wire at the center of the insertion of each bundle of the ACL by visual inspection of the remnants of the transected bundles. The femoral tunnels were first drilled 30 mm deep from inside the joint using a cannulated drill bit chosen according to the graft diameter; then the femoral tunnels were drilled through with a 4.5-mm-diameter cannulated drill (EndoButton Drill, Acufex, Smith & Nephew, Andover, Mass). A single tibial tunnel was placed using a Protrac tibial guide (Acufex, Smith & Nephew) positioned 5 to 7 mm anterior to the tibial insertion site of the PCL. 17 The diameter of the tibial tunnel was equal to the diameter of the AM and PL combined graft (mean, 10.1 ± 1.1 mm; range, 9-11 mm). The semitendinosus and gracilis tendon grafts were then pulled through the tibial tunnel and preconditioned by moving the knee through 5 cycles of the full range of knee flexion while applying a 22-N pretension to each graft.
For the first fixation protocol, fixation 60/FE, the knee flexion angles of 60° of knee flexion and full extension were selected for AM graft fixation and PL graft fixation, respectively, because they are the angles that correspond to the highest in situ force found for each bundle of the intact ACL. 12 The double-looped gracilis tendon, replicating the PL bundle, was fixed to the tibia with the knee at full extension (>; 0°) while a 67-N posterior tibial load was applied and 22 N of initial graft tension was maintained (Figure 2 A2). This fixation method has been previously shown to closely restore knee kinematics and in situ force in the ACL graft to those of the intact knee after ACL reconstruction. 15 The semitendinosus tendon graft, replicating the AM bundle, was then fixed to the tibia with the knee flexed 60° in the same manner (Figure 2 A1). For the second fixation protocol, fixation 30/30, both grafts were fixed to the tibia at 30° of flexion simultaneously while a 67-N posterior tibial load 15 was applied and 22 N of initial graft tension was maintained on each graft separately (Figure 2B). This fixation protocol was intended to simulate a common fixation procedure used in the clinical setting. 26 Both protocols used the EndoButton CL (Smith & Nephew) for femoral fixation and a spiked washer and screw (Mitek Products, Norwood, Mass) for tibial fixation (Figure 2B).
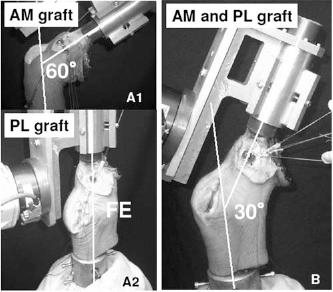
A1 and A2, fixation 60/FE: anteromedial graft fixation was performed at 60° of knee flexion after posterolateral graft fixation at full extension (FE). B, fixation 30/30: both grafts were fixed at 30° of knee flexion simultaneously.
For each fixation protocol, the same 2 loading conditions, that is, an anterior tibial load and combined rotatory loads, were applied, and the corresponding 5 DOF reconstruction kinematics were recorded. One of the AM and PL grafts was released individually (in alternating order), and the kinematics were replayed to obtain the in situ forces in the graft, as previously described via the principle of superposition. Finally, the second graft was released, and the in situ force in the total graft was determined.40,41
The 5 DOF knee kinematics obtained were compared for the 4 different knee conditions: (1) intact knee, (2) ACL-deficient knee, (3) ACL-reconstructed knee with fixation 60/FE, and (4) ACL-reconstructed knee with fixation 30/30. The overall in situ forces of the intact ACL and the ACL replacement grafts for 2 fixation protocols were compared. Furthermore, the force distributions of the AM and PL bundles were also compared with those of the AM and PL grafts. Based on our previous data, a power analysis was performed (power = .80, significance level = .05), so differences of 3 mm for anterior tibial translation (ATT) and 20 N for in situ force measurements could be detected. It was determined that 10 knee specimens were required for this study. Because all variables were measured on each specimen, statistical analysis of the ATT, internal tibial rotation (ITR), and in situ forces were performed using a 2-factor repeated measures analysis of variance, with knee state and flexion angle as the factors. This analysis has the advantage of being sensitive to relative changes occurring within an individual knee and minimizing the effects of interspecimen variability.36,38
Multiple contrasts were performed to evaluate the effects of ACL reconstruction at specific angles of knee flexion. Statistical significance was set at P < .05.
Results
In response to a 134-N anterior tibial load, the ATT for the intact knee ranged from 4.1 ± 2.2 mm at full extension to 8.3 ± 3.1 mm at 30° of knee flexion (Table 2). After ACL transection, these values significantly increased by more than 2-fold for all the flexion angles tested, measuring 10.0 ± 3.9 mm to 18.0 ± 4.0 mm (P = .0001). After ACL reconstruction, the ATT decreased significantly from that of the ACL-deficient knee in both fixation protocols (P = .0001). For fixation 30/30, the ATT ranged from 4.3 ± 3.4 mm to 8.5 ± 3.6 mm and was not significantly different from the intact knee. The only exception was at 90° of knee flexion, where the ATT was 1.1 mm less than the intact knee (P = .0435). For fixation 60/FE, the ATT ranged from 5.5 ± 3.5 mm to 9.0 ± 3.6 mm and was 1.4 mm higher at full extension and 15° of knee flexion (P= .0146 and .0235, respectively) but 1.7 mm lower at 90° of flexion than the intact knee (P= .0018). When comparing the ATT between the 2 fixation protocols, there were significant differences at full extension and at 15° of knee flexion (P = .0351 and .0308, respectively), as the ATT for fixation 60/FE was a mean of 1.2 mm higher than for fixation 30/30.
Anterior Tibial Translation (mm) in Response to a 134-N Anterior Tibial Load (mean ± SD) a
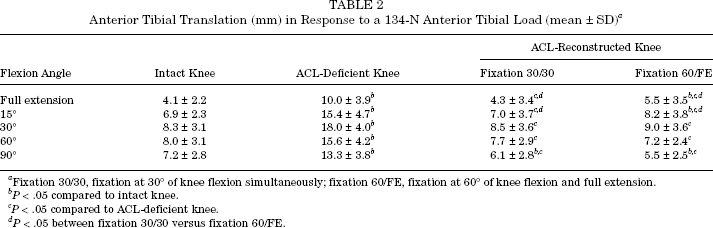
Fixation 30/30, fixation at 30° of knee flexion simultaneously; fixation 60/FE, fixation at 60° of knee flexion and full extension.
P < .05 compared to intact knee.
P < .05 compared to ACL-deficient knee.
P < .05 between fixation 30/30 versus fixation 60/FE.
The overall in situ forces of the intact ACL and the entire ACL grafts for both fixation protocols in response to an anterior tibial load are detailed in Table 3. For the intact ACL, the overall in situ force ranged from 74 ± 16 N at 90° to 113 ± 17 N at 30° of knee flexion. For fixation 30/30, the overall in situ force in the ACL graft ranged from 74 ± 22 N to 114 ± 18 N at 90° and 15° of knee flexion, respectively, and there were no significant differences compared with the intact ACL. For fixation 60/FE, the overall in situ force in the graft ranged from 79 ± 21 N to 106 ± 23 N at 90° and 15° of knee flexion, respectively; again, there were no significant differences when compared with the intact ACL. When comparing the overall in situ force in the ACL graft between the 2 fixation protocols, there were also no significant differences at all knee flexion angles except at full extension, where the in situ force of the entire ACL graft for fixation 60/FE was 22 N lower than that for fixation 30/30 (P = .0001).
In Situ Force in the Anterior Cruciate Ligament (ACL) and ACL Graft (N) in Response to a 134-N Anterior Tibial Load (mean ± SD) a
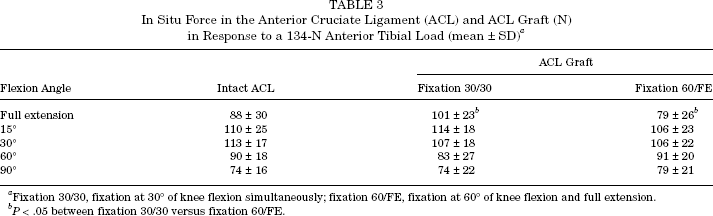
Fixation 30/30, fixation at 30° of knee flexion simultaneously; fixation 60/FE, fixation at 60° of knee flexion and full extension.
P < .05 between fixation 30/30 versus fixation 60/FE.
In contrast, the force distribution between the separate AM and PL grafts was significantly different from the distribution between the AM and PL bundles of the intact ACL for both fixation protocols. For intact ACL, the magnitude of the in situ forces for the AM bundle ranged from 43 ± 17 N at full extension to 82 ± 17 N at 60° of knee flexion, whereas those of the PL bundle were 57 ± 18 N and 10 ± 4 N, respectively (Figures 3 and 4). For fixation 30/30, in situ forces in the AM graft were generally lower, ranging from 41 ± 14 N to 65 ± 23 N at 15° and 60° of knee flexion, respectively. Significant differences between the AM graft and the AM bundle were found at 30° and 60° of knee flexion (P = .0001). Conversely, the in situ forces in the PL graft were generally higher, notably at 15° of knee flexion, where the in situ force was as high as 73 ± 16 N (Figure 4). There were significant differences between the PL graft and the PL bundle at 15° and 30° of knee flexion (P = .0001), resulting in a mean of 34% increase for the PL graft over those for the PL bundle.
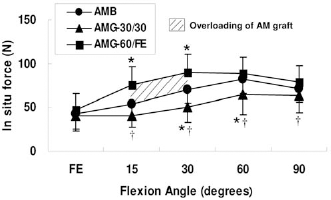
In situ force in the anteromedial (AM) bundle (AMB) and AM graft (AMG) in response to 134-N anterior tibial load for the 2 different fixation protocols. *P < .05 compared with AMB. †P < .05 compared with AMG-60/FE.
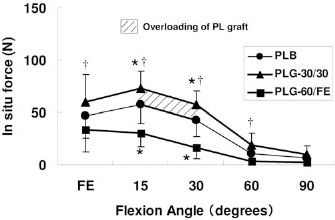
In situ force in the posterolateral (PL) bundle (PLB) and PL graft (PLG) in response to 134-N anterior tibial load for 2 different fixation protocols. *P < .05 compared with PLB. †P < .05 compared with PLG-60/FE.
For fixation 60/FE, in situ force in the AM graft was found to be higher, ranging from 47 ± 19 N to 90 ± 21 N at full extension and 30° of knee flexion, respectively, which represents a mean of 46% increase in load for the AM graft (Figure 3). Significant differences between the AM graft and the AM bundle were found at 15° and 30° of knee flexion (P= .0001). In contrast, the in situ force in the PL graft was very low at 90° of knee flexion (Figure 4). There were significant differences between the PL graft and the PL bundle at 15° and 30° of knee flexion (P = .0001). When comparing the in situ forces in each graft between the 2 fixation protocols, the in situ force of the AM graft for fixation 60/FE was significantly higher than that for fixation 30/30 at all knee flexion angles (P = .0001) except at full extension (P = .0762) (Figure 3). On the other hand, the in situ force in the PL graft for fixation 30/30 was significantly higher than that for fixation 60/FE at all knee flexion angles except 90° of knee flexion (P = .0001 from full extension to 60° of knee flexion, P = .0512 at 90° of knee flexion) (Figure 4).
In response to combined rotatory loads, the coupled ATT for the intact knee was 4.7 ± 2.7 mm and 7.0 ± 3.0 mm at 15° and at 30° of knee flexion, respectively, whereas the ITR was 13.8° ± 5.2° and 17.9° ± 6.0°, respectively (Table 4). After ACL transection, both the coupled ATT and ITR increased significantly (P = .0001 at 15° and 30° of flexion). After ACL reconstruction with fixation 30/30, the coupled ATT was reduced by 1 mm (P = .0001), whereas the ITR was reduced by 3.4° at 30° of knee flexion (P = .0001) compared with the intact knee. In contrast, for fixation 60/FE, the coupled ATT was 1.1 mm greater at 15° of flexion (P = .0001), whereas the ITR returned to the level of the intact knee (P = .1982 and .0878 at 15° and 30° of flexion, respectively). Comparison between the 2 fixation protocols revealed statistically significant differences in both the ATT and ITR for all knee flexion angles examined (P = .0001). In general, fixation 30/30 had smaller translation and rotation than fixation 60/FE.
Kinematics Data of Coupled Anterior Tibial Translation and Internal Tibial Rotation in Response to Combined Rotatory Loads (mean ± SD) a
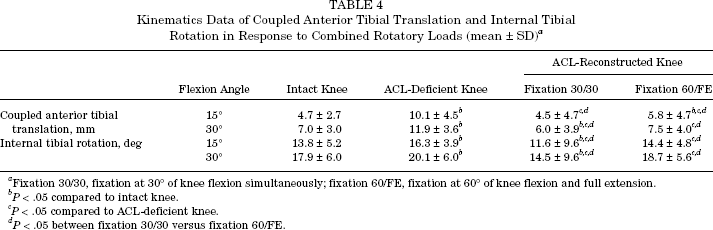
Fixation 30/30, fixation at 30° of knee flexion simultaneously; fixation 60/FE, fixation at 60° of knee flexion and full extension.
P < .05 compared to intact knee.
P < .05 compared to ACL-deficient knee.
P < .05 between fixation 30/30 versus fixation 60/FE.
The overall in situ force in the intact ACL in response to combined rotatory loads was 80 ± 15 N at 15° and 67 ± 27 N at 30° of knee flexion, whereas for fixation 30/30, these values were 82 ± 19 N and 80 ± 18 N, respectively. Similarly, for fixation 60/FE, the overall in situ force was 70 ± 17 N and 67 ± 19 N, respectively. No significant differences were found for the overall in situ forces between the ACL grafts and the intact ACL.
Meanwhile, in terms of the force distribution between the AM and PL grafts, overloading of the PL graft became apparent for fixation 30/30. Under combined rotatory loads, the in situ force for the AM bundle of the intact ACL was 42 ± 13 N and 42 ± 15 N at 15° and 30° of knee flexion, respectively, whereas those for the PL bundle were 39 ± 19 N and 26 ± 17 N, respectively (Table 5). For fixation 30/30, the in situ force in the PL graft increased to 57 ± 21 N and 51 ± 14 N (P = .0001), whereas those for the AM graft decreased to 26 ± 13 N and 30 ± 15 N (P = .0001 and .0012 at 15° and 30° of flexion, respectively). On average, the in situ force in the PL graft increased 67% over that of the PL bundle. For fixation 60/FE, the forces of the AM and PL grafts were not significantly different from those of the AM and PL bundles. Comparison between the 2 fixation protocols revealed that fixation 30/30 had a significantly lower in situ force in the AM graft (P = .0001 and .0027 at 15° and 30° of knee flexion, respectively) and a significantly higher in situ force in the PL graft (P = .0001) than fixation 60/FE.
In Situ Force in the Anteromedial (AM) and Posterolateral (PL) Bundles and the AM and PM Grafts (N) in Response to Combined Rotatory Loads (mean ± SD) a
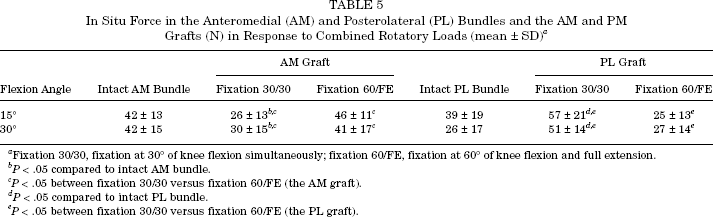
Fixation 30/30, fixation at 30° of knee flexion simultaneously; fixation 60/FE, fixation at 60° of knee flexion and full extension.
P < .05 compared to intact AM bundle.
P < .05 between fixation 30/30 versus fixation 60/FE (the AM graft).
P < .05 compared to intact PL bundle.
P < .05 between fixation 30/30 versus fixation 60/FE (the PL graft).
Discussion
In this study, the 5 DOF knee kinematics at selected angles of knee flexion and the corresponding in situ forces of the ACL and the ACL replacement graft in response to externally applied loads were quantitatively evaluated using the robotic/UFS testing system. More important, the force distributions between the AM and PL grafts were determined and compared with those of the respective bundles of the intact ACL. The kinematics data obtained in this study are consistent with published work from our research center and others.11,19,20,24,27,37,40 In addition, the in situ force in the ACL and force distribution data for all are also similar to previous work.12,29
The findings clearly suggest that the knee flexion angles for graft fixation play a significant role in the force distribution within the AM and PL grafts after DB-ACLR. Furthermore, these results support our hypothesis, as the fixation of the 2 grafts at 30° of knee flexion did increase the force of the PL graft. This fixation protocol actually resulted in a mean of 34% and 67% increase of the in situ force in the PL graft in response to an anterior tibial load and combined rotatory loads, respectively. Clinically, such substantial increases in the magnitude of forces in the graft could potentially lead to graft failure, especially for the shorter and smaller PL graft.
On the other hand, when the grafts were fixed at 60° of knee flexion and full extension, the angles that correspond to the highest in situ force found for each bundle of the intact ACL, 12 the force distribution between the AM and PL grafts was actually similar to those of the intact bundles under combined rotatory loads. However, in response to an anterior tibial load, the in situ force in the AM graft was up to 46% higher than that in the AM bundle (Figure 3). Concomitantly, the in situ force in the PL graft was lower than that in the PL bundle (Figure 4), with a corresponding increase of the ATT near full extension. These results suggest insufficiency of PL graft function. 12
Fixation 30/30 causes overloading to the PL graft (Figures 5 and 6), which may predispose the PL graft to stretching or failure because it is shorter in length as well as smaller in diameter than the AM graft. On the other hand, fixation 60/FE might be a better choice for the PL graft as its in situ force in response to the externally applied loads studied did not exceed the level of the PL bundle of the intact ACL. However, it should be recognized that the AM graft was overloaded by up to 46% during anterior tibial load. From the results of this study, it is evident that any protocol for graft fixation should recognize that the 2 grafts are necessary to function under different loading conditions; that is, the AM graft is more dominant for anterior tibial load, whereas the PL graft is more dominant for rotatory load.
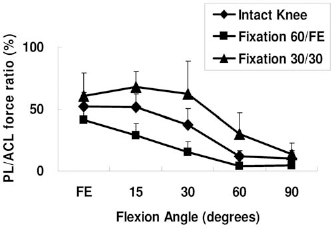
Force ratios of the posterolateral/anterior cruciate ligament (PL/ACL) for the intact knee versus ACL-reconstructed knees of the 2 fixation protocols in response to a 134-N anterior tibial load.
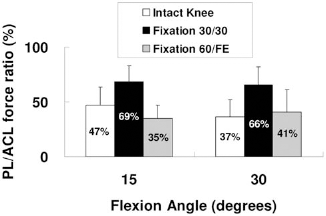
Force ratios of the posterolateral/anterior cruciate ligament (PL/ACL) at 15° and 30° of flexion for the intact knee versus ACL-reconstructed knees of the 2 fixation protocols in response to combined rotatory loads.
The initial graft tension applied to the first graft could reduce significantly during fixation of the second graft; that is, it would be possible that the PL graft tension changed when tension was applied to the AM graft in fixation 60/FE. The data suggest otherwise, as the tension of the PL graft (fixed at full extension) had already decreased by a significant amount as the knee flexed from full extension to 60° of knee flexion before the AM graft was fixed.3,6 Therefore, the remaining tension in the PL graft would not significantly decrease after the AM graft fixation at 60° of knee flexion.
A limitation of this study was that the order of the fixation protocols could not be randomized. Another limitation of this study is the fact that it is a time zero study. Therefore, the effects of stress relaxation of the hamstring graft have not been accounted for and must be considered. 8 These relatively simple external loading conditions used are limited to simulate those loads used in clinical examinations. Obviously, these loads are smaller than those experienced during physiological activities of daily living. Nevertheless, significantly higher loads could already be found to occur in the individual grafts than in the intact bundles (Figures 5 and 6). Hence, for in vivo activities such as running, jumping, and cutting, which would cause much greater external loads, the potential of overloading in the 2 grafts would be greatly increased.
When considering each graft separately, the force in the AM graft would be too high or too low when fixed at 60° or 30° of knee flexion, respectively (Figure 3), whereas the force in the PL graft would be too high or too low when fixed at 30° of knee flexion or full extension, respectively (Figure 4). Therefore, a future investigation is needed to find the optimal knee flexion angles for graft fixation between these ranges, that is, between 60° and 30° of knee flexion for AM graft fixation and between 30° of knee flexion and full extension for PL graft fixation. Because of the interactive nature between the grafts, the load sharing by the 2 grafts is affected when fixed at different angles. Therefore, it is necessary to conduct future studies to determine the effects of 2 variables separately, that is, knee flexion angles for AM graft fixation and for PL graft fixation. In addition, the effect of the magnitude of initial graft tension on each graft for adjusting force distribution between the 2 grafts should also be studied. Armed with such basic science data, the long-term clinical outcome studies could be designed and performed.
Footnotes
Acknowledgment
The financial support of NIH grant AR 39683 is gratefully acknowledged. The authors thank Dr. Yasuyuki Ishibashi, Hirosaki University, for raising the research question and Maribeth Thomas, BS, Jens Stehle, MD, Tan Duy Nguyen, MD, and özgür Dede, MD, of the Musculoskeletal Research Center for technical assistance.
No potential conflict of interest declared.