
Abstract
Background: The cyclooxygenase-2 specific inhibitor valdecoxib has not been approved in the United States for treatment of acute pain.
Hypothesis:Valdecoxib 20 mg twice daily or once daily (both with a 40-mg loading dose) is not clinically inferior to tramadol for treating the signs and symptoms of acute ankle pain.
Study Design:Randomized, controlled clinical trial; Level of evidence, 1.
Methods:Patients (N = 829) with acute firstor second-degree ankle sprain received 7 days' treatment with valdecoxib 20 mg either twice daily or once daily (both with 40-mg loading dose), tramadol 50 mg 4 times daily, or placebo. The primary end point was Patient's Assessment of Ankle Pain visual analog scale on day 4; a test of noninferiority compared valdecoxib with tramadol.
Results:On day 4, both valdecoxib doses were significantly better versus placebo and were comparable with tramadol in relieving ankle pain. On day 7, valdecoxib, but not tramadol, significantly reduced pain versus placebo. On days 4 and 7, more patients resumed normal walking with valdecoxib (45%-47% and 73%-79%, respectively) than with placebo (35% and 64%, respectively) or tramadol (38% and 67%, respectively). In contrast to valdecoxib, the number of withdrawals due to adverse events was significantly higher in the tramadol group (12.2% vs 3.4%; P = .0005).
Conclusions:Valdecoxib was comparable with tramadol and was significantly better than placebo in treating acute ankle sprain, and it enabled more patients to resume normal walking on days 4 and 7. Both valdecoxib and tramadol were well tolerated.
Ankle sprains are the most common sports-related soft tissue injury, with around 1 million people seeking medical attention for lateral ankle sprains each year in the United States alone.16–18,35,44 More than 40% of ankle sprains have the potential to cause chronic problems. 37 These injuries occur when stress is applied while the ankle is in an unstable position, causing the ligaments to overstretch. Ankle sprains are usually classified as first degree when they involve stretching of ligamentous fibers; second degree when they involve a tear of some portion of the ligament, with associated pain and swelling; and third degree when they involve complete ligamentous disruption. 25 Although most ankle sprains heal with no residual disability, initial treatment for pain and inflammation is essential because some untreated injuries may lead to long-term morbidity, including ankle instability, osteochondral injury, arthritis, and chronic pain. 32
Inflammatory response during acute ankle injury causes pain, hyperalgesia, erythema, and edema. 46 During this process, increased capillary permeability leading to hemorrhage and accumulation of fluid at the site of injury can limit motion, compound tissue damage, and delay healing. 32 Thus, inflammation can limit a patient's ability to perform rehabilitation required for proper healing, and it may delay a rapid return to normal function. Early treatment is, therefore, important for reducing pain and inflammation and enabling a speedy return to normal activity. 23 In addition, patients with ankle sprain often want relief of pain as well as a short recovery and fewer adverse effects.13,23,43 Immediate treatment for ankle sprain aims to prevent swelling and hemorrhage. Guidelines from the American Academy of Orthopaedic Surgeons suggest rehabilitation with nonsteroidal anti-inflammatory drugs (NSAIDs) for up to 3 weeks as well as resting the ankle, application of ice to limit the swelling, compressive bandages for immobilization and support, and elevation for 48 hours (RICE). During this period, weightbearing should be started as tolerated by the patient.7,33
Clinical trials have demonstrated that NSAIDs and cyclooxygenase-2 (COX-2) specific inhibitors can relieve pain, reduce inflammation, and facilitate return to full functioning.5,13,14,23,33,42,45 However, even with short-term use, nonspecific NSAIDs (which block COX-1 in addition to COX-2) can cause gastrointestinal (GI) toxicity20,22,40 and platelet dysfunction.27,28,40 This may result in an increase in bleeding time9,21,38 and may contribute to subcutaneous bleeding leading to ecchymosis,14,45 which can potentially negatively affect recovery from an injury. 14
In contrast, COX-2 specific inhibitors do not inhibit COX-1 at therapeutic doses and so provide analgesic and anti-inflammatory efficacy that is similar to nonspecific NSAIDs but with superior GI and platelet safety. †† Valdecoxib is a COX-2 specific inhibitor that was approved for relief of the signs and symptoms of osteoarthritis, adult rheumatoid arthritis, and primary dysmenorrhea in the United States and in a number of countries around the world.2,4,10,26,31 However, following completion of this study, sales of valdecoxib were suspended in the United States at the request of the Food and Drug Administration, and subsequently in most countries worldwide. Valdecoxib has been investigated for the treatment of acute pain and has been demonstrated to be efficacious and well tolerated in a variety of surgical models, including oral surgery, knee or hip arthroplasty, and bunionectomy.6,11,12,15,36
References 2, 3, 10, 14, 19, 26, 31, 39, 41, 45.
Tramadol is a synthetic, centrally-acting analgesic agent with 2 distinct synergistic mechanisms of action, acting as both a weak opioid agonist and an inhibitor of monoamine neurotransmitter reuptake. At doses of 50 to 100 mg every 4 to 6 hours, tramadol has been used to manage pain in a wide range of indications, including musculoskeletal diseases and acute trauma.29,30,34 However, tramadol is commonly associated with adverse effects such as dizziness, nausea, dry mouth, and sedation. 30
The objectives of the present study were to determine the efficacy, safety, and tolerability of valdecoxib (20 mg twice daily or 20 mg once daily, both with a loading dose of 40 mg on day 1), its noninferiority to tramadol (50 mg 4 times daily), and its superiority to placebo in relieving the signs and symptoms of a first- or second-degree ankle sprain.
Methods
Patients
Patients aged 16 to 65 years who had sustained an acute first-degree or second-degree lateral ankle sprain (specifically of the anterior talofibular ligament and/or calcaneofibular ligament) were enrolled, provided injury occurred within 48 hours of the first dose of study medication. Diagnosis of first-degree or second-degree ankle sprain was based on established criteria for the classification of ankle sprain (grades I-III) as described in the study protocol. Second-degree sprain was established based on tenderness to palpation and mild laxity compared with the contralateral ankle. The overall assessment of injury severity was based on scores from the Patient's Assessment of Ankle Pain visual analog scale (VAS) as well as results from the Patient's Assessment of Normal Function/Activity, Patient's Global Assessment of Ankle Injury, and Physician's Global Assessment of Ankle Injury scales.
The enrollment criterion for the study was ankle pain of moderate to severe intensity on full weightbearing. This range was defined as a baseline score of 60 mm or more on the Patient's Assessment of Ankle Pain VAS, which ranged from 0 (no pain) to 100 (severe pain). In addition, patients had to have a rating of at least 2 on both the Patient's Global Assessment of Ankle Injury and the Patient's Assessment of Normal Function/Activity scales. The Patient's Global Assessment of Ankle Injury is a 5-point scale ranging from very good to very poor as follows: 1 (very good) = no symptoms or limitation of normal activities; 2 (good) = mild symptoms, no limitation of normal activities; 3 (fair) = moderate symptoms, limitation of some normal activities; 4 (poor) = severe symptoms, inability to carry out most normal activities; and 5 (very poor) = very severe symptoms that are intolerable, inability to carry out all normal activities. The Patient's Assessment of Normal Function/Activity is a 5 point scale as follows: 1 = normal walking/activity and no pain; 2 = normal walking/activity with pain; 3 = mildly restricted walking due to pain, cannot resume normal activities; 4 = moderately restricted walking due to pain, cannot resume normal activities; and 5 = severely restricted walking due to pain, cannot resume normal activities. The Physician's Global Assessment of Ankle Injury is based on the patient's signs and symptoms (including swelling, tenderness, and limitation of range of movement) and is graded using the following 5-point scale: 1 = very mild; 2 = mild; 3 = moderate; 4 = severe; and 5 = very severe.
Patients were excluded from the study if a similar injury affecting the same joint had occurred within the past 6 months, if they had a complete rupture of the ankle ligaments (third-degree sprain), or if the injury was part of a bilateral ankle injury or was concurrent with an ipsilateral knee injury. Bed rest, hospitalization, surgery, or use of a nonremovable rigid cast were also criteria for exclusion. Patients were excluded if they had active GI, renal, or hepatic disease; upper GI ulceration within the past 30 days; or a history of epilepsy or a recognized risk for seizure, such as head trauma, metabolic disorders, alcohol/drug withdrawal, or central nervous system (CNS) infections. Patients were not eligible if they had received treatment with corticosteroids in the previous 8 weeks; had taken any analgesics in the previous 6 hours, or 24 hours in the case of long-acting NSAIDs; or if they had a known hypersensitivity to NSAIDs, COX-2 specific inhibitors, sulfonamides, or tramadol (aspirin ≤325 mg/d for cardiovascular prophylaxis and inhaled steroids were permitted).
The study was conducted at a total of 87 centers; 14 centers were located in Europe, and 73 were in the United States. All centers received prior ethics committee or institutional review board approval. The centers were chosen based on qualifications, including extensive experience in ankle sprain management in clinical practice, previous experience with clinical trials, and availability of a full-time study coordinator. The patients or their legal representatives were informed about the nature, purpose, and risk of participating in the study by the investigator or designated representative, and all patients (or their legal guardian if the subject was a minor) provided written informed consent before undergoing any study procedures.
Study Design
This was a multicenter randomized, double-blind, parallel-group, placebo- and active-controlled study. Principal investigators at all centers were directed by the study sponsor to conduct the study and to follow entrance and assessment criteria in accordance with the study protocol. Investigators were responsible for adhering to study procedures and for keeping study drug records.
Eligible subjects were randomized to treatment at each site in the order in which they were enrolled in the study. Each site was provided with blocks of balanced treatment allocations based on a block size of 7; the treatment randomization list was computer generated by the study sponsor before the start of the study. Screening and randomization were performed on day 1. At screening, written informed consent and medical history were obtained, and an abbreviated physical examination, pregnancy test (if applicable), and clinical laboratory tests were performed. The subject completed an ankle pain VAS, global assessment and assessment of normal function/activity, and the physician completed a global assessment. If, after the screening procedures, the subject qualified for entry into the study, he or she was randomized.
Throughout the study, patients, physicians, and study personnel were blinded to treatment assignment; the sponsor was blinded until after the data analyses. Both valdecoxib and tramadol had a matching placebo; all capsules and tablets and dosing schedules were outwardly identical. Unblinding was permitted only in emergency situations, in which knowledge of the treatment was necessary for the proper clinical management of the subject. No unblinding was necessary for this study.
Patients meeting eligibility criteria were randomized in the ratio of 2:2:2:1 to receive 7 days of treatment with valdecoxib 20 mg twice daily or once daily (both with a 40-mg loading dose), tramadol 50 mg 4 times daily, or matching placebo, respectively. Patients could take rescue analgesia, which was acetaminophen (paracetamol in Europe) 500 mg every 6 hours as needed up to 4 g/d, but not within 6 hours before any scheduled study visit. In addition, patients were permitted to receive traditional remedies such as RICE therapy as well as other nonpharmacologic interventions considered to be standard care, including crutches, cane, contrast baths, ankle taping/bracing, rigid double-upright ankle brace, strengthening and proprioceptive exercises, transcutaneous electrical nerve stimulation (TENS), diathermy, massage therapy, ultrasound, and acupuncture.
On days 1 (pretreatment), 4, and 7, or at the time of early withdrawal, patients were asked to rate their pain on weightbearing according to the Patient's Assessment of Ankle Pain VAS, the Patient's Global Assessment of Ankle Injury, and the Patient's Assessment of Normal Function/Activity. In addition to patient assessments, physicians assessed the severity of the ankle injury (using the Physician's Global Assessment of Ankle Injury) as previously described. Patients also completed the American Pain Society (APS) questionnaire1,8 before administration of the first dose of the study drug and on days 2 through 7 (or early termination visit) before taking their first daily dose of study medication. Patients and their physicians were asked to rate their willingness to use the same medication again for an ankle injury on a scale of 1 (very unwilling) to 10 (very willing), and patients rated their overall satisfaction with their study medication on a scale of 1 (very satisfied) to 5 (very dissatisfied). Patients were also monitored for adverse events at each visit.
For quality assurance, the study sponsor routinely monitored the study. At these visits, study procedures were reviewed, case report form data and informed consents were compared with original clinical records, drug accountability was assessed, data queries were resolved, and protocol deviations were discussed with the investigator. Telephone contact was maintained and documented with the investigators between site visits. In addition, the study was subjected to internal quality review by the sponsor. Before the database closure, a database quality acceptance sampling was performed. The estimated error rate resulting from this quality acceptance procedure was 0.01%. As this error rate was lower than the departmental standard for an acceptable error rate (<0.1%), the database met the departmental standard. The measures employed in this study (Patient's Assessment of Ankle Pain VAS, Patient's and Physician's Global Assessment of Ankle Injury, and Patient's Assessment of Normal Function/Activity) are widely used in studies involving the treatment of pain and are generally recognized as reliable, accurate, and relevant.14,33
Efficacy and Safety End Points
The primary efficacy end point in this study was the Patient's Assessment of Ankle Pain VAS score on weightbearing day 4 in the evaluable population. Secondary efficacy and safety end points during the 7-day study were as follows: Patient's Assessment of Ankle Pain VAS score on weightbearing day 7, Patient's and Physician's Global Assessments of Ankle Injury score (days 4 and 7), Patient's Assessment of Normal Function/Activity score (days 4 and 7), APS questionnaire score (days 2-7), patient's and physician's willingness to use the same medication, and patient's overall satisfaction with study medication.
Data for incidence of any CNS-related adverse events (combined rates of somnolence, dizziness, vertigo, nausea, and vomiting) and GI-related adverse events (combined rates of abdominal pain, dyspepsia, and nausea) were collected on all visits after the screening. Adverse events reported during the study were summarized by the investigator's worst assessment of severity (mild, moderate, severe) and coded using modified World Health Organization Adverse Reaction Terminology (WHOART) dictionary. Adverse events were also tabulated by body system. There were no serious adverse events in this study.
Statistical Evaluation
The sample size calculation was based on a test of noninferiority for valdecoxib 20 mg twice daily and for tramadol 50 mg 4 times daily as measured on a 100-mm VAS for the primary efficacy measure. The hypothesis for noninferiority of valdecoxib relative to tramadol for pain VAS was accepted if the upper 95% confidence interval (CI) for the treatment difference between valdecoxib and tramadol was less than 10 mm (on a 100-mm scale). It was determined that a sample size of 192 patients in each treatment group had a 90% power using a 2-group, 2.5%, 1-sided t test to reject the null hypothesis that valdecoxib is clinically inferior to tramadol in favor of the alternative hypothesis that valdecoxib is clinically noninferior. In addition, the sample size had a 93% power to detect a clinically significant difference in pain VAS between placebo and active treatments.
A general linear model, with fixed effects for center and treatment and baseline VAS as a covariate, was used for the test of noninferiority. If noninferiority was demonstrated between valdecoxib 20 mg twice a day and tramadol 50 mg 4 times a day for the primary efficacy end point, another test of noninferiority compared valdecoxib 20 mg once a day and tramadol 50 mg 4 times a day. For these analyses, the differences in the least squares (LS) mean, the standard error of the differences, the 95% CI for the difference, and the level of statistical significance were calculated. A type I (α) error for all noninferiority hypothesis testing was set at .025 one-sided, and all tests of superiority were set at .05 two-sided.
For the secondary efficacy variables, tests of superiority were conducted separately for comparisons of valdecoxib 20 mg twice daily and valdecoxib 20 mg once daily versus tramadol; active treatments were not compared with placebo for the secondary end points. A general linear model with fixed effects for center and treatment, with pretreatment score as a covariate, was used for continuous variables. The differences in LS means, the standard error of the differences, the 95% CI for the difference, and statistical significance were calculated using a χ2 test (replaced by a Fisher exact test if the expected cell size was smaller than 5). Cochran-Mantel-Haenszel statistics were used in analyzing ordered secondary categorical responses. If required, these responses were analyzed using the Fisher exact test.
Efficacy analyses were performed with data from the intent-to-treat (ITT) and evaluable populations. The ITT population was used for all efficacy and safety analyses and included all patients who were randomized to treatment and who were administered at least 1 dose of study medication. For the ITT analysis, the last observation carried forward (LOCF) method was used to impute missing data. The evaluable cohort was used for the noninferiority test between active treatments and included patients from the ITT population who provided primary efficacy data on day 4 and who had no major protocol violations. For the evaluable cohort, the LOCF method was not used; subjects with missing observations were not evaluable for that visit.
Results
Patient Baseline Characteristics and Disposition
A total of 829 patients were enrolled in the study and were randomized to valdecoxib 20 mg twice a day with 40-mg loading dose (n = 233), valdecoxib 20 mg once a day with 40-mg loading dose (n = 235), tramadol 50 mg 4 times a day (n = 238), or placebo (n = 123). The study population was predominantly white with more male than female subjects. Although the inclusion criteria specified that patients should be aged 16 to 65 years, some exceptions were made. The exceptions were permitted on a case-by-case basis for requests, when in the investigators’ opinion the patient was otherwise a suitable candidate for the study. The age of patients enrolled ranged from 15 to 74 years, with the mean age between the 4 treatment arms ranging from 28.8 to 30.5 years. Baseline demographic and pretreatment injury characteristics were similar among the 4 treatment arms (Table 1). Most patients had an inversion injury (84%-87%) and a second-degree sprain (66%-72%) with severe pain (96%-98%). In 38% to 48% of patients, the ankle injury was sports related. The duration of the injury at the time of first dose was approximately 24 hours in all groups. The baseline pain VAS, Patient's and Physician's Global Assessments of Ankle Injury, and Patient's Assessment of Normal Function/Activity results were similar for the 4 treatment arms (Table 2). There was no significant difference between treatment groups in the use of rescue medication for ankle pain (Cochran-Mantel-Haenszel test, P = .333).
All randomized subjects received at least 1 dose of study medication and were, therefore, included in the ITT population. A total of 110 (13.3%) patients prematurely discontinued treatment (Figure 1). Although similar proportions of subjects discontinued treatment with valdecoxib 20 mg twice daily (10.7%), valdecoxib 20 mg once daily (11.1%), and placebo (9.8%), almost twice as many subjects (19.7%) discontinued treatment with tramadol 50 mg 4 times daily. This difference was largely due to a higher incidence of withdrawals for treatment-emergent adverse events in the tramadol treatment arm (described later).
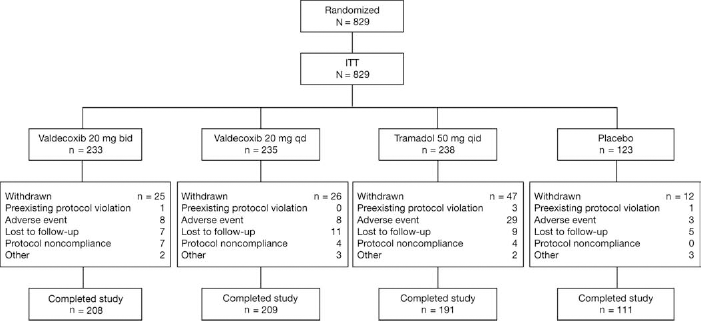
Patient disposition; ITT, intent to treat; bid, twice daily; qd, once daily; qid, 4 times daily.
The evaluable population, used to test for noninferiority between valdecoxib and tramadol for ankle pain VAS during weightbearing on day 4, consisted of 677 subjects treated with valdecoxib 20 mg twice daily (n = 203; 87.1%), valdecoxib 20 mg once daily (n = 206; 87.7%), tramadol 50 mg 4 times daily (n = 173; 72.7%), and placebo (n = 95; 77.2%). Patients were excluded from the evaluable population if there were any reasons that may have interfered with the primary efficacy assessment on day 4, and patients may have had more than 1 reason for exclusion, for example, acetaminophen use and use of prohibited medication on day 4. The most common reasons for exclusion from the evaluable population were unavailable pain VAS data on day 4 or use of acetaminophen. Other reasons were: preexisting protocol violation; lack of compliance with taking study medication; use of prohibited medication or analgesic agent on day 4; lost to follow-up; and not stable for 3 months on selective serotonin reuptake inhibitors.
Patient Demographics and Ankle Injury Characteristics at Baseline a
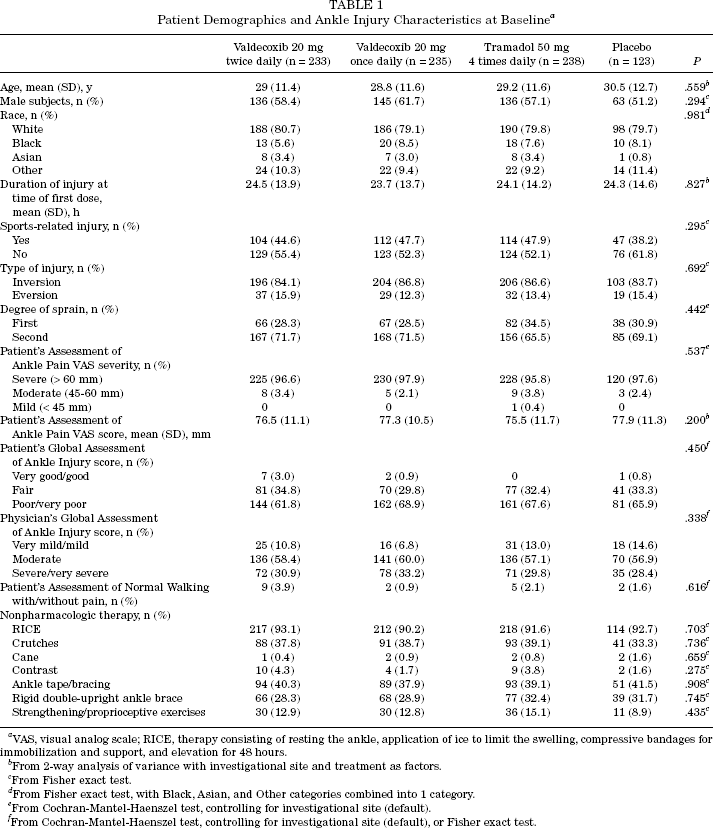
VAS, visual analog scale; RICE, therapy consisting of resting the ankle, application of ice to limit the swelling, compressive bandages for immobilization and support, and elevation for 48 hours.
From 2-way analysis of variance with investigational site and treatment as factors.
From Fisher exact test.
From Fisher exact test, with Black, Asian, and Other categories combined into 1 category.
From Cochran-Mantel-Haenszel test, controlling for investigational site (default).
From Cochran-Mantel-Haenszel test, controlling for investigational site (default), or Fisher exact test.
Summary of Outcome in the 4 Treatment Arms With Respect to Secondary Efficacy End Points (Intent-to-Treat Population) a
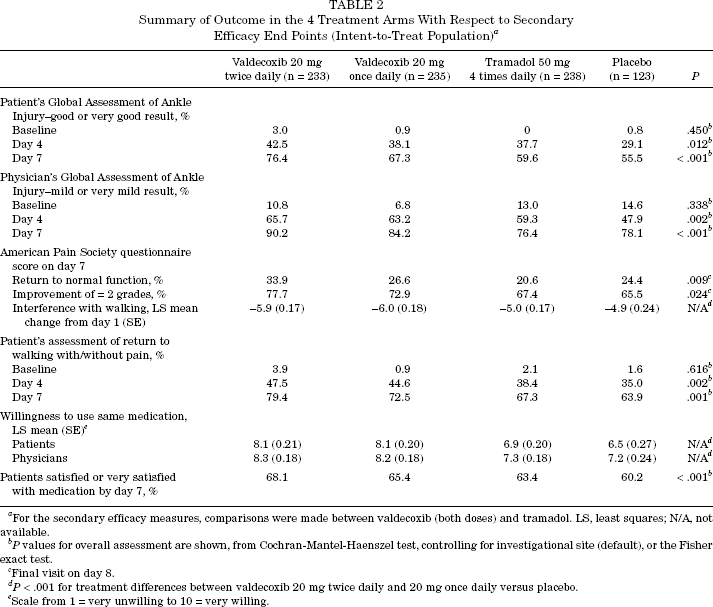
For the secondary efficacy measures, comparisons were made between valdecoxib (both doses) and tramadol. LS, least squares; N/A, not available.
P values for overall assessment are shown, from Cochran-Mantel-Haenszel test, controlling for investigational site (default), or the Fisher exact test.
Final visit on day 8.
P < .001 for treatment differences between valdecoxib 20 mg twice daily and 20 mg once daily versus placebo.
Scale from 1 = very unwilling to 10 = very willing.
Efficacy Analyses
In the evaluable patient cohort regarding ankle pain VAS results on day 4, both valdecoxib 20 mg twice daily and valdecoxib 20 mg once daily were comparable with tramadol 50 mg 4 times daily, based on a prespecified limit for the 95% CIs (upper limit, 1.98; prespecified limit for noninferiority, 10.0). The LS means for ankle pain VAS on day 4 were 27.1 for valdecoxib 20 mg twice daily, 29.0 for valdecoxib 20 mg once daily, and 31.0 for tramadol. The difference between the LS mean ± SE was –3.87 ± 2.00 (95% CI, –7.80 to 0.05) for valdecoxib 20 mg twice daily minus tramadol 50 mg 4 times daily and was –1.91 ± 1.98 (95% CI, –5.81 to 1.98) for valdecoxib 20 mg once daily minus tramadol 50 mg 4 times daily. Both valdecoxib doses significantly improved pain VAS scores compared with placebo in the evaluable cohort on day 4 (P < .001 with valdecoxib 20 mg twice daily; P = .008 with valdecoxib 20 mg once daily). In contrast, the difference between tramadol and placebo on day 4 was not statistically significant in the evaluable cohort (P = .071) (Figure 2).
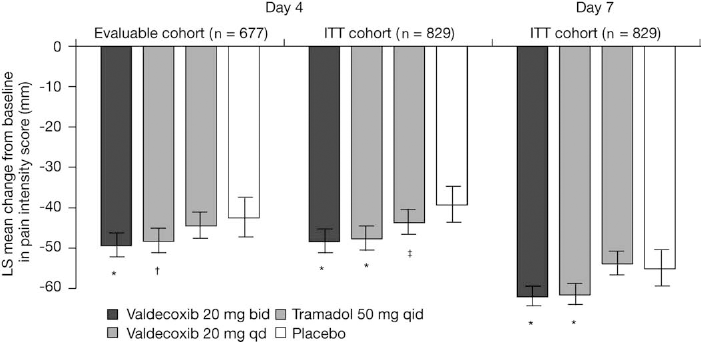
Patient's Assessment of Ankle Pain visual analog scale (VAS) score on weightbearing (least squares [LS] mean change from baseline, with error bars showing confidence intervals). The mean baseline score ranged from 75.5 to 77.9 mm. The means on days 4 and 7 are adjusted for baseline VAS score and investigational site; the baseline VAS score is adjusted for investigational site only. *P < .001; †P = .008; ‡P = .003; all P values versus placebo. ITT, intent to treat; bid, twice daily; qd, once daily; qid, 4 times daily.
Noninferiority between valdecoxib dosages and tramadol was confirmed in the ITT population by treatment differences on both day 4 (–3.67 ± 1.92 [95% CI, –7.44 to –0.09] for valdecoxib 20 mg twice daily minus tramadol; –2.19 ± 1.91 [95% CI, –5.95 to 1.56] for valdecoxib 20 mg once daily minus tramadol) and on day 7 (–7.16 ± 1.75 [95% CI, –10.6 to –3.74] for valdecoxib 20 mg twice daily minus tramadol; –5.94 ± 1.74 [95% CI, –9.35 to –2.53] for valdecoxib 20 mg once daily minus tramadol). In this population, valdecoxib 20 mg twice daily and once daily provided significant improvements versus placebo in pain VAS scores on days 4 and 7 (P < .001 for both groups). Tramadol significantly improved pain VAS scores versus placebo on day 4 (P = .003) but not on day 7 (P > .05). Analysis of other secondary efficacy end points further supported these findings, showing that valdecoxib was at least as effective as tramadol and superior to placebo (Table 2).
Treatment with valdecoxib was more effective than with placebo in enabling patients to resume normal walking with or without pain on days 4 and 7 of the study. Whereas 45% to 47% of valdecoxib-treated patients had resumed normal walking by day 4, only 35% of those treated with placebo and 38% of those treated with tramadol resumed normal walking by day 4. By day 7, 73% to 79% of valdecoxib-treated patients compared with only 64% of those on placebo and 67% of those on tramadol resumed normal walking. Both valdecoxib treatments significantly improved the APS scores for interference with walking ability versus placebo on days 3, 4, 5, 6, and 7 (P = .001) (day 7 results shown in Table 2).
Adverse Events With at Least 2% Incidence (Intent-to-Treat Population) a
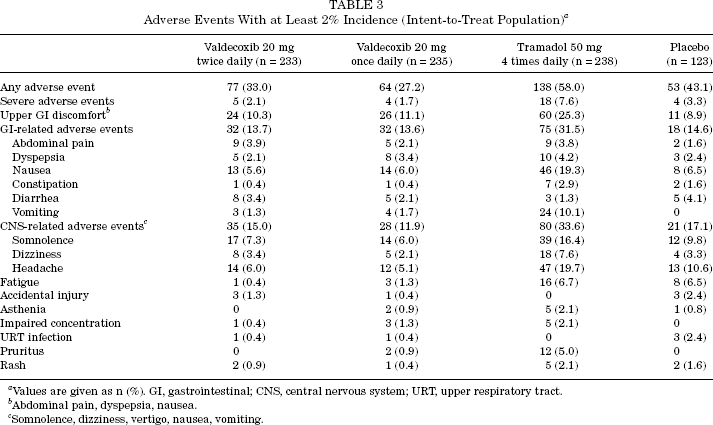
Values are given as n (%). GI, gastrointestinal; CNS, central nervous system; URT, upper respiratory tract.
Abdominal pain, dyspepsia, nausea.
Somnolence, dizziness, vertigo, nausea, vomiting.
A higher proportion of patients who took valdecoxib were satisfied or very satisfied with their medication (65%-68%) compared with those taking tramadol (63%) or placebo (60%) (P < .001) (Table 2). Furthermore, compared with placebo, significantly more valdecoxib-treated patients and their physicians expressed a willingness to use the same medication again (P < .001). In contrast, tramadol was similar to placebo with respect to patients’ and physicians’ willingness to use the medication again.
Safety Analyses
Adverse events occurred in 58% of patients receiving tramadol 50 mg 4 times daily, 27% to 33% of patients receiving valdecoxib 20 mg twice or once daily, and 43% of patients receiving placebo. Most adverse events reported in the study were mild to moderate in intensity. The incidence of severe adverse events was 7.6% in the tramadol group and 1.7% to 3.3% in patients receiving valdecoxib or placebo, respectively. No patient experienced a serious adverse event in this study.
Upper GI discomfort occurred in 25.3%, 10.3%, 11.1%, and 8.9% of patients in the tramadol, valdecoxib 20 mg twice daily, valdecoxib 20 mg once daily, and placebo treatment groups, respectively. The incidence of nausea was numerically higher (19%) in the tramadol treatment group compared with the other treatment groups (Table 3). Central nervous system-related adverse events (including moderate/severe somnolence, dizziness, vertigo, nausea, and vomiting) occurred in 33.6%, 15.0%, 11.9%, and 17.1% of patients in the tramadol, valdecoxib 20 mg twice daily, valdecoxib 20 mg once daily, and placebo treatment groups, respectively.
Tramadol treatment resulted in a 4-fold higher rate of withdrawals due to adverse events compared with valdecoxib treatment (12.2% vs 3.4%; P = .0005). The rates of withdrawals due to adverse events were similar in the valdecoxib and placebo groups (3.4% vs 2.4%; P = .75) (Figure 3).
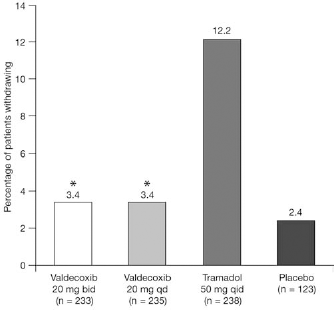
Incidence of withdrawals due to treatment-emergent adverse events. *P = .0005, valdecoxib versus tramadol and P = .75, valdecoxib versus placebo, based on the Fisher exact test for 2 × 2 tables; bid, twice daily; qd, once daily; qid, 4 times daily.
Discussion
This randomized, double-blind, placebo-controlled study showed that 7 days’ treatment with valdecoxib 20 mg either once or twice daily (both with a 40-mg loading dose) provided improvements that were significant versus placebo and at least as good as tramadol 50 mg 4 times daily in relieving the signs and symptoms of acute ankle sprain. On day 4, valdecoxib significantly reduced the patient's pain versus placebo and was comparable with tramadol; whereas on day 7, valdecoxib but not tramadol significantly reduced the patient's pain versus placebo. The tramadol group also had a numerically higher rate of adverse events, including upper GI-related and CNS-related events, and a significantly higher rate of withdrawals due to adverse events.
In the present study, the hypothesis of noninferiority was met between valdecoxib 20 mg twice or once daily and tramadol 50 mg 4 times daily for Patient's Assessment of Ankle Pain VAS scores on day 4 in the evaluable patient cohort. These findings were supported by the ITT population analyses, which showed that valdecoxib was significantly more effective than was placebo on both days 4 and 7 with respect to pain relief and other efficacy measures such as functional improvement and a return to normal activities. It was notable in this study that significantly more patients in the valdecoxib treatment arms had returned to normal walking within 4 to 7 days compared with placebo-treated patients and those on tramadol. An early return to normal activity is clearly beneficial, as it not only improves patient satisfaction with treatment but also enhances his or her ability to perform the functional rehabilitation needed for proper healing. Previous studies have shown that when used to augment standard nonpharmacologic treatment such as RICE, both nonspecific NSAIDs and COX-2 specific inhibitors can accelerate a return to normal function in patients with acute ankle sprain.14,45 For example, compared with the generally accepted recovery times of 8 days for grade I/mild sprain and approximately 15 days for grade II/moderate sprain with nonpharmacologic treatment, the average return time to normal activity was shortened with nonspecific NSAID treatment (6 days) and was further accelerated with COX-2 specific inhibitor therapy (5 days). 14
In addition to the importance of returning to normal function as early as possible, the safety and tolerability of adjunctive analgesic therapy is also a key consideration. Tramadol has often been used as an analgesic agent in preference to nonspecific NSAIDs, especially in patients already experiencing gastric problems. 29 However, tramadol is commonly associated with CNS-related adverse effects such as dizziness, nausea, dry mouth, and sedation, 30 which may limit its use for the treatment of ankle sprains as well as other conditions, especially in the ambulatory setting. In the present study, valdecoxib provided comparable analgesic efficacy to tramadol but was clearly better tolerated.
A total of 13.2% of patients discontinued prematurely from this study in the randomized population (Figure 1), with the highest proportion of patient discontinuations in the tramadol group (19%). This group, in which the highest percentage of patients suffered nausea (19.3%) (Table 3), also had the highest percentage of patients discontinue due to adverse events (3.5% compared with 0.96% for both valdecoxib groups) (Figure 1). Within all randomized patients, loss of patients because of noncompliance was 0.84% in the valdecoxib 20 mg twice daily group, followed by 0.48% in both the valdecoxib 20 mg once daily and tramadol groups (Figure 1). This study was sufficiently powered (93% power) to accommodate this discontinuation of patients, so the loss of patients did not affect the overall results.
Possible limitations of this study include the absence of dose titration for tramadol, which could have led to exaggerated adverse effects in some patients. Secondly, it is likely that more informative data could have been obtained by assessing the return-to-normal function before day 4 and between days 4 and 7.
Previous studies have shown that COX-2 specific inhibitors provide anti-inflammatory and analgesic efficacy that is comparable to nonspecific NSAIDs but with a reduction in the GI and platelet toxicity associated with nonspecific NSAIDs. ‡‡ The lack of adverse effects on platelet function is particularly important in patients with acute ankle sprain because bleeding, in addition to pain and inflammation, can be part of the injury condition. Hence, although an anti-inflammatory strategy employing nonspecific NSAIDs can be helpful, their adverse platelet effects might be detrimental. The use of a treatment that is platelet sparing may decrease volumetric changes in the ankle, further accelerating the patient's return to normal activity. 14
References 2, 3, 10, 14, 19, 26, 31, 33, 39, 41, 45.
A patient and physician preference for valdecoxib treatment over tramadol was observed in this study. Compared with tramadol-treated patients, a substantially higher proportion of patients taking valdecoxib were satisfied with their medication. Furthermore, a higher proportion of valdecoxib-treated patients and their physicians expressed a willingness to use the same medication again. These data suggest that the overall effectiveness of valdecoxib may be superior to that of tramadol.
The withdrawal of rofecoxib from the market sparked concerns regarding the cardiovascular safety of the COX-2 inhibitors. Because of this apprehension, regulatory agencies in both the United States and European Union reviewed the data for NSAIDs, including COX-2 inhibitors. Both committees decided that additional information was needed; however, they also concluded that these agents have a place in medical therapeutics. After the completion of this study, sales of valdecoxib were suspended in the United States, ostensibly because of higher reporting rates of rare but serious skin reactions than seen with other selective COX-2 inhibitors. 24
In conclusion, valdecoxib 20 mg twice daily or once daily (both with a 40-mg loading dose) was at least as effective as tramadol 50 mg 4 times daily and significantly better than placebo in providing pain relief in patients sustaining a first-degree or second-degree ankle sprain. In the evaluable population on day 4, valdecoxib but not tramadol provided significantly greater improvements in pain VAS results compared with placebo. Valdecoxib enabled more patients to resume normal walking on days 4 and 7 than did placebo or tramadol. In contrast, tramadol failed to distinguish itself from placebo in most efficacy analyses. Both valdecoxib and tramadol were well tolerated; however, a higher number of patients withdrew due to adverse events in the tramadol treatment group than in the valdecoxib treatment group. These findings confirm those of previous reports and indicate that COX-2 specific inhibitors, such as valdecoxib, provide safe and effective pain relief in the early treatment of ankle sprain. These agents appear to provide analgesic activity that is as effective as tramadol for this condition but with superior tolerability and safety profiles.