
Abstract
Background: Identification of mechanical factors associated with patellofemoral pain, the most prevalent running injury, is necessary to help in injury prevention, but unfortunately they remain elusive.
Hypothesis: Runners who develop patellofemoral pain have increased knee joint angular impulse in the frontal plane.
Study Design: Case control study; Level of evidence, 3.
Methods: A retrospective study compared knee abduction impulses of 20 patellofemoral pain patients with those of 20 asymptomatic patients. A second prospective study quantified knee angular impulses during the stance phase of running of 80 runners at the beginning of the summer running season. Epidemiologic data were then collected, recording the type and severity of injury of these runners during a 6-month running period.
Results: The patellofemoral pain patients in the retrospective study had significantly higher (P = .026) knee abduction impulses (17.0 ± 8.5 Nms) than did the asymptomatic patients (12.5 ± 5.5 Nms). Six patients developed patellofemoral pain during the prospective study. The prospective data showed that patients who developed patellofemoral pain had significantly higher (P = .042) knee abduction impulses (9.2 ± 3.7 Nms) than did matched patients who remained uninjured (4.7 ± 3.5 Nms).
Conclusion: The data indicate that increased knee abduction impulses should be deemed risk factors that play a role in the development of patellofemoral pain in runners.
Clinical Relevance: Footwear and running style can influence knee angular impulse, and the appropriate manipulation of these variables may play a preventive role for patients who are predisposed to patellofemoral pain.
Patellofemoral pain is a debilitating injury that has been reported as the most common athletic injury, affecting up to a quarter of all persons active in sporting activities.9,22 Patellofemoral pain is especially common in sports that involve running, occurring twice as frequently as the second most common running injury (iliotibial band friction syndrome or tibial stress syndrome, depending on the study).5,32 Patellofemoral pain is a chronic injury that can persist and affect athletic activity indefinitely. In fact, even with treatment, up to 75% of affected athletes must modify their athletic activity, as they continue to be plagued by pain for several years.3,20
Patellofemoral pain commonly develops on the lateral aspect of the patella.8,12 This finding suggests that frontal plane loading, in particular internal knee abduction moments, may play a large role in the development of patellofemoral pain in runners. Increased knee abduction moments during running could be generated by increased muscle forces, increased soft tissue forces, or a combination of the two. It has been suggested that increases in these forces overpower the vastus medialis, which acts as a medial stabilizer for the patella. 15 When this occurs, lateral tracking of the patella and increased lateral stress can occur. 6 Increases in values for these moments would, therefore, likely reflect as increases in loads and stresses on the lateral facet of the patella, which in turn can result in the activation of nociceptive (pain) fibers in the bone and/or synovium 11 and the development of patellofemoral pain.
Patellofemoral pain is typically classified as an overload or overuse injury, as large stresses are exacerbated by repetitive loading, leading to a cumulative effect.27,33 Because cumulative loading is best quantified with impulse variables, it was hypothesized that runners who develop patellofemoral pain have higher knee joint angular impulse in the frontal plane than do runners who do not develop patellofemoral pain. Abduction moments represent the torque or twisting loads on the knee in the frontal plane, and the impulse is the total twisting load experienced during the stance phase, calculated by multiplying the load with the length of time it is applied (Figure 1). The analysis of knee abduction impulse for patients with and without patellofemoral pain may provide information about biomechanical factors responsible for the onset of this pain. Furthermore, to truly assess this hypothesis and determine whether knee abduction moments are causally related to patellofemoral pain, a prospective study is required.
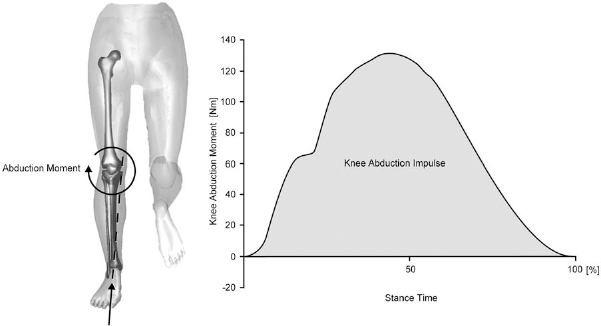
Schematic illustration showing the resultant knee abduction moment and the calculation of the knee abduction impulse during the stance phase of running. The knee abduction impulse (shaded region) represents the area under the moment-time curve.
Therefore, the purposes of this investigation were to determine (1) whether knee joint angular impulse in the frontal plane is associated with patellofemoral pain in runners with the use of a retrospective case control study and (2) whether knee joint angular impulse in the frontal plane is causally related to the onset of patellofemoral pain in a group of recreational runners with the use of a prospective study.
Methods
Retrospective Case Control Study
Two groups of runners were analyzed using a case control study design. These groups included the following:
Patellofemoral pain group (PFP group): group of patients with patellofemoral pain at time of study, with no other injuries to the lower extremity in the past 3 months.
Asymptomatic group (ASYMP group): group of patients who never had patellofemoral pain, with no other injuries to the lower extremity in the past 3 months.
Data were collected on 40 patients (PFP group, n = 20; ASYMP group, n = 20). The mean anthropometric data for the patients can be found in Table 1.
Patient Characteristics of the 40 Runners Who Participated in the Retrospective Study a
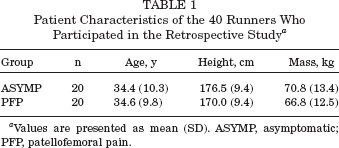
Values are presented as mean (SD). ASYMP, asymptomatic; PFP, patellofemoral pain.
Patellofemoral pain volunteers were recruited via medical records from a sports medicine clinic. Potential patients were contacted by telephone and asked whether they would be willing to participate. Asymptomatic volunteers were recruited through advertisements placed at local running shoe stores with organized running programs. Before the study, all volunteers read and signed a subject consent form approved by the university ethics committee. Entry criteria for the ASYMP group included having maintained a minimum weekly running distance of 20 km for at least the 6 months before the study. All patients were between 20 and 50 years old, had no injuries to the testing leg, had no prior knee surgery, and had no diagnosis of joint disease. Entry criteria for the patellofemoral pain patients included the above criteria plus their patellofemoral pain was not related to an acute injury but was overuse in nature. Proper diagnoses of the injured patients were performed by 1 of 2 sports medicine physicians (12 patients were diagnosed by 1 physician, whereas the remaining 8 were diagnosed by the other physician). Common symptoms and signs used to diagnose patellofemoral pain by the sports medicine physicians were pain on palpation of the medial or lateral border of the patella, pain on deep knee flexion (ie, deep knee bend, walking up or down stairs), and/or pain on the posterior surface of the patella when the quadriceps muscles were contracted with the knee in full extension. Patients were excluded if their knee pain was found to be related to patellar tendinitis, quadriceps tendinitis, or prepatellar bursitis.
Three-dimensional kinematics of the affected limb were quantified for the PFP group. For the ASYMP group, the left or right leg was randomly selected for analysis. The upper leg, the lower leg, and the foot segments were prepared using 9 reflective markers (3 per segment) attached to the skin with adhesive tape. The markers were attached at the following locations: proximal lateral upper leg, midanterior upper leg, distal lateral upper leg, proximal lateral lower leg, midtibial crest, distal lateral lower leg, posterior shoe heel, distal shoe heel, and the lateral side of the shoe below the lateral malleolus. The 3-dimensional spatial positions of the markers were collected using 4 electronically shuttered, high-speed video cameras (NAC MOS-TV, V-14B, Japan) equipped with 12.5- to 75-mm zoom lenses (Cosmicar, Japan) and a VP310 video processor (Motion Analysis Corp, Santa Rosa, Calif). The sampling frequency was set at 200 frames per second, and the exposure time was set at 1/2500 seconds. System calibration was achieved using a calibration frame containing 8 control points. The calibration volume closely matched the volume of interest. The raw data were stored on a SUN 3/280 computer.
Simultaneous 3-dimensional force data were collected using a force platform (Kistler AG, Winterthur, Switzerland) mounted flush with the floor in the center of a 30-m runway. Force data were sampled at 1000 Hz. Patients were given several practice trials to ensure that the foot landed with a natural running style on the force platform. In all of the cases, the natural running style was one of a heel-toe strategy. Running speed was controlled (4.0 ± 0.2 m/s) using 2 photocells, 1.9 m apart, at shoulder height.
Positions of the markers to establish the defined neutral position were identified in a standing trial using the video system (200 Hz, 2-second sample). The patient was asked to stand in a position with feet pointing anteriorly and approximately hip width apart. The knee and hip were in a fully extended position, with the ankle joint at approximately a 90° angle. Six markers were used to identify joint centers in the standing neutral trial. The hip joint center was identified by markers placed on the greater trochanter and on the anterior leg just below the anterior superior iliac spine, the knee joint center was identified by markers on the lateral knee and at the center of the patella, and the ankle joint center was identified by markers on the lateral malleolus and on the anterior talus. For each joint, the lateral marker defined the joint center's anterior-posterior and superior-inferior coordinates, and the anterior marker defined the joint center's mediolateral coordinate. This information was necessary to make a transformation file relating the marker-based coordinate system to a meaningful anatomical segmental coordinate system for the lower and upper leg using a singular value decomposition method. 31
Video data were processed using Expert Vision Three-Dimensional software (Motion Analysis Corp). A direct linear transformation was performed to determine 3-dimensional spatial coordinates of each marker from the 2-dimensional data collected. Data were tracked for a period corresponding to 10 frames before and after contact with the force plate. Before calculation, the kinematic data were smoothed using a second-order low-pass Butterworth filter with a cutoff frequency of 12 Hz, and the kinetic data were smoothed using a second-order low-pass Butterworth filter with a cutoff frequency of 100 Hz. Both the kinematic and kinetic data were imported into Kintrak 4.0 (Motion Analysis Corp) for further analysis.
Three-dimensional joint attitude and angular motions were determined using a joint coordinate system implemented in Kintrak 4.0. This joint coordinate system consisted of the proximal segment's (thigh segment for the knee joint calculations) flexion-extension axis, the distal segment's (shank segment for the knee joint calculations) longitudinal axis, and a third “floating” axis calculated as the cross-product of the flexion-extension and longitudinal axes. Knee joint kinematics (3-dimensional) was calculated for the period of stance as the relative movement of the lower leg with respect to the upper leg. Resultant joint moments in the frontal plane were calculated about the floating axis for the stance phase of running in Kintrak using a standard inverse dynamics approach. Abduction moments represent the torque or twisting loads on the knee in the frontal plane. Internal abduction impulse was quantified by integrating the moment-time curve and represents the cumulative twisting load during the entire stance phase. Means were calculated for 5 trials per patient. A 1-tailed t test was used to compare the knee abduction impulse between the injured and uninjured patients with a level of significance set at α =. 05.
Prospective Study
The data collected in this investigation consisted of 2 parts. The first aspect was a detailed kinematic and kinetic analysis during the stance phase of running for 140 runners at the beginning of the summer running season. The second aspect was an epidemiologic study quantifying the type and severity of injury of these runners as they undertook a 6-month running period. As the patients constituted a relatively experienced group of runners, 89% reported at least 1 previous running-related injury. However, all runners were free from pain or injury at the onset of the study. Eighty patients (Table 2) fully completed the study with detailed running logs and injury data after the 6-month period. Informed written consent in agreement with the university ethics committee's policy was obtained from all patients.
Patient Characteristics of the 80 Runners Who Completed the Prospective Investigation a
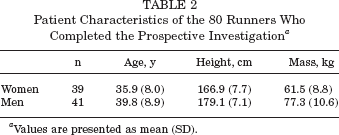
Values are presented as mean (SD).
Using similar methodology as in the retrospective case control study, force and movement data were collected in the laboratory at a running speed of 4.0 ± 0.2 m/s. Although training paces of the patients varied, all patients were comfortable at this pace. One small modification was made to the data collection protocol for the prospective study. The knee joint center was calculated as the midpoint between markers placed on the lateral and medial epicondyles, as opposed to on the patella. This change was made in conjunction with newly presented data from Ferber et al, 10 showing that knee abduction moments are highly repeatable using this methodology. All patients had data collected on both right and left legs while wearing their own running shoes. Internal abduction impulse was quantified by integrating the moment-time curve, and means were calculated for 3 trials per patient.
After completion of the kinematic and kinetic data collection, patients began a 6-month running period (approximately May-October, depending on the patient). During the running period, patients were required to document daily running distance and intensity in a log book that was collected monthly. Any lower extremity pain or injury that was thought to be running related was documented in the log book. Although the patients did not meet regularly with the investigators, they were encouraged to contact the investigators if they had any questions. Moreover, a weekly injury clinic was organized at which 2 sports medicine physicians were available to assess injuries requiring medical attention.
During the study, 6 patients who were seen by the physicians were diagnosed with patellofemoral pain. None of the 6 patients previously had patellofemoral pain. Diagnosis of patellofemoral pain was based on meeting all of the following historical and physical examination criteria:
History
Nontraumatic unilateral and/or bilateral peripatellar or retropatellar knee pain
Patellofemoral knee pain with and/or after activity
Inactivity patellofemoral pain and/or stiffness, especially with sitting with knees held in flexed posture
No history of knee surgery
Physical examination
No or minimal articular or periarticular effusion or bursitis
No significant joint line tenderness
No intra-articular ligamentous instability
Peripatellar tenderness ± mild inferior patellar pole tenderness
No patellar apprehension
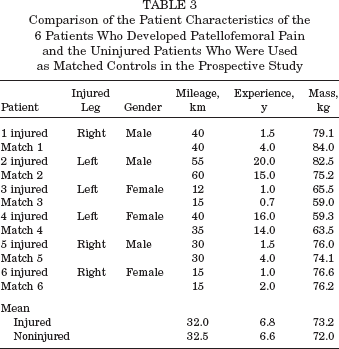
To analyze the knee joint impulses of the injured (PFP group) patients, 2 different analyses were performed. The first analysis compared the 6 injured patients to the 74 patients who did not develop patellofemoral pain. This analysis is confounded by the fact that some of the patients who did not develop patellofemoral pain during this study (1) had a previous history of patellofemoral pain and/or (2) developed other running injuries such as iliotibial band syndrome or tibial stress syndrome. Therefore, a second analysis was performed in which the 6 injured patients were matched to 6 patients who remained injury free (ASYMP group) throughout the study, 1-to-1 case-to-control matching. Patients were matched according to weekly training distance, years of running experience, mass, and gender (Table 3), variables that have been proposed to be associated with injury and/or that can have an influence on resultant joint moments.25,34 All matching was performed solely on the variables listed, with the researchers blinded to the outcome variables. None of the 6 asymptomatic patients had a previous patellofemoral injury. For both comparisons, a 1-tailed paired t test was used to compare the knee abduction impulse between the injured and uninjured patients. The level of significance was set at α =. 05.
Comparison of the Patient Characteristics of the 6 Patients Who Developed Patellofemoral Pain and the Uninjured Patients Who Were Used as Matched Controls in the Prospective Study
Results
Retrospective Case Control Study
Resultant knee joint moments in the frontal plane were primarily abduction throughout the stance phase. The mean resultant knee abduction moments showed similar patterns but different magnitudes for the PFP and ASYMP groups (Figure 2). The PFP group patients had significantly higher (P =. 026) knee abduction impulses (17.0 ± 8.5 Nms) than did the ASYMP patients (12.5 ± 5.5 Nms) (Figure 3).
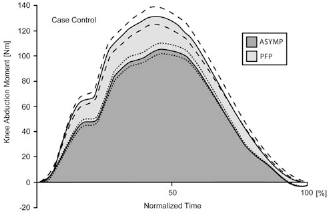
Mean (SE) resultant knee abduction moments for the 20 patellofemoral pain (PFP) and 20 asymptomatic (ASYMP) patients. The shaded regions represent the knee abduction impulses.
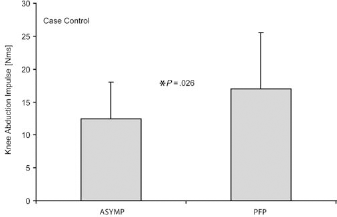
Mean (SD) knee abduction impulses for the 20 patellofemoral pain (PFP) and 20 asymptomatic (ASYMP) patients.
Individual results for the knee joint impulses are presented in Figure 4. Individual values for each PFP group patient are compared with the mean knee abduction impulse of the ASYMP group. There is an approximately equal distribution of PFP group patients who had knee abduction impulses higher and lower than the mean of the ASYMP group. However, 10 of 20 patients had more than 50% larger abduction impulses compared to the ASYMP group, with 6 patients having impulses that were more than 100% larger. In contrast, only 1 patient within the ASYMP group had more than a 50% larger impulse than the ASYMP group mean.
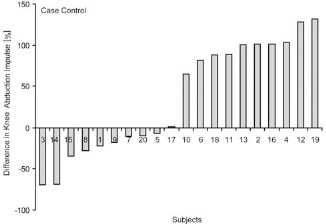
Knee abduction impulse for the patellofemoral pain (PFP) patients. Comparison is made to the asymptomatic (ASYMP) patients where zero represents the mean of the ASYMP group. A positive value indicates the PFP patient had knee abduction impulses that were higher than the mean of the ASYMP group.
Prospective Study
Six patients (3 men and 3 women) were clinically diagnosed with patellofemoral pain. The mean resultant knee joint moments during running showed similar patterns (Figure 5) to the retrospective study. There was no significant difference (P =. 230) in knee abduction impulses when comparing the PFP group patients (9.2 ± 3.7 Nms) to all the other patients who did not develop patellofemoral pain (7.7 ± 4.8 Nms) (Figure 6). When matched according to running mileage, running experience, gender, and mass, the PFP group patients had significantly higher (P =. 042) knee abduction impulses (9.2 ± 3.7 Nms) than did the matched ASYMP patients (4.7 ± 3.5 Nms) (Figure 7). Individual results for the knee joint moments are presented in Figure 8. Five of the 6 patellofemoral pain patients had higher knee abduction impulses than did their asymptomatic matched controls.
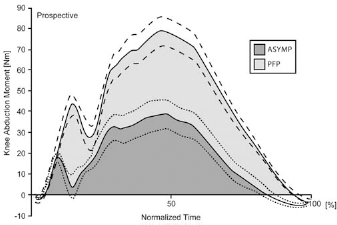
Mean (SE) resultant knee abduction moments for the 6 patients who developed patellofemoral pain (PFP) and the 6 asymptomatic matched controls (ASYMP). The shaded regions represent the knee abduction impulses.
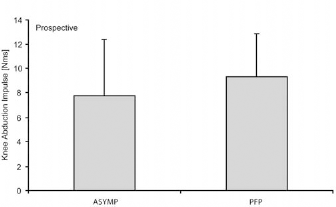
Mean (SD) knee abduction impulses for the 6 patients who developed patellofemoral pain (PFP) and the 74 patients who did not develop PFP. ASYMP, asymptomatic.
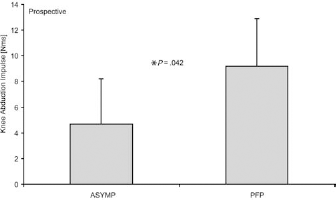
Mean (SD) knee abduction impulses for the 6 patients who developed patellofemoral pain (PFP) and the 6 asymptomatic matched controls (ASYMP).
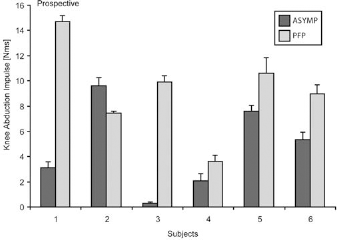
Mean (SD) knee abduction impulse for each of the 6 patients who developed patellofemoral pain (PFP) in comparison to their asymptomatic matched controls (ASYMP).
Discussion
The first purpose of this investigation was to determine whether knee angular impulses in the frontal plane are associated with patellofemoral pain. The data from the retrospective case control study showed that abduction impulses are related to patellofemoral pain, as mean knee abduction moments in the PFP group were significantly higher than those in the ASYMP group by 36%. The second purpose was to determine whether these abduction impulses are causally related to the onset of patellofemoral pain. In the prospective study, the patients who developed patellofemoral pain had knee abduction impulses that were, on average, 19% higher than those in the remaining runners who did not develop patellofemoral pain. These differences were not significantly different; however, they were confounded by various factors. The main confounding factor was that some of the patients, although currently uninjured, had a history of patellofemoral pain. Another confounding factor was that some of these patients developed other running injuries such as iliotibial band syndrome or tibial stress syndrome. It may be that these runners modified their training programs or running styles as a result of these injuries, thus preventing the onset of patellofemoral pain. Consequently, an attempt was made to compare the patients with patellofemoral pain in the prospective study to similar (matched on the basis of gender, running mileage, running experience, and mass) uninjured patients. Research has shown that joint moments are influenced by mass and gender 25 ; thus, it was important to match for these criteria. Furthermore, injury has been related to weekly running distance and years of running experience 34 ; thus, it was deemed necessary to match for these criteria as well. The prospective data show that the patients who developed patellofemoral pain had significantly higher (97%) knee abduction impulses before injury than did uninjured matched controls. Thus, the hypothesis that runners characterized by increased knee abduction impulses are predisposed to patellofemoral pain was supported. The data from these 2 studies indicate that knee abduction impulses should be deemed risk factors that play a role in the development of patellofemoral pain in runners.
Although several studies1,16,17 have quantified patellofemoral loads and pressures in vitro, it is obviously difficult to determine these parameters in vivo. Therefore, resultant knee joint moments have been used to look at in vivo patellofemoral joint loading. Scott and Winter 29 studied internal forces at the knee joint during running. They used knee joint moments as inputs into a 2-dimensional sagittal plane model to calculate patellofemoral joint contact force over the stance phase of running. Mean patellofemoral joint contact forces equated to 7.6 times body weight. Other authors have also indicated that these patellofemoral forces can be several times body weight18,28 and have, therefore, speculated that this large force substantiates why this joint has such a high injury frequency rate. Recently, Powers et al 26 showed that increases in knee extensor moments lead to increases in contact forces and stress in the patellofemoral joint. However, extensor moments account for only part of the joint loading. Glitsch and Baumann 14 found that for patients running at 5 m/s, moments in the frontal plane contributed significantly to the 3-dimensional intersegmental knee joint moment. Initial foot placement during running necessitates the hip being in an adducted position during the stance phase. Consequently, the positioning of the ground-reaction force results in an external adduction moment at the knee, which can be quite large, up to 50% of the knee extension moments, 21 and must be counteracted by an internal abduction moment. A comparison with a 2-dimensional approach showed that there was an underestimation of the internal loads by up to 60%, suggesting that a 3-dimensional approach including frontal and transverse plane moments should be used to get a clear picture of the loads acting on the knee joint.
Frontal plane knee moments have been linked to disorders other than patellofemoral pain. A study done by Andriacchi 2 showed that a higher than normal abduction moment at the knee joint may be related to progressive degenerative changes at the knee joint. It was suggested that this factor may influence surgical outcome in patients treated for varus deformities. Hurwitz et al 19 found that the abduction moment during walking was the single best predictor of knee joint bone mineral content measured by radiograph absorptiometry. This finding suggests that an increase in value for this moment may equate to an increase in load and may have important implications for the progression of degenerative joint disease. It has also been shown 30 that there was a significant relationship between abduction moments and severity of osteoarthritis.
Knee joint moments and impulses in the frontal plane can be influenced by footwear and running style. Different authors have shown that medially or laterally wedging footwear can influence peak knee moments in the frontal plane. Inverted orthotics posted between 15° and 25° significantly increase peak knee abduction moments during running. 36 Medial wedges of 10° were also found to significantly increase peak knee abduction moments during walking. 35 In contrast, lateral wedges significantly reduced peak knee abduction moments7,35 with wedges as small as 5°. Running mechanics such as hip adduction will also influence the knee abduction moment. Greater hip adduction will result in increased knee joint moments as the lever arm between the line of action of the ground-reaction force and the knee joint center increases (Figure 9). In addition, foot contact position and angle can influence the point of application of the ground-reaction force and, subsequently, the knee joint moment. It appears that even relatively small changes in footwear and running mechanics can have significant influences on knee loading in the frontal plane.
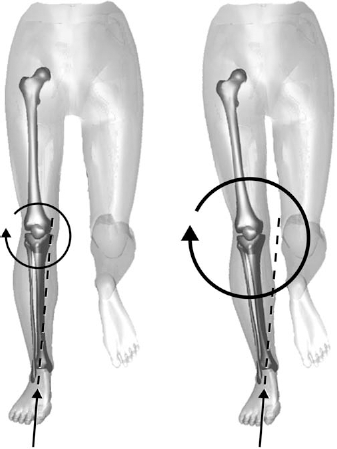
Schematic illustration showing how increased hip adduction (right) results in increased knee abduction moments with identical ground reaction forces.
Limitations and errors associated with determining resultant joint moments have been well documented.4,23 However, Ferber et al 10 showed knee abduction moments to be highly repeatable with within-day and between-day interclass correlation coefficients of 0.98. Despite the use of slightly different methods, the resultant knee joint moments found in this investigation showed similar patterns and peak magnitudes to those previously reported. 24 There were some discrepancies in the absolute magnitudes of the abduction impulses between the retrospective and prospective studies. These discrepancies can be primarily attributed to different methods of selecting the knee joint centers, as discussed in the “Methods” section; however, this does not affect the repeatability of the measurements. A main limitation of this investigation was the small group of injured patients in the prospective study. Six of 80 patients (those who completed the study) developed patellofemoral pain during a 6-month period for an annual injury incidence of 15%. This finding was slightly lower than the reported values of 16% to 25%.5,32 Another limitation is that patellar loading was not directly quantified. To fully understand the cause of patellofemoral pain, it is important to directly quantify the loading of the patellofemoral joint. However, this procedure is extremely invasive and is difficult to perform in vivo. Thus, the exact mechanical link between increased frontal plane knee joint angular impulse and patellofemoral pain cannot be conclusively defined. However, the results indicate that knee joint abduction impulse may be a useful predictor of persons who may be predisposed to developing patellofemoral pain during running.
In conclusion, despite a substantial amount of research on patellofemoral pain during the past 25 years, it still remains the number one running injury, 32 suggesting that little progress has been made in prevention. Prevention is obviously difficult if the risk factors remain unknown. Runners who have patellofemoral pain have significantly higher knee abduction impulses than do asymptomatic runners. Furthermore, runners who developed patellofemoral pain during a 6-month running season had higher knee abduction impulses than did patients with similar characteristics who remained uninjured. The increased knee joint loading, as indicated by the increased joint impulses, may result in higher local stresses and, therefore, pain after repetitive cycles. Footwear and running style can have a substantial influence on the knee joint moments, and the appropriate manipulation of these variables may play a preventive role for patients who are predisposed to injury.