
Abstract
Background: Ulnar collateral ligament injury is most common in the overhead-throwing athlete. Jobe et al published the first report of ulnar collateral ligament reconstruction in throwing athletes with a 62.5% success rate. Recently, Altchek developed a new docking technique for reconstruction of the ulnar collateral ligament. The authors report the first series using a further modification of the docking technique using a 4-strand palmaris longus graft for reconstruction of the ulnar collateral ligament.
Hypothesis: The modified docking technique yields a high rate of successful return to preinjury level of competition in elite baseball players.
Study Design: Case series; Level of evidence, 4.
Methods: The authors retrospectively reviewed 25 elite professional or scholarship collegiate baseball players who underwent elbow ulnar collateral ligament reconstruction using the modified docking procedure with a minimum 2-year follow-up.
Results: Twenty-three of 25 (92%) were able to return to their preinjury levels of competition. The mean time to return was 11.5 months (range, 10-16 months). Complications included 1 transient postoperative ulnar nerve neurapraxia and 1 stress fracture of the ulnar bone bridge that occurred at 14 months postoperatively, after a full return to pitching.
Conclusion: The modified docking technique yields highly successful return to preinjury level of competition rates (92%) in a select group of elite baseball players.
The primary restraint to valgus force at the elbow is the anterior bundle of the anterior band of the ulnar collateral ligament (UCL).14–17 During throwing, the anterior bundle is subjected to high tensile loads as a result of the extreme valgus stress placed on the elbow during the throwing motion. The initiation of valgus load on the elbow coincides with the initiation of the acceleration phase of the throwing motion. In the 30 to 40 milliseconds from the initiation of the acceleration phase to the time of ball release, the elbow rapidly extends and achieves a mean angular velocity of 2300 deg/s.4,5,7,8,23 The resulting valgus force produces tensile forces of up to 290 N concentrated on the medial elbow. The estimated static tensile force placed on the UCL during pitching has been estimated at 35 N, whereas the ultimate tensile strength has been reported to be only 33 N.8–10,12,18,20 Although a portion of the medial tensile forces is likely resisted by the medial flexor-pronator muscles and the osseous anatomy of the elbow joint, it is clear that the UCL is subjected to repetitive high tensile loads. With such high repetitive tensile loads, it is easy to understand why pitchers most commonly suffer injury to this ligament.
Jobe et al 13 published the first report of UCL reconstruction in throwing athletes. The “Tommy John procedure” used the palmaris longus tendon as an autograft for reconstruction of the UCL. This original technique involved detachment of the flexor-pronator muscles at their origin with obligatory submuscular transposition of the ulnar nerve. It resulted in a 62.5% success rate as defined by return to preinjury level of sports participation but had a 31.25% complication rate related primarily to the ulnar nerve. Since that report, Thompson et al 22 reported improved success and fewer complications using a modified technique employing a muscle-splitting approach without obligatory transposition of the ulnar nerve. Numerous other authors have reported similarly successful results using various modifications of the initial Jobe technique.1–3 More recently, Rohrbough et al 19 reported a new technique for reconstruction of the UCL. Using this modified technique, called the docking technique, the authors reported that 33 of 36 throwing athletes were able to return to preinjury levels of sports participation by 2 years after surgery.
Since 1998, the authors have been using a further modification of the docking technique using a 4-strand palmaris longus graft for reconstruction of the UCL. The purpose of this study was to evaluate the results of this modified docking technique in a group of elite professional and collegiate baseball players.
Materials and Methods
Between January 1998 and January 2000, 25 elite male baseball players underwent UCL reconstruction performed by one of the authors (G.A.P.). Twenty were professional players, of which 19 were pitchers and 1 was a catcher. One professional played at the major league level and 19 played at the minor league level. Of those who played at the minor league level, 3 played at AAA level, 6 played at AA level, 7 played at A level, and 3 played for independent league professional teams. The remaining 5 were Division I scholarship collegiate pitchers. High school and amateur throwers were excluded. The mean age was 24.5 years, with a range of 19 to 27 years. The dominant extremity was involved in all cases. There were 20 right-handed pitchers and 5 left-handed pitchers. Nine (36%) reported a distinct injury with sudden onset of symptoms after a single pitch or throw. The remaining 16 (64%) recalled no distinct injury but rather described gradual onset of progressive medial elbow pain and associated decreased pitching performance. All players reported an inability to continue to pitch secondary to pain or diminished pitching performance, including loss of velocity and/or control. Three (12%) patients underwent surgery within 2 weeks of injury or diagnosis. Eight (32%) underwent surgery within 2 to 6 weeks of injury or diagnosis. The remaining 14 (56%) underwent surgery more than 6 weeks after initial injury or diagnosis. The mean time to surgery in this delayed group was 14 weeks. Only 2 patients had undergone previous surgery on the affected elbow. One player with chronic symptoms had undergone previous isolated ulnar nerve transposition 2 years earlier. One player with acute injury had undergone arthroscopy with posteromedial osteophyte excision for valgus extension overload 1 year earlier.
All players underwent a thorough history and physical examination. History included information regarding duration of symptoms (acute or chronic injury), pitch type thrown at time of injury, correlation of symptoms with phase of throwing and pitch type, and the player's perception of pitching performance since onset of symptoms. Physical examination included inspection, palpation, and determination of elbow range of motion for both extremities, valgus stress testing at 30° and 90°, flexor-pronator and extensor-supinator muscle groups examination, complete neurovascular examination with special attention to ulnar nerve function, and evaluation for the presence of a palmaris longus tendon.
Standard radiographs were performed on all patients and included AP, lateral, oblique, and radiocapitellar views. Anteroposterior maximum manual valgus stress radiographs were performed on both the involved and uninvolved elbows by a single examiner (G.A.P.) in all cases. Standardized mechanical valgus stress views were not performed because of the unavailability of a fixed arm-holder device. All patients underwent a gadolinium-enhanced MR arthrogram of the elbow using a 1.5-T scanner and dedicated elbow coil with 3-mm coronal sections through the UCL.
Indications for early surgery (within 6 weeks of initial presentation) included a complete tear of the anterior band of the UCL as demonstrated by leakage of gadolinium on MRI scan or by more than 2 mm of relative valgus laxity of the throwing elbow as demonstrated on stress radiographs. Athletes with partial tears without significant valgus laxity were initially treated nonoperatively with a minimum of 6 weeks of rest, avoidance of throwing, nonsteroidal antiinflammatory drugs, and physical therapy. The indications for surgical reconstruction in those athletes with partial tears without significant valgus laxity were persistent positive laxity or pain with a valgus stress test at 6 weeks after injury or an inability to return to pain-free throwing after a minimum of 12 weeks of nonsurgical treatment. The mean time to surgery for this group was 14 weeks.
The technique used was a modification of the docking technique described by Rohrbough et al. 19 A quadruple-stranded palmaris longus graft was used instead of a double-stranded palmaris graft. The contralateral palmaris longus tendon was the graft of choice when available to avoid additional surgical risk to the dominant arm and was used in 21 of 25 cases. The ipsilateral palmaris longus was the second preference and was used in 2 of 25 cases. The gracilis tendon was used when a palmaris tendon was not available; it was used in 2 of 25 cases. In those patients in whom a gracilis tendon was selected as graft choice, a double-looped gracilis tendon graft was used.
Arthroscopy was performed only in cases with clear indications for the procedure such as intra-articular loose bodies or large posteromedial osteophytes. Arthroscopy was performed in 6 of 25 cases in standard fashion. An arthroscopic valgus stress test, such as that described by Field and Altchek, 6 was performed and had a positive result in 4 of 6 cases. Subcutaneous transposition was required in 2 cases in which the ulnar nerve was hypermobile or subluxating as described by Azar et al. 2
The ulnar tunnel was prepared by subperiosteally exposing the posterior ulna with careful protection of the ulnar nerve. A 3-mm bur on a 90° dental drill was used to create bone tunnels anterior and posterior to the sublime tubercle. Care was taken to preserve a 10- to 15-mm bone bridge between the anterior and posterior holes. A No. 1 Ethibond Excel OS-2 needle (Ethicon Inc, Johnson & Johnson, Somerville, NJ) was used to pass a looped 2-0 nonabsorbable suture with the looped side exiting the anterior tunnel. The humeral tunnel was positioned in the central 2 quartiles or 50% of the medial epicondyle in the anterior position of the existing UCL. A 4- or 5-mm bur (selected based on the size of the palmaris tendon graft) on a straight microdrill was used to create a tunnel to a depth of 25 mm. Care was taken to preserve the anterior and posterior cortices of the medial epicondyle. The anterior portion of the upper border of the medial epicondyle was exposed using a muscle split just anterior to the intermuscular septum. A 2-mm bur on the 90° dental drill was then used to create 2 small tunnels that connected with the main humeral tunnel in a Y-like shape. These 2 small tunnels were separated by a 10-mm bone bridge. The looped end of the doubled palmaris was passed initially through the ulnar tunnel from anterior to posterior (Figure 1). In the case of a gracilis graft, 1 free end of the graft was prepared by placing a No. 1 braided nonabsorbable suture in a Krackow fashion. The Krackow suture was then passed through the ulnar tunnel and used to pull the free end of the graft through. The elbow was reduced with varus force, and the underlying native UCL was imbricated using No. 0 Panacryl suture. The looped end of the palmaris graft was then prepared by placing a No. 1 braided nonabsorbable suture in a Krackow fashion. The free ends of the Krackow suture were then passed through 1 of the small Y limb drill holes using the previously placed looped suture (Figure 1). The end of the graft was then pulled into the humeral tunnel and securely “docked” completely within it. The graft was tensioned and the elbow put through a full range of motion to eliminate potential creep in the graft. The final length of the graft was determined by placing the undocked free limb of the graft adjacent to the humeral tunnel. The length of the graft was trimmed after estimating adequate length to allow 10 mm of the free end to enter the mouth of the humeral tunnel. This point was marked, and a No. 1 braided nonabsorbable suture was placed in the free end in a Krackow fashion. The remainder of the free end of the graft distal to the ink mark was amputated. The free end of the graft was then docked securely in the humeral tunnel with the Krackow suture exiting the second of the small Y limb tunnels. Both limbs of the graft were then tensioned so that 15 to 17.5 mm of each limb was docked within the humeral tunnel (Figure 2). Final tensioning was performed with the elbow reduced with varus, the forearm in neutral rotation, and the elbow flexed at 45°. The graft was tensioned, and the 2 sets of sutures exiting the proximal humeral tunnels were tied over the bone bridge.
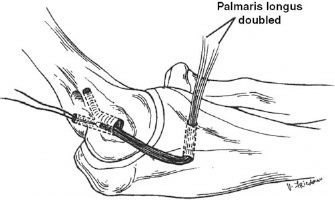
The looped end of the doubled palmaris longus tendon has been passed from anterior to posterior through the ulnar tunnel and docked in the humeral tunnel with the sutures exiting 1 of the small Y limb tunnels.
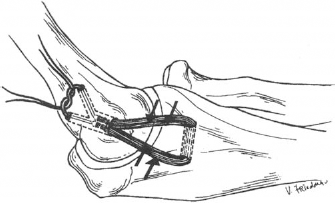
The free limb of the palmaris graft has now been docked in the humeral tunnel. The graft is tensioned, and the sutures are tied over the proximal bone bridge.
The elbow was maintained in the initial postoperative splint with the elbow at 80° of flexion and the forearm in neutral rotation for 10 to 14 days. After the splint was removed, the elbow was placed in a hinged brace, which was worn at all times except during supervised physical therapy. Range of motion was initiated immediately on removal of the initial postoperative splint. The brace was set to allow 30° to 90° range of motion for postoperative weeks 2 to 4 and 15° to 105° for postoperative weeks 4 to 6.
At 6 weeks after surgery, the brace was discontinued. Restoration of full range of motion was emphasized. Gradual forearm and shoulder strengthening was begun with avoidance of valgus stress at the elbow. At 12 weeks after surgery, increased strengthening was instituted with gradual progression of valgus stress on the elbow. The athlete was allowed to begin rehabilitation in the 90° of external rotation/90° of abduction position, including manual isometric and isotonic strengthening exercises and gentle throwbacks in preparation for a return to throwing.
At 16 weeks after surgery, a formal progressive return to throwing program was instituted. At 7 months after surgery, pitchers began throwing from the mound with an anticipated return to competitive throwing at 10 months after surgery.
Results
All 25 players were available for follow-up at a mean of 30 months and a minimum of 24 months after surgery. Twenty-three of 25 (92%) returned to their preinjury levels of competition or to higher levels (defined as still throwing at the same or a higher level at the time of minimum 2-year follow-up). The mean time to return to competitive throwing was 11.5 months (range, 9–16 months). There was no difference in time to return to play between the professional and collegiate players.
All 20 professional players had a good outcome, but only 19 of 20 returned to preinjury levels of competition or higher. One player was released by his team before completing his rehabilitation and decided to retire without returning to play. At the time of follow-up, he had a stable, pain-free elbow and was playing recreational baseball without limitation. Four of 5 collegiate players returned to preinjury levels of competition. One player was unable to return to competitive pitching because of persistent medial elbow pain with pitching. He had no evidence of valgus laxity; however, sequential plain radiographs demonstrated progressive widening of the ulnar bone tunnel without evidence of fracture.
The mean preoperative range of motion was 8° to 138°. The range of preoperative loss of flexion was 0° to 40°. Twenty-three of 25 (92%) had tenderness medially in the region of the UCL. Only 4 of 25 (16%) had clearly detectable valgus laxity on preoperative clinical valgus stress testing. Twenty of 25 (80%) had a positive milking maneuver sign. Two of 25 (8%) had preoperative sensory changes in the ulnar nerve distribution, but none had ulnar nerve motor dysfunction. The Tinel sign was positive at the cubital tunnel in 8 (32%) patients. Flexor-pronator provocative tests had positive results in 7 (28%) patients. A palmaris longus tendon was present in 22 (88%). The contralateral palmaris was present in 21 of 22, whereas 1 player had only an ipsilateral palmaris longus tendon present. Of the 9 who recalled acute onset of symptoms with a single pitch, 4 recalled throwing a curveball, 3 recalled throwing a fastball, and 2 recalled throwing a slider.
Plain radiographs demonstrated findings common to the thrower's elbow, including posteromedial osteophyte formation. One patient had obvious loose bodies. There were no avulsion fractures. Maximum manual stress radiographs were positive with more than 2 mm relative valgus laxity in 9 (36%) patients. The MR arthrogram was positive for either complete or partial tears in all patients. Five of 25 (20%) had complete tears with extra-articular leakage of the gadolinium. All others had evidence of a partial tear.
Postoperative range of motion averaged 5° to 132° (range, –5° to 138°). The range of postoperative flexion contracture was 0° to 15°. Valgus stress radiographs at 24 months after surgery demonstrated no player with more than 1 mm of relative valgus laxity versus the nonthrowing elbow. Complications included 1 transient postoperative ulnar nerve sensory neurapraxia, which resolved within 6 weeks, and 1 stress fracture of the ulnar bone bridge, which occurred at 14 months after surgery after a full return to pitching. No patients reported complications related to graft harvest site. No patients required reoperation. The player with the ulnar bridge stress fracture was a collegiate pitcher who had returned to pitching 12 months after surgery. He developed symptoms at 14 months after surgery after having pitched successfully for 2 months. He was treated with 3 months of rest and use of an ultrasound bone stimulator. The stress fracture healed, and he has subsequently returned to pitching without recurrence of the stress fracture.
Discussion
Ulnar collateral ligament injury is most common in the overhead-throwing athlete. Baseball pitchers experience the highest incidence of this injury. Although partial injuries may be managed nonoperatively, frequently complete tears with demonstrable valgus laxity require surgical reconstruction to return to overhead activities. Elbow UCL reconstruction results in significant interruption of a player's career progression with a mean recovery time of 12 to 16 months. In the past 25 years, reconstruction techniques have made successful return to preinjury levels of competition more likely, thereby converting this from a career-ending injury to a career-threatening injury.
Isolated repair of the UCL has yielded poor results, with previous studies reporting more favorable results with reconstruction. 13 In the original report by Jobe et al, 13 62.5% of throwing athletes were able to return to preinjury levels of competition. However, the original surgical technique had an unacceptably high complication rate of 31.25% related primarily to submuscular transposition of the ulnar nerve. After modifying their technique, the same group reported 80% good or excellent results with a reduced complication rate of 20%. 22 Subsequently, Andrews and Timmerman 1 and Azar et al 2 have reported results of UCL reconstruction without submuscular ulnar nerve transposition. In these series, subcutaneous ulnar nerve transposition was performed. The complication rates in these series were less than 10%; 81% of players were able to return to preinjury levels of competition in the series reported by Azar et al. Rohrbough et al have further refined the technique of UCL reconstruction with the description of the docking technique. 19 The authors reported a 92% success rate in returning 33 of 36 competitive throwing athletes to preinjury levels of competition. 19 The authors performed subcutaneous ulnar nerve transposition in 2 patients.
We report a similar success rate in a group of elite professional and collegiate throwers using a further modification of the docking technique. This technique offers highly predictable results, with 92% of players returning to preinjury levels of competition. Our time from injury to surgery was shorter than in earlier studies, and we believe this reflects improved means to diagnose these injuries and a better understanding of the poor natural history of complete UCL tears in this population over the decade since the earlier studies were performed. A minimum of 6 weeks of nonoperative treatment was recommended for partial tears with less than 2 mm of valgus laxity. Earlier studies have used a minimum of 12 weeks of nonsurgical treatment, and most of our patients tried longer periods of nonsurgical management, as evidenced by the mean time to surgery of 14 weeks in this group.
The technique is performed through a muscle-splitting approach, thereby preserving the flexor-pronator origin.11,21,22 The technique does not mandate transposition of the ulnar nerve yet allows reliable protection of the nerve. The technique minimizes the number and size of the humeral bone tunnels, thereby decreasing risk of medial epicondyle fracture, yet allows placement of the graft securely within ulnar and humeral bone tunnels. The technique allows secure fixation and proper tensioning of the graft. The use of 4 strands of palmaris tendon graft also offers the advantage of incorporation of increased collagen tissue into the reconstruction. Paletta et al have reported that the biomechanical profile of this modification of the docking technique offers improved initial strength and strain parameters as compared with the traditional Jobe technique (see pages 1599–1603). Limitations of the study include its retrospective nature and its exclusion of high school and amateur throwers. Although it may be assumed that the excellent results noted in this high-demand population are generalizable to other throwers, this is not known and should be addressed in future studies.
Conclusion
The modified docking technique yields highly successful return to preinjury levels of competition rates in a select group of elite baseball players. It is a safe and predictable technique for reconstruction of the UCL. The technique offers a predictably high rate of success and a low complication rate. In our series of elite baseball players, 92% were able to return to preinjury or higher levels of competition.