
Abstract
Background
A rupture of the entire fibers of the anterior cruciate ligament leads to knee instability due to increased anterior tibial translation and increased internal tibial rotation. The influence of isolated deficiency of the anteromedial or posterolateral bundle of the anterior cruciate ligament on the resulting knee kinematics have not yet been reported.
Hypothesis
Transection of the anteromedial bundle will lead to increased anterior tibial translation at 90°. Transection of the posterolateral bundle will show an increased anterior tibial translation as well as a combined rotatory instability at 30°.
Study Design
Controlled laboratory study.
Methods
Kinematics of the intact knee were determined in response to a 134-N anterior tibial load and a combined rotatory load of 10 N·m valgus and 4 N·m internal tibial rotation using a robotic/universal force moment sensor testing system. Subsequently, the fibers of the anteromedial and posterolateral bundle were resected in an alternating order and the new translation in response to the same external loading conditions measured. Statistical analysis was performed using a 2-way ANOVA test.
Results
Transection of the anteromedial bundle increased anterior tibial translation at 60° and 90° of knee flexion significantly. Isolated transsection of the posterolateral bundle increased anterior tibial translation in response to 134-N anterior load at 30° of knee flexion significantly and resulted in a significant increase in combined rotation at 0° and 30° in response to a combined rotatory load compared with the intact knee and isolated resection of the anteromedial bundle.
Conclusion
The anteromedial and posterolateral bundles stabilize the knee joint in response to anterior tibial loads and combined rotatory loads in a synergistic way.
Clinical Relevance
The results of the current study suggest that, from a biomechanical point of view, it may be beneficial to reconstruct both bundles of the anterior cruciate ligament to better restore normal anterior tibial translation and combined rotation.
Several anatomical studies have shown that the anterior cruciate ligament (ACL) can be distinguished into 2 functional bundles, the anteromedial (AM) and the posterolateral (PL).2, 3, 6, 12, 13, 18 Even though there is disagreement on an actual anatomic division of the ACL, it has been proposed that the ACL has functional bands that vary the tension among the fibers in the ligament with different ranges of motion.3, 6, 12, 13, 17, 18 The terminology of the bundles is based on their tibial insertion. The AM fibers originate on the most proximal part of the femoral origin and insert on the anteromedial aspect of the tibial insertion site. The PL fibers originate on the most distal aspect of the femoral origin and insert on the posterolateral aspect of the tibial insertion site.3, 6, 12, 13, 18 Because of the change of the position of the femoral insertion during passive flexion and extension, the fibers of the ACL show a distinct tensioning pattern. When the knee is extended, the femoral attachment of the ACL is in a vertical position, the PL bundle is tight, and the AM bundle is moderately lax. As the knee is flexed, the femoral attachment of the ACL becomes a more horizontal orientation, causing the AM bundle to tighten and the PL bundle to loosen.3, 6, 12, 14 Only limited data are available for the role of AM and PL bundles in tibial rotation.5, 6, 7, 9, 15, 16, 19, 20
In vitro and in vivo studies have suggested that rupture of the ACL leads to significant knee instability.4, 5, 7, 15, 16, 19, 20 The increased anterior tibial translation (ATT) and internal tibial rotation of an ACL-deficient knee may be partially responsible for future degenerative changes in the knee joint. 4 , 7 The goal of this biomechanical study is to determine the effect on knee kinematics of isolated sections of the AM and PL in response to anterior tibial and combined rotatory loading conditions. We hypothesize that the transection of the AM bundle will lead to increased ATT at 90°, and the transection of the PL bundle would lead to an increase at 30°. Furthermore, we hypothesize that after the resection of the PL bundle, the ATT, in response to a combined rotatory load, will significantly increase at 30° of knee flexion when compared with the intact knee.
Material and Methods
Specimens
In this study, 10 fresh-frozen human cadaveric knees were used (age range, 53-71 years). Before testing, the knees were stored at –20°C and thawed for 12 hours at room temperature. To exclude specimens with degenerative changes, deformity, or previous ligament injury, radiographs of all knees were taken and the knees were clinically examined. The femur and tibia were cut 20 cm from the joint line and secured within thick-walled aluminum cylinders with polymethylmethacrylate bone cement (Palacos, Merck, Darmstadt, Germany). The femoral cylinder was mounted to the base of the robot (KR 125, KUKA Robots, Augsburg, Germany) using a custom-made clamp, while the tibial cylinder was connected to a universal force moment sensor (UFS; FTI Theta 1500-240, Schunk, Lauffen, Germany). The UFS was firmly fixed to the end-effector of a 6 degrees of freedom robotic manipulator (Figure 1). To prevent exsiccation of the soft tissues, the skin of the specimens was left intact, and the specimens were moistened with saline irrigation throughout the testing procedure.
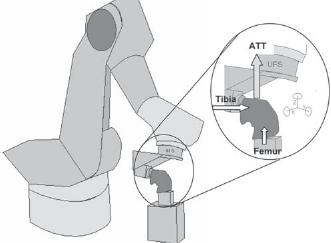
Schematic drawing of the robotic/UFS testing system. The tibia is attached to the robot whereas the femur is fixed to a post. The anterior tibial translation (ATT) in response to a 134-N load imitates a clinical examination.
Robotic/UFS Testing System
To determine the knee kinematics, a testing system for knee kinematics that combines robotic technology with a UFS was used as described by Woo and coworkers.5, 9, 11, 19, 20 In a number of biomechanical research studies, the influence of surgical techniques on knee kinematics and in situ forces of the knee ligaments have been evaluated using this technique.8, 13, 22 The system in our laboratory uses a 6-joint, serially articulated robot that allows 6 degrees of freedom movement of the knee.8, 13, 21 The robotic manipulator is capable of achieving positional control of the knee in 6 degrees of freedom, while the UFS can measure 3 orthogonal forces and moments. Simultaneously, this system is capable of operating in a force-controlled mode via the force feedback from the UFS to the robot.5, 8, 9, 11, 13, 19, 20, 22
Testing Protocol
The path of passive flexion-extension of the intact knee joint was determined by the robotic/UFS testing system by minimizing forces and moments in all remaining degrees of freedom. To do this, the system found the positions of the knee that minimized all external forces and moments applied to the joint throughout the range of flexion from 0° to 90° in 1° increments. The positions were accepted as starting positions for the application of external loading conditions within 0.5 N for forces and 0.2 N·m for moments.
To perform kinematic testing, the robot was used to move the joint to the desired flexion angle and to apply an external anterior tibial and combined rotatory load to the joint. To simulate clinical examination using an instrumented knee laxity measurement, ATT in response to 134 N was applied to the specimen at 0°, 30°, 60°, and 90° of flexion while allowing 5 degrees of freedom motion of the tibia. This load was chosen to simulate a clinical examination using the KT-1000 arthrometer (MedMetric, San Diego, Calif). An anterior load application of 30 force pounds corresponds to a 134-N load, which has been used previously when evaluating injuries to the ACL using a robotic/UFS testing system.5, 8, 9, 11, 19, 20, 22 Afterward, the path of motion in response to combined rotatory loads of 10 N·m of valgus torque and 4 N·m of internal torque was applied at 0° and 30° of knee flexion. This load was chosen to simulate a pivot shift test, and a similar load has been used in previous studies.5, 9, 11, 19, 20, 22
Next, the AM bundle or the PL bundle was transected through a lateral parapatellar incision in an alternating order to simulate an isolated AM or PL bundle tear. In 5 specimens, the AM bundle was cut first, then the PL bundle, and in the remaining 5 specimens, the PL bundle was cut first, then the AM bundle. The functional bundles of the ACL were separated according to their tensioning pattern as described earlier.6, 12, 18 After transection, the incision was closed with 3-0 Vicryl suture material. To assess the ATT of the AM or PL bundle-deficient knee joint, the robot then reapplied anterior external loading of 134 N and a combined rotatory load of 10 N·m valgus and 4 N·m internal tibial torque. In the next step, the remaining fibers of the ACL were transsected and a new set of motions was recorded using the same principles.
Statistics
Because all conditions were tested in 1 specimen, statistical analysis was performed using a 2-factor repeated measures analysis of variance (ANOVA). The 2 factors evaluated were knee conditions (intact, AM deficient, PL deficient) and flexion angle. The dependent variables investigated were knee kinematics and in situ forces in the AM and PL bundles. The significance level was set at P < .05.
Results
Knee Kinematics in Response to 134-N Anterior Tibial Load
In response to a 134-N anterior tibial load, the ATT of the intact knee was a mean (± standard deviation) of 4.0 (±1.7) mm, 8.2 (±1.8) mm, 7.1 (±3.0) mm, and 6.7 (±2.9) mm at 0°, 30°, 60°, and 90° of knee flexion, respectively (Figure 2).
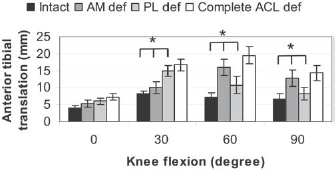
Anterior tibial translation in response to a 134-N anterior tibial load. The increase after sectioning the AM bundle at 60° and 90° was statistically significant. The increase after cutting the PL bundle at 30° was significantly higher when compared with the AM-deficient and intact knee.
The transection of the AM bundle resulted in a mean ATT of 5.3 (±0.6), 10.0 (±1.5), 15.9 (±1.8), and 12.7 (±2.0) mm at 0°, 30°, 60°, and 90° of knee flexion (Figure 2). The difference at 60° and 90° was statistically significant when compared with the intact knee (P = .001, Figure 2). An isolated transection of the PL bundle showed a mean ATT of 6.0 (±0.5) mm at 0°, 14.9 (±1.2) mm at 30°, 10.7 mm (±2.0) mm at 60°, and 8.3 (±0.7) mm at 90° of knee flexion. This difference was statistically significant at 30° of knee flexion when compared with the intact knee (P = .003, Figure 2).
Knee Kinematics in Response to a Combined Rotatory Load
In response to a rotatory load, the ATT of the intact knee was nearly as high as for the anterior tibial load with a mean of 3.3 (±0.9) at 0° of knee flexion and 5.3 (±1.9) at 30° (Figure 3). A transection of the AM bundle of the ACL resulted in slightly higher ATT in response to a combined rotatory load at 0° and 30° of knee flexion (Figure 3). The ATT after resection of the AM bundle was 4.1 (±1.4) mm at 0° and 6.3 (±1.0) mm at 30° of knee flexion. This difference was not statistically significant when compared with the intact knee (P = .08). Posterolateral bundle-deficient knees showed significantly higher ATT at 0° and 30° of knee flexion. The increase of ATT in response to a combined rotatory load after resection of the PL bundle was 6.4 (±1.3) mm at 0° and 6.5 (±0.8) mm at 30°, resulting in a total ATT of 9.8 (±1.1) mm and 11.7 (±2.0) mm at 0° and 30°, respectively (Figure 3). This difference was statistically significant when compared with the AM-deficient knee and intact (P = .003).
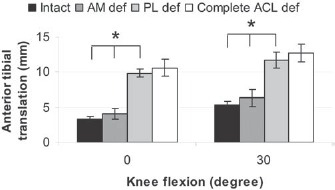
Anterior tibial translation in response to a combined rotatory load of 10 N·m valgus and 4 N·m internal tibial torque. The increase in anterior tibial translation after transection of the PL bundle was statistically significantly higher when compared with the AM-deficient knee and intact.
Discussion
The aim of the current study was to further evaluate the influence of the AM and PL bundles separately on the resulting knee kinematics in response to anterior tibial load as well as to a combined rotatory load. The results suggest that a resection of the AM bundle results in significantly increased ATT in response to an anterior tibial load at 60° and 90°. Furthermore, the results imply that resection of the PL bundle increases the ATT at 30° of flexion significantly. Because of the different tensioning pattern of the 2 functional bundles of the ACL, the ATT increased at higher flexion angles after resection of the AM bundle and at lower flexion angles after resection of the PL bundle. Furthermore, the results of the current study confirm the authors’ second hypothesis: After resection of the PL bundle, the ATT significantly increased in response to a combined rotatory load at 0° and 30° of knee flexion when compared with the intact knee. Transection of the AM bundle did not significantly increase the ATT in response to a combined rotatory load, whereas the PL bundle-deficient knee showed significantly higher ATT. This result may be important to further understand the passive restraints of a pivot shift test.
The ACL is known to be an important stabilizer of the human knee joint and is the primary restraint to ATT and secondary restraint to internal tibial rotation. The most common technique in reconstructing a torn ACL is to use a single-bundle approach, restoring mainly the AM bundle of the ACL. A recent biomechanical study using a robotic/UFS testing system has shown that a single-bundle ACL reconstruction using hamstring or BPTB grafts limited ATT under anterior tibial loads. 19 In response to a combined rotational load, however, reconstruction with either of the 2 grafts was not as effective in reducing ATT. 19 An explanation for this may be that a graft placed close to the central axis of the human knee joint may be inadequate in limiting a combined rotational load. 19 Gabriel et al 5 investigated the in situ forces of the 2 functional bundles of the ACL and showed higher in situ forces in the PL bundle close to knee extension when compared with the AM. In that study, the authors cut everything but the ligament to determine the in situ forces of the AM and PL bundles. The approach of the current study was different. In this study, the focus was to evaluate the resulting knee kinematics in an AM-deficient and a PL-deficient knee. In joint positions close to extension, the PL bundle plays an essential role for the knee joint, especially in response to a combined rotatory load. Because of the insertions points of the AM bundle close to the central axis of the human knee, the ability of the AM bundle to restrain combined rotatory loads was only little. However, the AM-deficient knee showed a significantly increased ATT under anterior tibial loads at 60° and 90° of flexion. Woo et al 19 demonstrated that even though a single-bundle ACL reconstruction is able to limit the ATT, it fails to reduce the anterior translation in response to a combined rotatory load. Similar results were reported by Loh et al. 9 These authors investigated 2 different tunnel positions for the placement of a single-bundle ACL reconstruction and were able to show that ACL grafts placed at the 10 o'clock position significantly better limit the ATT under combined rotatory loads when compared with an 11 o'clock position, but there was a significantly higher ATT under anterior tibial loads at high flexion angles in comparison with a 11 o'clock position. 9
Yagi et al 20 investigated the influence of a more anatomical approach in ACL reconstruction, restoring the AM and PL bundles separately on the femoral side. These authors reported that an anatomical ACL reconstruction restores the intact knee kinematics more closely when compared with a single-bundle reconstruction. From a biomechanical point, it seems that a single-bundle ACL reconstruction placed at either the 10 or 11 o'clock position may not be able to restore the complex structure of the ACL. The results of the current study suggest an additional benefit of restoring the PL bundle in addition to the AM bundle. While a reconstruction of the AM bundle may prevent an ATT at higher flexion angles, a reconstruction of the PL bundle may additionally restrain anterior tibial loads as well as a combined rotatory load at lower flexion angles. Therefore, to further improve surgical outcome after ACL reconstruction, there may be the need for a more anatomical approach to reconstruct the AM and PL bundles separately.
Recently, there has been high interest in the fairly old concept of a more anatomical approach to reconstruct the ACL as described early by Mott 10 and Blauth. 1 Several different techniques are available to achieve this aim. Mott and Blauth reconstructed the ACL in an open-fashioned way. Mott 10 used a semitendinosus tendon graft and osteomized the lateral femoral condyle to drill 2 tunnels into the lateral femoral condyle. Blauth 1 described his technique with fixation of the PL bundle of a quadriceps tendon graft in a femoral tunnel and placing the AM bundle over the top. Today, anatomical ACL reconstructions are performed arthroscopically. Yasuda et al 21 used 2 tibial and 2 femoral tunnels and drilled their femoral tunnels transtibial. Vidal et al 17 reported in their technical description a 2-femoral and 2-tibial technique with allografts and drilled the femoral tunnels through an accessory medial portal. Yagi et al 20 used, in their biomechanical study, a reconstruction with 2 femoral tunnels and 1 tibial tunnel. In some cases with an increased ATT but no pivot shift in the clinical examination, the PL bundle may be intact. In these cases, a careful dissection of the ruptured ACL may reveal a torn AM bundle but an intact PL bundle. Here an augmentation of the PL bundle with a single-bundle AM reconstruction may lead to improved knee kinematics. The same may be true for a partially torn PL bundle. Here an augmentation of the intact AM bundle may be possible.
A limitation of the current study could be the age of the human material used (range, 53-71 y). Even though the age of the material used in this study may not reflect the most typical age for ACL injuries, it is comparable with the mean age of human material used in other studies. 19
In conclusion, this study has shown that the AM and PL bundles of the ACL play an important role for the knee kinematics of the intact knee. In response to a combined rotatory load, the PL bundle showed an important influence on the resulting knee kinematics. The question of whether anatomic ACL reconstruction restoring the AM and PL bundles separately may provide significantly better clinical outcome can only be answered in prospective randomized clinical trials.