
Abstract
Rotator cuff repair surgery for full-thickness tears is common and accepted in orthopaedics today. Given that a significant number of people have asymptomatic rotator cuff tears, the indications for surgery are, however, somewhat unclear. Multiple factors such as duration of symptoms, acuity and size of the tear, patient age, and others require consideration and can influence the decision to perform surgery. This article reviews these variables and the indications for surgery to repair full-thickness rotator cuff tears.
Background
Surgical decision making regarding repair of full-thickness rotator cuff tears is complex. Clinical presentation and patient preferences can be quite variable. Although numerous series of rotator cuff repairs are present in the literature, relatively few delineate the exact indications for surgery. A survey of the American Academy of Orthopaedic Surgeons’ membership demonstrated a lack of clinical agreement about the indications for rotator cuff surgery. 14 Historically, several factors have been considered in the management of these patients; however, these criteria are based on little evidence. Hence, it is difficult to approach this common disorder in an evidence-based manner. The purpose of this review is to establish an evidence-based clinical pathway for patients with rotator cuff disease.
The prevalence of rotator cuff disease has been shown to be quite high and seems to correlate with aging. Magnetic resonance imaging of asymptomatic volunteers demonstrated partial or complete tears of the rotator cuff in 4% of patients <40 years of age and 54% in those >60 years of age. 68 Similar findings of asymptomatic subjects using ultrasound detected a prevalence of rotator cuff tears in 40% of subjects >50 years of age, and when subjects were stratified by age a graded response was seen: 13% in the fifth decade, 20% in the sixth decade, and 31% in the seventh decade of life. 71 Surveys of large numbers of cadaveric shoulders demonstrate similar findings. 46 These studies demonstrate that rotator cuff disease is found in a large number of asymptomatic people. Less is known about the prevalence of symptomatic patients and how and why some individuals become symptomatic. The best data on the natural history of asymptomatic rotator cuff tears were reported by Yamaguchi et al. 81 Patients treated for rotator cuff tears underwent ultrasound on the contralateral asymptomatic shoulder, which revealed that nearly 40% had asymptomatic tears. These authors followed patients with asymptomatic rotator cuff tears with ultrasound examinations and showed that 51% became symptomatic over 2.8 years, and 39% of those tears progressed in size during that time. 81
Patients with rotator cuff disease fall along a spectrum of disease. Neer 59 popularized the concept of 3 stages of rotator cuff disease. Stage I occurs in those younger than 25 years and involves edema and hemorrhage of the tendon and bursa. Stage II involves tendinitis and fibrosis of the rotator cuff in 25- to 40-year-olds. Stage III involves tearing of the rotator cuff (partial or full-thickness) and occurs in those older than 40 years. Debate continues over the causes of cuff pathologic changes regarding intrinsic tendon degeneration versus extrinsic mechanical impingement. With the exception of acute injuries leading to rotator cuff tears, it is generally believed that chronic impingement and tendinopathy can lead to partial tears that progress to full-thickness tears over time. Yamanaka et al 82 performed repeat arthrography on 40 of 61 subjects with partial-thickness tears, and these authors believed that 10% healed, 10% became smaller, 53% became larger, and 28% progressed to full-thickness tears. It is generally accepted that full-thickness rotator cuff tears will not heal spontaneously20,51,76,81; consequently, full-thickness tears likely progress over time with retraction of the tendon edge, which in some individuals can lead to an irreparable tear. Healing is potentially hindered because of poor vascularization in certain regions47,64,66 as well as the intra-articular environment, in which synovial fluid may interfere with healing.
Treatment of rotator cuff disease includes many options that fall along a spectrum of invasiveness. Nonoperative interventions include pain and anti-inflammatory medications, physical therapy, and subacromial injections of local anesthetic, steroid, or both. Operative alternatives include arthroscopic debridement of the tear, subacromial decompression with or without acromioplasty, and repair of the torn tendons. Different permutations of these alternatives have been reported for each of the categories of rotator cuff disease, from subacromial impingement to full-thickness tears. Most series are procedure oriented, consisting of retrospective reviews of 1 surgeon's patient population with limited numbers of patients. There are relatively few condition-oriented studies comparing different treatment options. A Cochrane Database systematic review of the interventions for rotator cuff tears concluded that there is little evidence to support or refute the efficacy of commonly used treatment methods. 15 The focus of this article is the treatment of full-thickness rotator cuff tears.
Nonoperative Treatment
The natural history of rotator cuff disease is not transparent. Clearly, rotator cuff tears are very prevalent and may be asymptomatic. The outcome of symptomatic rotator cuff tears managed nonoperatively gives us some information regarding the course of disease. Bartolozzi et al 3 reported on 136 patients with symptomatic cuff disease and found the following to portend a worse outcome: (1) a full-thickness tear greater than or equal to 1 cm2, (2) symptoms lasting longer than 1 year, and (3) functional impairment and weakness. Thus, these authors recommended that early surgery be considered in these patients. Itoi and Tabata 39 reported on nonoperative management in 62 cuff tears in 54 patients. This was a selected group of patients who were not significantly symptomatic or were undesirable operative candidates, and 72% of patients were found to have good or excellent results after an average of 3.4 years. In this study, better results correlated with less initial patient-reported pain and with greater strength and motion measurements. Bokor et al 7 reported on 53 patients with rotator cuff tears confirmed by arthrography who were treated nonoperatively; 74% of patients had minimal or no pain at 7 years, and 86% rated their result as satisfactory. The most pertinent finding was that two thirds of those patients whose duration of pain was less than 3 months were still asymptomatic at 7 years, whereas only 56% of patients with symptoms for greater than 6 months remained asymptomatic. This study is limited by selection bias, because it did not account for those patients who failed nonoperative means and eventually underwent surgery. Samilson and Binder 67 reported on 292 full-thickness rotator cuff tears managed nonoperatively and found that 72% of shoulders demonstrated greater than 150° of active abduction but 40% were rated as fair or poor results. Hawkins and Dunlop 31 found unsatisfactory results in 14 of 33 patients after nonoperative management.
Rotator Cuff Repair Results
Surgical repair of rotator cuff tears using a variety of techniques has produced satisfactory results in the majority of patients. Although relatively few studies have evaluated the integrity of the rotator cuff after surgery, evidence is mounting that rotator cuff repairs fail at surprisingly high rates. The overall retear rate for rotator cuff tears as determined by MRI is 20% to 39%,45,69,83 and in larger tears (>2 cm) the retear rate at 2 years is even higher (41% to 94%).21,24,72 Interestingly, in most of these series, outcome scores showed significant initial improvement at 12 months despite failure of the repair; however, there appeared to be some deterioration thereafter. Furthermore, patients with an intact repair have significantly better outcomes,24,45 and the outcome of revision surgery for symptomatic failed primary repairs is inferior to successful primary repair, with only 69% patients satisfied. 13 Despite the possibility of retear, attempted rotator cuff repair reduces pain and improves strength and function of symptomatic patients. 40
The lack of understanding regarding the natural history of cuff disease and the perplexing clinical entity of an asymptomatic cuff tear leads to a number of important questions regarding the treatment of rotator cuff disease. First, what factors predict successful nonoperative treatment (ie, returning a symptomatic full-thickness tear back to an asymptomatic state)? Does converting a full-thickness tear to an asymptomatic state allow progression of the tear over time, thereby increasing the difficulty of later surgical repair? Is there an optimal interval during the natural history to repair a full-thickness rotator cuff tear? What factors are associated with failure of rotator cuff repair?
Variables that Contribute to Surgical Management Decision: History
Duration of Symptoms
Patients with rotator cuff tears generally present with complaints of pain of varying magnitude. The pain is generally located over the lateral shoulder region in the area of the subacromial space and deltoid muscle. The severity of pain is variable from one patient to the next. We know that a significant number of patients with full-thickness rotator cuff tears are asymptomatic.68,81 It is unknown what predicts which patients will have pain. There is no consensus on how long a patient should be symptomatic before being offered surgical repair. Studies of rotator cuff patients who were treated nonoperatively found that those patients presenting with pain for at least 1 year correlated with a poor result, 66 and a significant percentage of patients had lasting improvement when symptoms were present for less than 3 months. 7 In patients treated with subacromial decompression for partial rotator cuff tears, tendinitis, or tendinosis, duration of symptoms greater than 1 year negatively affected results. 63 Similarly, patients with a full-thickness rotator cuff repair treated surgically with a subacromial decompression without repair had worse results if symptoms had been present for greater than 1 year.23,51 When evaluating outcome predictors, several authors have found increased duration of symptoms to correlate negatively withoutcome.18,29 Ellman et al 16 determined that a longer duration of symptoms correlated with larger tears and increased difficulty of repair, although duration of symptoms did not directly correlate withoutcome measures after repair. This coincides with the findings that rotator cuff tears will not heal on their own and a substantial percentage will increase in size with time.51,81 However, other authors found no correlation withoutcome and duration of symptoms in their series of rotator cuff repairs,6,36,61,65 and the debate thus continues. On the basis of these studies it seems reasonable to treat patients with symptomatic full-thickness rotator cuff tears with conservative means for a minimum period of 6 weeks to 3 months. Although scientific evidence on this matter is lacking, this has been the general approach of many authors in the literature. This period of nonoperative management is used to monitor for improvement in pain and function. However, longer duration of symptoms has been correlated with histological changes in the muscle that are often progressive and irreversible and potentially increase the difficulty of repair.24,27,72 Therefore, a trade-off of time given for symptomatic improvement versus potential for repair and possible strength return must be recognized. One caveat to this general approach concerns physiologically young patients with rotator cuff tears and acute symptomatic tears. These issues are discussed below.
Age
The definition of a “young” patient with a rotator cuff tear is unclear. Such a person has been chronologically defined as less than 40, 50, or 60 years old. In those series that have used age as a predictor variable in evaluating rotator cuff repair results, older age, when considered a continuous variable, correlated with worse results.10,18,30 When age is arbitrarily categorized, age greater than 65 years has correlated with less satisfactory results after rotator cuff repair surgery.18,65 Patients younger than 60 who were managed with subacromial decompression without repair of full-thickness tears did poorly. 51 Although full-thickness tears are relatively less common in this population, earlier surgery has been recommended for “younger” patients to allow earlier return to work and to high-demand activities.55,61 Immediate repair of full-thickness rotator cuff defects in patients younger than 40 or 50 achieved subsequent good results in the majority of patients in 3 series.48,61,73 However, a long-term follow-up of patients younger than 50 found a substantial number of unsatisfactory results at a minimum of 13 years of follow-up. 69 No prior studies have attempted to evaluate treatment options related to physiologic age, despite the frequent discrepancy between physiologic and chronologic age. No measures exist for assessing physiologic age.
Acute Tear versus Chronic Tear
Acute tears are reported to make up 8% of all rotator cuff tears and are usually related to a traumatic event such as a fall or shoulder dislocation.9,65 The definition of an acute tear is difficult because many patients report an acute event that initiated their symptoms. However, many of these acute events were potentially a new injury to a shoulder that already had a rotator cuff tear. Determining if the rotator cuff tear itself is acute is more difficult clinically and usually requires additional tools to determine, such as MRI to evaluate fatty degeneration, atrophy, and retraction. Bassett and Cofield, 4 in a retrospective series, reported that tears that were repaired within the first 3 weeks of an acute injury had a greater return of motion (abduction) than those repaired from 3 to 6 weeks and those repaired from 6 to 12 weeks. In contrast, Romeo et al, 65 in their series, found that the time from injury to surgery was not significant.
Gender
The role of gender in rotator cuff surgery and outcome is unclear. Men and women were found to have the same results after rotator cuff repair in a series by Hattrup. 30 However, other series have found female gender to correlate with worse outcomes. Female gender was a negative predictor for pain relief, active motion, and results rating in a series by Cofield et al. 10 Romeo et al 65 also found that women older than 65 tended to have worse outcomes.
Variables that Contribute to Surgical Management Decision: Examination Findings
Weakness
The presence of weakness in patients with rotator cuff tears has been implicated as an indication for earlier surgical management. Patients with 3 out of 5 strength or less on manual testing do very poorly with nonoperative management. 3 When these patients were evaluated with a functional measure, less than 50% of those with moderate to severe functional impairment by UCLA score had an acceptable outcome with nonoperative management. 3 In those patients undergoing repair, preoperative strength has been found to correlate with postoperative strength. 10 Preoperative manual muscle testing that reveals weakness, especially less than 4 out of 5 strength on forward flexion and external rotation, has correlated with worse results after surgery for repair.16,18,36
Range of Motion
It is crucial to evaluate the active and passive range of motion in a patient with rotator cuff disease. It is not uncommon to see concomitant adhesive capsulitis and loss of passive range of motion in patients with a rotator cuff tear. When dramatic loss of passive range of motion is found, treatment should focus on improving motion, not repairing the rotator cuff tear. Preoperative active range of motion has been reported to predict postoperative range of motion, strength, and result rating. 10 Less than 100° of active abduction preoperatively has been found to correlate with less satisfactory outcomes after surgery.16,18,61
Signs of Impingement
Most patients presenting for treatment of a rotator cuff tear have positive impingement signs on physical evaluation. The Hawkins sign32,33 and Neer impingement sign58,60 are the most commonly used examinations for this. Some authors have indicated a need for signs of rotator cuff impingement preoperatively before performing a rotator cuff repair.9,22 These physical examination maneuvers have been reported to be very sensitive to rotator cuff tears. 49 An “impingement test” is taken a further step when the shoulder is injected with local anesthetic and the impingement maneuvers are again checked. If symptoms are decreased after injection, the diagnosis of impingement is made. However, Kirkley et al 43 called into question the usefulness of the impingement test because it did not reliably predict outcome after subacromial decompression in patients with tendinosis or partial-thickness tears.
Physical Examination Predictors of Rotator Cuff Tear
Two studies have identified combinations of findings that predict a high probability of full-thickness rotator cuff tear. A 98% chance of a full-thickness tear was found by Murrell and Walton 57 in patients with weakness in abduction, positive impingement signs, and age greater than 60 years. Park et al 62 found that a combination of a positive painful arc sign, 41 a drop arm sign, 8 and weakness in external rotation produced a 91% probability that a rotator cuff tear was present. In addition, Hertel et al 34 described lag signs, which are helpful in diagnosing full-thickness tears. These include the external rotation lag sign and the drop sign.
Variables that Contribute to Surgical Management Decision: Radiographic Findings
Acromiohumeral Distance
The distance between the undersurface of the acromion and the superior aspect of the humeral head has been used as a correlate of chronicity of a rotator cuff tear. A diminishing acromiohumeral distance can be attributable to superior migration of the humeral head into a rotator cuff defect over time. The acromiohumeral distance can be measured on an anteroposterior (AP) or true AP plain film of the shoulder. An acromiohumeral distance of 7 mm or less has been correlated with a larger rotator cuff tear, decreased strength, decreased motion, lower outcome scores after surgery, and decreased satisfaction after attempted repair.16,24
Acromial Shape
Mechanical impingement of the rotator cuff on the undersurface of the acromion has long been implicated in rotator cuff disease. The shape of the acromion is variable and was categorized by Bigliani et al 5 as flat, curved, or hooked. A more down-sloping acromion has been implicated in causing increased mechanical impingement on the underlying rotator cuff and predisposing these patients to tears. The role and importance of acromial shape have, however, been debated recently. Preoperative acromial shape was not found to correlate withoutcome after repair. 18 Rotator cuff pathologic abnormalities have not been found to correlate with acromial shape when age and gender are taken into account, especially in those patients older than 50 years.26,80 Two recent studies found no difference in outcome when a rotator cuff repair was done with an acromioplasty versus without an acromioplasty.23,53
Variables that Contribute to Surgical Management Decision: Advanced Imaging Findings
Tear Presence and Size
Multiple advanced imaging methods are available including MRI, MRI arthrogram, double-contrast arthrography, CT arthrogram, and ultrasound. Each has allowed clinicians to directly and accurately assess for the presence of a full-thickness rotator cuff tear.17,38,44,70 Magnetic resonance imaging and ultrasound are the most common methods of rotator cuff assessment and have been proven accurate in assessing full-thickness rotator cuff tear size.38,70 Ultrasound requires a physician or technician familiar with the technique. Computed tomography arthrogram and MRI arthrogram are more invasive options that may also be used to assess tear size and can give additional information when only a partial articular-sided tear is present. Double-contrast arthrography is less helpful in providing information beyond tear presence. 17 Tear retraction can be assessed with MRI, MRI arthrogram, or CT arthrogram. Ultrasound is more limited in ability to assess retraction. 44 Ultrasound, CT arthrogram, and double-contrast arthrography provide excellent alternatives for advanced imaging in patients with implanted metal, which prohibits MRI.
Treating surgeons generally account for tear size when surgical management is considered. Massive tears are technically more difficult to repair and in some cases irreparable. A rotator cuff tear is generally measured in its greatest dimension. Tears greater than 1 cm2 have been found to have a significantly increased likelihood of an unfavorable outcome when treated with nonoperative measures. 3 As mentioned previously, reduction in tear size or spontaneous healing or repair of a full-thickness rotator cuff tear does not occur.51,81 Larger tears were a negative predictor of outcome in nonoperatively treated patients. 39 In those studies accounting for tear size, large tears portend worse outcomes.6,18,29,30,37,42,56,65,72,80 For example, in the open repair series by Romeo et al, 65 53% of those tears greater than 5 cm2 had an unsatisfactory result.
Atrophy and Degeneration of Rotator Cuff
The rotator cuff muscles undergo change after a tear. The importance of these factors in predicting outcome of rotator cuff tears continues to increase with further research. These changes are 2-fold and include fatty infiltration or degeneration of the muscles and muscle atrophy.16,24,27,72 In sheep models, fatty infiltration and atrophy progress steadily over the first 16 weeks after tendon detachment.11,25 There is also a gradual loss of elasticity of the cuff musculotendinous unit with retraction over time.11,25 Goutallier et al 27 described a staging process for fatty degeneration of the rotator cuff musculature based on CT scans. Stage 0 is normal, stage 1 corresponds to some fatty streaks, stage 2 has more muscle than fat, stage 3 shows a fat content equal to muscle, and stage 4 has more fat than muscle. 27 In this series, Goutallier et al found that fatty changes of the supraspinatus reversed in only 6 of 14 cases, and no fatty degeneration of the infraspinatus reversed after cuff repair. A 50% retear rate was seen when fatty changes of stage 2 or greater were noted preoperatively. Magnetic resonance imaging has also been used effectively to grade these changes after rotator cuff tear.19,28 In rabbit models, no reversal of fat atrophy or fat infiltration was seen when repair was done after a period of detachment, and some muscles actually accumulated more fat in the initial time period after repair.25,52,75 Thomazeau et al 72 described a staging system for describing supraspinatus atrophy after a rotator cuff tear and found that this system predicted the rotator cuff tendon state 1 year after repair. After repair, the atrophy ratio of the supraspinatus showed moderate, although incomplete, reversal.
Nonoperative Interventions for Rotator Cuff Tears
Physical Therapy
A trial of physical therapy to restore and maintain active and passive range of motion and shoulder strength is a common part of the early management of patients with rotator cuff disease. The efficacy of therapy, however, is still a matter of debate. Joint mobilizations and exercise have been found to be efficacious in treating patients with impingement syndrome.12,54 The use of ultrasound has not been found to be efficacious in the setting of rotator cuff disease. Despite the widespread application of therapy, no good randomized trials with enough patients to answer the question of usefulness are currently available.12,54
Subacromial Injection
The use of subacromial injection is multifaceted. It is used as a treatment modality to reduce symptoms and enhance other interventions such as therapy. Also, as described earlier, subacromial injection is a diagnostic tool often used to confirm that rotator cuff disease is the cause of symptoms. A positive response to an injection can predict the response to surgery for rotator cuff tears or impingement.36,50,58 The usefulness of subacromial steroid injection as a treatment modality remains unclear. Several clinical trials for shoulder pain and tendinitis or small tears have been performed to assess the efficacy of injection.1,35,77,79 Of 4 trials, 2 trials showed no difference compared with nonsteroidal anti-inflammatory drugs (NSAIDs), 1 found improvement compared with NSAIDs for tendinitis, and 1 found injection to be good for pain relief for small tears.
The general recommendation is for 3 or fewer steroid injections around a partial or complete rotator cuff tear because of concern over possible adverse effects of injected steroid on cuff tissue. In a rat model, steroid injection once a week for 3 weeks showed no damage to tendon. 74 In contrast, injection every other week for 5 weeks led to microscopic and macroscopic damage consistent with inflammation, necrosis, and fragmentation of collagen bundles. Low-dose steroid injection was not found to decrease the biomechanical properties of the type I collagen in the long term. 78 However, the necessity of adding steroid to the injection is debatable as well. A recent randomized controlled study in 58 patients with partial-thickness tears and tendinosis found no significant difference in outcome when comparing injection of betamethasone with xylocaine and xylocaine alone. 2 All these patients had chronic symptoms and had failed prior therapy and NSAID management. In summary, little evidence exists to support the use of injections either in a diagnostic capacity or as a treatment modality.
Algorithm for Treatment of Rotator Cuff Tears
Justification of Algorithms (Figures 1–3)
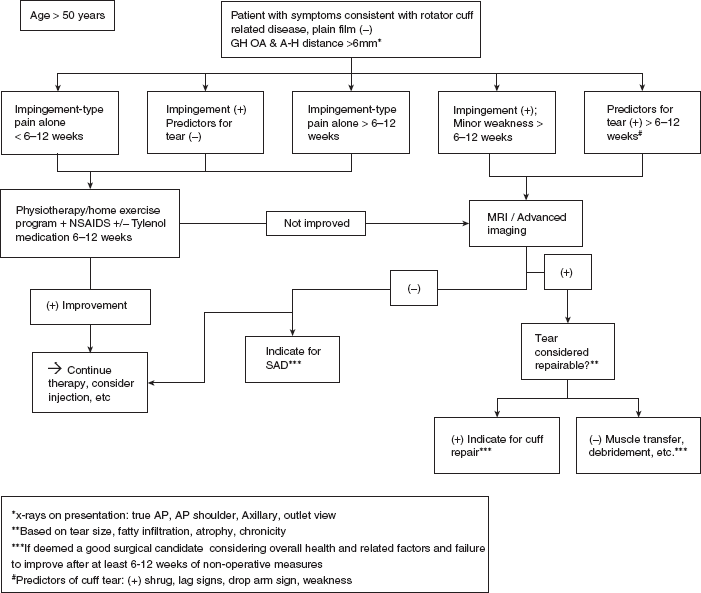
Treatment algorithm for patients older than 50 years of age. GH, glenohumeral; OA, osteoarthritis; A-H, acromiohumeral; NSAIDs, nonsteroidal anti-inflammatory drugs; SAD, subacromial decompression; A P, anteroposterior.
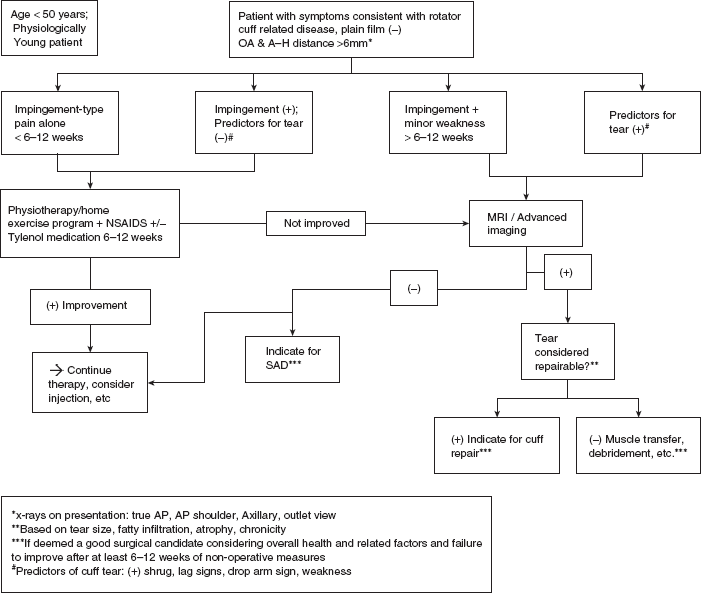
Treatment algorithm for patients younger than 50 years of age and physiologically young patients. OA, osteoarthritis; A-H, acromiohumeral; NSAIDs, nonsteroidal anti-inflammatory drugs; A P, anteroposterior.
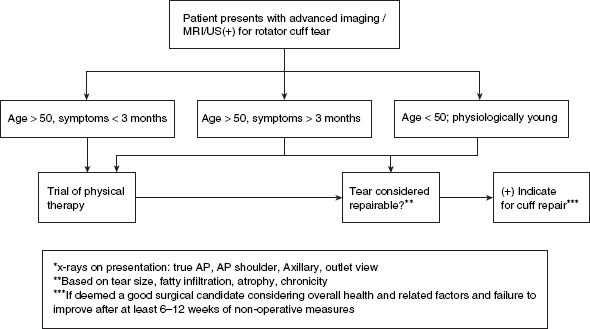
Treatment algorithm for patients who present with imaging positive for a rotator cuff tear. US, ultrasound; AP, anteroposterior.
The goal of rotator cuff repair surgery is to reduce pain and improve function. The vast majority of patients demonstrate reduced pain and improved function after repair, despite evidence that a significant percentage of rotator cuff repairs fail.21,40 The evidence provided regarding nonoperative management of rotator cuff disease suggests a trial of a minimum of 6 weeks to 3 months of nonoperative means before performing surgery in the absence of gross weakness.3,7,39 We advocate against prolonged nonoperative management in symptomatic patients because of the potential negative consequences. These include possible increase in tear size, retraction and difficulty of repair, 16 and fatty infiltration and atrophy,16,24,27,72 all of which correspond to potential diminished results. Patients presenting with strength less than 4 out of 5 on manual testing, with a positive shrug on active elevation of the arm, positive lag signs, or a positive drop arm sign, are unlikely to improve with nonoperative means and should be managed more aggressively. It is the opinion of our group, despite debatable evidence, that patients under the chronologic age of 50 years should be managed more aggressively as well. Additionally, consideration of more aggressive management for those patients over the age of 50 but still physiologically young is acceptable, especially if a tear is deemed acute in nature. Unfortunately, a strict definition of “physiologically young” is lacking in the literature. However, work status and job requirements, sports or recreation participation status, and overall general health can guide assessment of physiologic age.
Despite minimal evidence to support its use, physical therapy has come to be an accepted modality and adjunct for conservative care in rotator cuff disease patients. We continue to use a trial of regular therapy or a home exercise program to work on motion and early strengthening activities in those physiologically and chronologically older patients without profound weakness and without history of an acute tear. We recommend obtaining an MRI, or other advanced imaging modality, in any patient with persistent weakness and clinical evidence of rotator cuff impingement that has not improved after 6 to 12 weeks of conservative management. There is no evidence regarding corticosteroid injection in the setting of full-thickness rotator cuff tears. Multiple injections should definitely be avoided in the case of a known rotator cuff tear that potentially is repairable. An isolated injection can perhaps be used for impingement symptoms when no tear is present, or before advanced imaging, to facilitate therapy exercises.
Our protocol for radiographic assessment includes an AP of the shoulder, true AP, axillary views, and outlet views. If a rotator cuff tear is suspected based on strength testing and history, we advocate obtaining an MRI that includes sagittal oblique images of the rotator cuff musculature medial to the glenoid. We prefer MRI because of its ability not only to assess tear presence but also to evaluate for atrophy and fatty degeneration and potential tear retraction. Other advanced imaging techniques can be substituted for MRI if desired.
Although limited, current available evidence suggests that acute tears are optimally treated with early surgical repair, and we advocate this. Our group has chosen the chronologic age of 50 years, and those select patients over 50 years of age who are deemed physiologically young, as the cutoff for more acute management. These patients are indicated for surgical repair without having to first fail a trial of nonoperative means. Patients over the age of 50 are treated with a minimum of 6 to 12 weeks of therapy-type exercises aimed at decreasing impingement-related pain and focusing on rotator cuff rehabilitation before being offered surgical intervention.
Summary
Most of the guiding principles used for decision making in treating rotator cuff disease are based on limited evidence and minimal science. Factors that seem to be important include duration of symptoms, acuity of tear, weakness, size of the tear, and muscle atrophy and fatty infiltration. Further studies into the indications for rotator cuff surgery are needed.