
Abstract
Background: No comprehensive studies of bone stress injuries in the ankle and foot based on magnetic resonance imaging findings have been published.
Purpose: Using magnetic resonance imaging findings to assess incidence, location, and type of bone stress injuries of the ankle and foot in military conscripts with ankle and/or foot pain.
Study Design: Case series; Level of evidence, 4.
Methods: All patients with ankle or foot pain, negative findings on plain radiography, and magnetic resonance images obtained of the ankle or foot were included in this 86-month study. Magnetic resonance images with bone stress injury findings were re-evaluated regarding location and injury type. Based on the number of conscripts within the hospital catchment area, the person-based incidence of bone stress injuries was calculated.
Results: One hundred thirty-one conscripts displayed 378 bone stress injuries in 142 ankles and feet imaged, the incidence being 126 per 100 000 person-years. This incidence represents the stress injuries not diagnosable with radiographs and requiring magnetic resonance images. Of injuries, 57.7% occurred in the tarsal and 35.7% in the metatarsal bones. Multiple bone stress injuries in 1 foot were found in 63% of the cases. The calcaneus and fifth metatarsal bone were usually affected alone. Injuries to the other bones of the foot were usually associated with at least 1 other stress injury. The talus and calcaneus were the most commonly affected single bones. High-grade bone stress injury (grade IV-V) with a fracture line on magnetic resonance images occurred in 12% (talus, calcaneus), and low-grade injury (grade I-III) presented only as edema in 88% of the cases.
Conclusion: Multiple, various-stage bone stress injuries of the ankle and foot may occur simultaneously in physically active young adults. When considering injuries that were missed by plain radiographs but detected by magnetic resonance imaging, the bones most often affected were the tarsal bones, of which the talus and calcaneus were the most prominent single bones and most common locations for higher grade (IV-V) bone stress injuries. With use of magnetic resonance imaging, early detection and grading of bone stress injuries are available, which enable early and appropriate injury management.
Fatigue bone stress injuries of the ankle and foot typically occur among military recruits, athletes, and sports enthusiasts as a result of excessive increase in the duration or intensity of exercise. These bone stress injuries occur in response to repetitive overloading of normal bone without adequate recovery time. 1
Bone stress injuries of the metatarsal bones, or march fractures as initially described in military recruits, 7 are reportedly the most common bone stress injuries of the foot. Of the metatarsals, the second and the third metatarsals are particularly involved.6,21,27,31
Bone stress injuries on the tensile side of the bone, or in bones with vulnerable blood supply areas such as the medial malleolus, the tarsal navicular, the base of the fifth metatarsal bone, and the first digit great toe sesamoids, can present a high risk for complete fracture, delayed union, or nonunion.5,8,14,29 Bone stress injuries of the distal fibula, the calcaneus, and the other metatarsals have a favorable prognosis if treated early with restriction or cessation of activity.5,6,19
As a diagnostic imaging method for bone stress injuries of the ankle and foot, magnetic resonance imaging (MRI) is as sensitive as scintigraphy but highly specific at showing soft tissue damage as well.4,17 These MRI properties enable prompt treatment of bone stress injuries even before they are evident on plain radiographs. Because of the early intervention, usually only short treatment periods are necessary.
The purpose of the present study was to establish the incidence, distribution, and type of bone stress injuries, based on MRI findings, of the ankle and foot in military conscripts.
Materials and Methods
This retrospective study took place at the Central Military Hospital, Helsinki, Finland. A computer search identified all consecutive conscripts who underwent MRI on account of exercise-induced ankle or foot pain for a period of 86 months, from March 1997 through April 2004. The conscripts were referred to the Central Military Hospital for a consultation with an orthopaedic surgeon because of ankle or foot pain disturbing their military training. The inclusion criteria for the present study were ankle or foot pain, or both, during military service; a physical examination performed by an orthopaedic surgeon at the hospital; a negative finding on plain radiographic evaluation obtained at a primary military health care unit; and an MRI finding of a bone stress injury. The exclusion criteria were a known recent trauma and infection involving the ankle or the foot. The original medical records and MRIs of patients meeting these inclusion and exclusion criteria were retrieved and reviewed for data. Patients with a diagnosis based on radiographs were not included in the study. All patients were treated with reduced exercise and a short period of nonweightbearing if walking caused pain. The study was approved by the Medical Ethics Committee of the Central Military Hospital.
All Finnish men become liable for 6-, 9-, or 12-month military service at the age of 18 years. Military service is voluntary for women. Each year, on average, 26 500 male conscripts and 500 female recruits undergo training in the Finnish Defence Forces. Military equipment was the same for both sexes and remained unchanged throughout the study period. Marching and other forms of physical training, such as running, athletics, games, skiing, and swimming, are actively performed on a weekly basis throughout the service period. The recruits use standard military footwear consisting of boots for marching and athletic shoes for running exercises.
Within the service area of the Central Military Hospital, the total exposure time for the population at risk during the study period was 104 340 person-years. This number was calculated by registering the dates of entry to and transfer or discharge from the hospital for every conscript in the catchment area. Physical examination by the orthopaedic surgeon involved careful history-taking and palpation. Range of movement of the ankle joints and ligamentous stability were examined. Skin changes were recorded. By using a 1.0-T scanner (Signa Horizon, GE Healthcare, Milwaukee, Wis), the symptomatic sites of all patients were MR imaged. The scans were performed in at least 2 different planes, of which sagittal and coronal T1-weighted spin-echo (SE) sequence images and T2-weighted fast spin echo (FSE) sequence images with fat suppression were the most common. Also, additional sequences such as short tau inversion recovery (STIR) were acquired.
Two radiologists re-evaluated the MRIs retrospectively and independently. In cases of disagreement, a third radiologist interpreted the MRI. The MRIs of the ankle and foot were evaluated for bone stress injury location and bone stress injury type. Bone stress injuries of the following anatomic regions were registered: the upper talocrural joint area (tibia, fibula), the tarsal bones (talus, calcaneus, tarsal navicular, cuboid, and cuneiform bones I-III), the metatarsal bones (metatarsal bones I-V), the digits (digits I-V), and the sesamoids and accessory ossicles (first digit sesamoids, os trigonum, os tibiale externum). Bone stress injuries were graded as follows 17 : grade I, endosteal marrow edema; grade II, periosteal edema and endosteal marrow edema; grade III, muscle edema, periosteal edema, and endosteal marrow edema; grade IV, fracture line; and grade V, callus in cortical bone.
Associations between occurrences of bone stress injuries in different anatomical locations were tested with the Pearson χ 2 test. The Mann-Whitney U test was used to test differences in skew continuous data between groups when comparing the length of time from commencement of military service between persons with unilateral fractures and persons with bilateral fractures. Data analysis was performed using SPSS/Win (version 12.0, SPSS Inc, Chicago, Ill) with a significant P value set at .05.
Results
On the basis of MRI findings, 131 patients were identified. Of the patients with stress injuries, 9 were women and 122 were men, with a mean age of 20 years (range, 17-27). Altogether, there were 1 to 11 bone stress injuries of the ankle and foot, including 11 patients (8%) with bilateral injuries. This yielded an incidence of 126 per 100 000 person-years. The incidence for male conscripts was 118 per 100 000, and for female recruits, it was 507 per 100 000. A total of 378 bone stress injuries were detected in the 142 feet or ankles in the following anatomic regions: upper part of the talocrural joint (3.4%), tarsal bones (57.7%), metatarsal bones (35.7%), digits (0.6%), and sesamoids and accessory ossicles (2.6%) (Table 1). A single bone was affected in 53 (37%) feet, and 2 or more bones were affected in 89 (63%) feet (2 bones in 33 feet, 3 bones in 24 feet, and 4-11 bones in 32 feet). Bone stress injuries occurred on the right side in 80 cases and on the left side in 62 cases. There was no relationship in the distribution of bone stress injuries occurring on the left side or the right side.
Magnetic Resonance Imaging Gradings of the Fatigue Fractures of the Talocrural Joint and Foot Bones

Of the 142 feet affected, talus bone stress injury occurred in 55 cases (39%) and calcaneal bone stress injury in 33 cases (23%). Single or multiple metatarsal stress injuries were seen in 75 feet (53%), affecting 135 bones altogether. Bone stress injury of the second metatarsal bone occurred in 42 cases (30%) (Figure 1), of the third metatarsal bone in 37 cases (26%), and of the first metatarsal bone in 29 cases (20%). Of the distal tibial bone stress injuries, 6 occurred around the tibial epiphyseal line (Figure 2), and 2 occurred in the medial malleolus (Figure 3). There were no lateral malleolar bone stress injuries. In the sesamoids and accessory bones, bone stress injuries were as rare as in the distal ankle. A fracture line was seen in 9% of the cases, most commonly in the calcaneus (Figure 4) and in the talus (Figure 5). Endosteal edema occurred in nearly 68% of the cases, involving all bones of the imaged area.
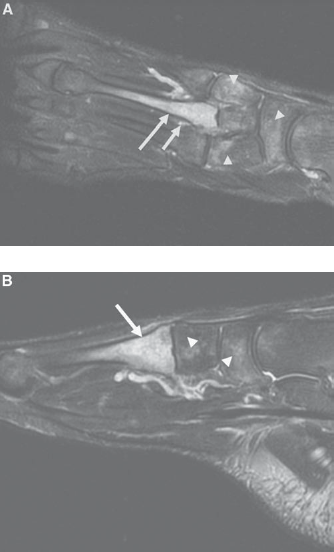
A 20-year-old conscript with left foot pain for 20 days. A, Coronal view: marrow edema in the proximal part of the second metatarsal bone (arrow) and adjacent soft tissue edema (small arrow) are seen. Subtle marrow edema (arrowheads) is also visible on the other bones of the foot. B, Sagittal view of the the same case.
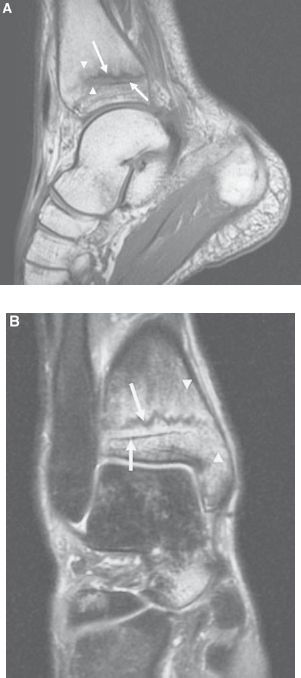
A 21-year-old male conscript with bilateral ankle pain for 14 days. MRI revealed bilateral grade IV bone stress injury of the distal tibia. A, Sagittal T1-weighted spin echo image demonstrates a linear band of low-signal intensity representing a fracture line (arrow) above the epiphyseal line (small arrow) of the right distal tibia posteriorly. The fracture is surrounded by a poorly defined zone of low-signal intensity edema (arrowheads). B, Corresponding findings on coronal T2-weighted fat suppressed MR image. Fracture line (arrow), epiphyseal line (small arrow), high-signal intensity marrow edema (arrowheads).

A 21-year-old conscript with pain in the medial portion of the right ankle for 3 months. Coronal T2-weighted fat suppressed MR image demonstrates a focal high-signal intensity bone marrow edema at the medial malleolus (arrow).
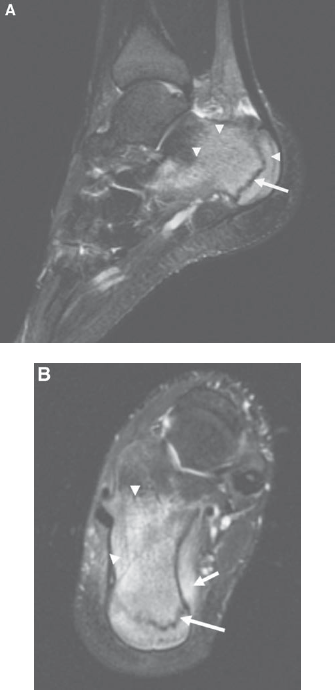
A 21-year-old male conscript with right heel pain for 42 days. A, Sagittal T2-weighted fat suppressed MR image depicts a vertical linear area of low-signal intensity (arrow) extending through the posterior calcaneus consistent with stress fracture. The adjacent high-signal intensity marrow edema (arrowheads) is broad. B, A fracture line (arrow) with surrounding marrow edema (arrowheads) and soft-tissue edema (small arrow) are seen on axial T2-weighted fat suppressed MR image.
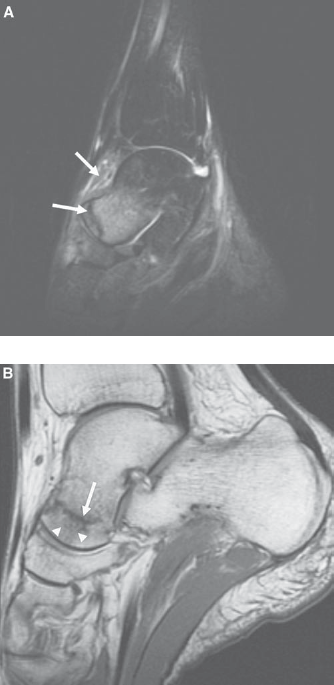
A 19-year-old male conscript with bilateral ankle pain for 20 days. A, Sagittal T2-weighted fat suppressed MR image demonstrates a fracture line (arrow) with surrounding high-signal intensity marrow edema in the head of the talus (in the right leg). Note the anterior soft tissue edema (upper arrow). B, Sagittal T1-weighted MR image shows a fracture line in the talar collum (arrow) with surrounding edema (arrowheads). In talar bone stress injuries, a fracture line is parallel to the talonavicular joint.
In the tarsal bones, except for the calcaneus, and in the metatarsal bones, except for the fifth metatarsal bone, a bone stress injury was significantly more often seen in more than 1 bone (Table 2). Talus bone stress injuries occurred significantly more often simultaneously with stress injuries to the other bones than as solitary (P = .007), with navicular bone stress injury (n = 22/55, 40%) (P < .001), and with calcaneal bone stress injury (n = 18/55, 33%) (P = .033). In the calcaneus, no statistical difference was found between the occurrence of isolated and nonisolated bone stress injuries (P = .779). Tarsal bone stress injuries occurred combined with stress injuries to other tarsal bones and with metatarsal bone stress injuries. Metatarsal bone stress injuries occurred combined with stress injuries of the other metatarsals and with tarsal bone stress injuries.
Location and Number of Bone Stress Injuries of the Ankle and Foot a
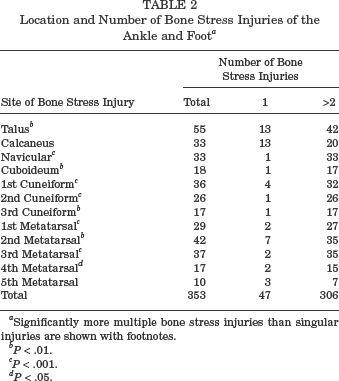
Significantly more multiple bone stress injuries than singular injuries are shown with footnotes.
P < .01.
P < .001.
P < .05.
In all 131 patients, the median length of time from commencement of military service to onset of ankle or foot pain was 30 days (range, 3-330). The onset of the ankle or foot pain was earlier in patients with bilateral bone stress injuries (median, 14 days; range, 2-60) than in patients with bone stress injuries in 1 foot (median, 30 days; range, 2-330) (P = .027). The median duration of ankle or foot pain before a positive MRI finding was 65 days. The clinical findings, for example, tenderness, were not predictive and in many cases did not correlate with the MRI findings.
Discussion
Fatigue bone stress injuries of the ankle and foot are known to commonly occur in athletes and military conscripts. Depending on the study population and the imaging method used, they have been described in any bone of the foot to varying degrees.5,6,19,20,21,23,26,30 Previous studies have indicated that the sensitivity of both MRI and bone scintigraphy are excellent for the detection of bone stress injuries, but bone scintigraphy has shown significantly lower specificity than MRI.1,16,17 Furthermore, it is noteworthy that in bone scintigraphy, the radiation dose is equal to 2 years of background radiation. 13
In the present MRI-based study, as compared with previous studies, the incidence of bone stress injuries involving exercise-induced ankle or foot pain was relatively low in some bones and relatively high in others. It is possible that some of the bone stress injuries of the ankle and foot, especially those of the metatarsals, were already diagnosed on the basis of plain radiographs at primary military health care units, which would explain why they were never sent to orthopaedic consultation and subsequent MRI examination. 24 The total incidence of bone stress injuries of the present study thus reflects the number of injuries that could not be diagnosed by plain film radiographs and the clinical examination of an experienced orthopaedic surgeon. However, the true incidence of these stress injuries may be underestimated because many patients with low-grade symptoms may not have sought medical attention and were therefore not included in the incidence figures.
The number of cases with tarsal bone stress injury was relatively high in our data; more than a half of all bone stress injuries occurred in the tarsal bones. Moreover, more than one third of all bone stress injuries occurred in the metatarsal bones. The second and third metatarsal bones were the most commonly affected, a finding consistent with earlier studies.6,21,27,31 A prior scintigraphic study of 320 athletes with stress fractures documented a similar result; the tarsals (25.3%) and the metatarsals (8.8%) were the most commonly affected anatomical areas of the foot after the tibia (49.1%), which was the most commonly affected bone. 20
Of the 142 feet MR imaged in the current study, talus bone stress injury occurred in 39% of the cases. In this bone, combined bone stress injuries occurred significantly more often than isolated ones. In contrast, the number of cases combining calcaneal bone stress injury with injury to adjacent bones was not statistically significant. According to previous literature, talus bone stress injuries are rare in military trainees and athletes, whereas the calcaneus is the tarsal bone with the highest number of stress fractures.9,21,26,31,32 Calcaneal bone stress injuries among military trainees and athletes have been encountered in activities like parachute jumping and as a result of prolonged standing.9,15 The high incidence of stress injuries in the talus in this study is probably due to the better sensitivity of MRIs compared with radiographs in diagnosing these stress injuries. Stress injuries in the tarsal bones are usually thought to be much less common than those in the metatarsals. However, because metatarsal stress injuries are much easier to diagnose by clinical examination or plain radiographs, many of them were not included in the present study, and their prevalence is probably higher than presented here. Our findings indicate that stress injuries to the tarsal bones can and do occur but are probably more commonly missed than injuries to the metatarsal bones.
In the literature, isolated bone stress injuries of the tarsal navicular, the cuboid, and the cuneiform bones are considered rare, a finding based on only few moderate-sized case series and mainly case reports.2,21 Navicular bone stress injuries are categorized as high-risk injuries because avascular necrosis of the lateral fragment is a potential complication of completely dislocated navicular fractures.14,16,29 However, navicular bone stress injuries have been depicted as uncommon, mainly occurring in joggers and basketball players.5,12,28,30 In the present study, no displaced fractures in the navicular bone were identified.
Distal tibial bone stress injuries seem to occur typically around the former epiphyseal line. 33 A similar location of bone stress injuries, adjacent to the epiphyseal line, has been reported to occur in other parts of the lower extremities as well.10,22,25 In the current study, only a few bone stress injuries were found in the medial malleolus, the first digit sesamoids, and the accessory ossicles. There is evidence that bone stress injuries, acute fractures, and osteonecrosis of the first digit sesamoids at the head of the first metatarsal bone are common in athletes and ballet dancers. 27 Magnetic resonance imaging is valuable for the differential diagnosis. Most of the anatomic bipartite sesamoids are seen in the medial sesamoids. Bone marrow edema, irregular fracture line, soft tissue edema, joint effusion, and synovitis can be found in sesamoid stress fractures 3 and smooth margined bones in bipartite sesamoids.11,18 In this study, bone stress injury of the os trigonum, which in approximately 10% to 14% of individuals remains as a separate ossicle, was associated with bone stress injury of the posterior talus.
In the current study investigating the individual bones of the foot and ankle, the findings of the physical examination, for example, tenderness, correlated poorly with the location of the stress injury on MRI. Many of the patients displayed no tenderness or any other clinical findings upon examination. However, all the patients had foot or ankle pain, and the MRI finding could therefore not be considered clinically insignificant. According to previous evidence, asymptomatic bone stress injuries require no treatment, and asymptomatic patients should not be routinely screened by MRI because it could unnecessarily lead to modification of a training program. 15
The observation that ankle or foot pain and bone stress injuries mainly occur during the basic training period, that is, during the first 2 to 3 months of the military service, is in agreement with prior investigations on bone stress injuries of the lower extremities. 25 Due to the retrospective nature of the study, the delay from the onset of pain to the MRI could not be affected.
Conclusion
In conclusion, multiple bone stress injuries of the ankle and foot, in various stages, were identified in physically active young adults with exercise-induced ankle or foot pain during military service. The tarsal bones were the most commonly affected anatomical area, while the talus and the calcaneus were the most prominent single bones and the most common locations for higher grade (IV-V) bone stress injuries. As the method and duration of injury management for bone stress injuries of the ankle and foot vary depending on the bone involved and the injury grade, the importance of an early diagnosis by MRI should be emphasized for physically active young adults with stress-related ankle and foot pain and with negative radiography results.