
Abstract
Background: Successful anterior cruciate ligament reconstruction requires secure healing between tendon and bone.
Hypothesis: Bone morphogenetic protein-signaling plays an important role in tendon-to-bone healing. rhBMP-2, a powerful osteoinductive agent, can improve tendon-bone interdigitation.
Study Design: Controlled laboratory study.
Methods: The study was designed in 2 phases: Phase I consisted of a dose-response study where 21 New Zealand White rabbits underwent bilateral anterior cruciate ligament reconstructions. Rabbits received either rhBMP-2 (11.5, 50, or 115 µg) or noggin (10, 15, 30, or 100 ng) (a potent bone morphogenetic proteins inhibitor) delivered in an injectable calcium phosphate matrix. Animals were sacrificed at 2 weeks and histomorphometric analyses were performed. In phase II, 60 rabbits underwent bilateral anterior cruciate ligament reconstructions and were assigned to 3 groups: rhBMP-2 (115 µg), noggin (30 ng) in a calcium phosphate carrier, and calcium phosphate carrier alone. Animals were sacrificed at 2, 4, and 8 weeks and histomorphometric and biomechanical analyses were performed.
Results: rhBMP-2 treatment led to a significant increase in the width of new bone formation at the tendon-bone interface in a dose-dependent fashion (0.24-0.35 mm vs 0.13-0.16 mm in controls). All dosages of noggin inhibited new bone formation (0.06-0.1 mm vs 0.15-0.16 mm in controls); however, there was no dose-dependent effect in the concentrations studied. In the phase II study, rhBMP-2 resulted in a significant increase in new bone formation (81%, 89%, and 113%) at increasing time periods compared with controls. Tunnel diameters in the rhBMP-2 group were significantly smaller (15%-45%) than in the carrier group. The negative effect of noggin was not sustained, as new bone formation increased with time. The rhBMP-2 group demonstrated significantly increased stiffness at 8 weeks, while there was no significant difference in ultimate tensile load when compared with the other 2 groups.
Conclusion: rhBMP-2 demonstrated a strong, positive dose-dependent effect on osteointegration at the tendon-bone junction. In contrast, noggin decreased osteointegration. No tunnel widening was detected with rhBMP-2 using the calcium phosphate carrier.
Clinical Relevance: Further studies are needed to investigate the potential clinical application of enhancing healing and decreasing recovery time using bone morphogenetic proteins in soft tissue ligament reconstruction.
Successful anterior cruciate ligament (ACL) reconstruction using a tendon graft, such as semitendinosus and gracilis tendons, requires secure healing between the tendon and bone. The site of ACL tendon graft attachment to bone is the “weak link” in the early healing period, necessitating a delay in return to functional activities. As a result, there is significant clinical relevance to understanding and improving the tendon-to-bone healing process.
It is widely believed that healing between tendon and bone is slower than bone-to-bone healing. Studies from our laboratory have found that tendon-to-bone healing is initiated by the formation of a fibrovascular interface tissue between tendon and bone, followed by progressive bone ingrowth into this interface tissue. This is followed by re-establishment of collagen fiber continuity between the tendon and bone, resulting in an indirect type of insertion. 18 The properties of the normal insertion site are not consistently re-established after surgical tendon-to-bone attachment. The resulting attachment site likely has abnormal material properties and may contribute to recurrent knee laxity. Numerous studies have examined the biological events that occur during remodeling of the intra-articular part of the graft; however, the role of graft-to-bone healing in postoperative knee laxity has not been well investigated.
Despite generally favorable results with ACL reconstruction, instrumented testing of knee stability demonstrates frequent increased anterior laxity, which may lead to symptomatic instability. 4 Furthermore, these studies have found increases in joint laxity over time.3,9,21 Although many factors determine the outcome of ACL reconstruction, including graft fixation site, initial graft tension, and graft material, one of the most important factors is graft healing to bone. Failure of secure healing of the tendon in the bone tunnel before returning to activity can result in graft slippage in the tunnel with resultant increased knee motion.
Another clinical concern is radiographic tunnel widening after ACL reconstruction using a soft tissue graft.5,11,16,22,23 The cause of tunnel widening is not currently known, but several possible mechanisms have been proposed: graft-tunnel motion, synovial fluid influx into the tunnel, and inflammatory cytokines.7,11,16,32 There is concern about the effect of tunnel widening on long-term graft fixation. A recent study reported a positive correlation between radiographic tunnel widening and postoperative knee laxity. 26 Furthermore, bone resorption around the bone tunnel is likely to complicate graft revision surgery. A better understanding of the basic mechanism of tendon-to-bone healing and tunnel widening may allow development of methods to improve healing in these situations.
Bone morphogenic proteins (BMP) have been found to play a fundamental role in bone formation and skeletogenesis. 12 Numerous experimental studies have demonstrated the potential for BMPs to induce both endochondral and intramembranous bone formation in many species. Several studies have also demonstrated the ability of BMP to augment bone ingrowth into collagenous tissue.10,15 Improved bone ingrowth into a tendon graft transplanted into an extra-articular bone tunnel in a dog model was reported by our laboratory after treatment with rhBMP-2 administered on an absorbable collagen sponge (ACS). 19 BMP-2 induces pluripotent stromal cells to differentiate into osteogenic cells and promotes osteoblastic maturation.25,29 BMP-2 also stimulates alkaline phosphatase activity in osteoblastic cells and thus plays an important role in mineralization. 24 Since tendon-to-bone healing requires bone ingrowth into the interface tissue, we hypothesize that BMPs may be involved in the initiation and regulation of bone ingrowth into a tendon graft in a bone tunnel.
The goal of this study is to investigate the effect of the BMP-2 pathway on tendon-to-bone healing. We hypothesized that BMP-2 would improve tendon-bone interdigitation. In this study, we investigated the effect of rhBMP-2 and noggin (an inhibitor of all BMP activities) on tendon-to-bone healing in a rabbit ACL reconstruction model. Prior study in our laboratory using ACS as the delivery vehicle for rhBMP-2 found excessive bone resorption preceding bone formation. 19 In the current study we used a slower releasing calcium phosphate matrix to deliver rhBMP-2, hypothesizing that this material would result in less bone resorption.
Materials and Methods
Study Design
The study consisted of 2 phases. In phase I we evaluated the dose-response to rhBMP-2 (Wyeth Research, Cambridge, Mass) and noggin (R&D Systems, Minneapolis, Minn) in an intra-articular tendon-to-bone healing model. Synthetic calcium phosphate matrix (CPM, Etex Corp, Cambridge, Mass) containing bicarbonate was used as a carrier material for rhBMP-2 and noggin. After identifying the appropriate dosage for each agent, the selected dose was used for phase II of the study.
Animal Model
This study used an established model of ACL reconstruction in the knee of skeletally mature, male New Zealand White rabbits. 2 The rabbits were obtained from a licensed United States Department of Agriculture dealer and were housed in the facility for the care of laboratory animals at our institution, in accordance with the standards established by the National Institutes of Health for the care and use of laboratory animals. This study was approved by the Institutional Animal Care and Use Committee.
Surgical Procedure
An anteromedial incision was made and a medial parapatellar arthrotomy was used to expose the ACL. The native ACL was resected. The semitendinosus tendon was harvested, and drill tunnels (2.4 mm) were created through the femur and tibia at the insertion of the native ACL. The graft was passed through the bone tunnels to replace the ACL. The tunnels were irrigated with normal saline before application of the experimental agents.
Using an 18-gauge spinal needle, we injected 0.5 mL of the CPM carrier containing rhBMP-2 or noggin around the periphery of each tunnel surrounding the tendon graft. The graft was slid back and forth to ensure even coating of the agent along the entire tunnel. The graft was then secured to the periosteum and surrounding soft tissues outside the femoral and tibial tunnels using 4-0 Ethibond suture (Ethicon Inc, Somerville, NJ). All animals were allowed ad lib activity postoperatively. The rabbits typically required 2 days of analgesic agents and usually had a mild limp up to 2 weeks and regular pain-free activities after 2 weeks.
Phase I Dose-Response Study
Twenty-one skeletally mature, male New Zealand White rabbits underwent bilateral ACL reconstructions as previously described. Three rabbits each received rhBMP-2 (11.5, 50, or 115 μg) or noggin (10, 15, 30, and 100 ng) in the CPM carrier in 1 limb. The dosages were chosen based on previous in vivo rhBMP-2 animal studies on tendon-to-bone healing18,19 and in vitro noggin studies.1,6 A 10-fold difference in concentration was included to evaluate the dose response of each agent. The contralateral limb received the CPM carrier only (control). The animals were sacrificed at 2 weeks. Histomorphometric and radiographic analyses were performed (described below).
Phase II Study
The dosages of 115 μg rhBMP-2 and 30 ng noggin were chosen based on the results of the phase I study. Sixty mature New Zealand White rabbits underwent bilateral ACL reconstruction, as described previously. Each animal was assigned to 1 of 3 groups: control (n = 24), rhBMP-2 (n = 18), and noggin (n = 18). For the control group, the CPM carrier was applied to the tendon-bone interface in the left limb while the contralateral limb received no carrier. For the rhBMP-2 and noggin groups, the agents were applied to the tendon-bone interface in both limbs to avoid possible confounding from a systemic effect of rhBMP-2 or noggin in one limb. Animals were sacrificed at 2, 4, or 8 weeks.
For the rhBMP-2 and noggin group, 6 rabbits (12 limbs) were sacrificed at each time period. Four limbs were used for histomorphometric and radiographic analyses, and the remaining 8 limbs were used for biomechanical testing. Eight animals in the control group were sacrificed at each time point, providing 8 limbs treated with the CPM carrier only and 8 limbs with no treatment. Two of these control limbs were used for histomorphometric and radiographic analyses; the remaining 6 limbs were used for biomechanical testing at each time period.
Histomorphometric and Radiographic Analysis
Each limb was carefully dissected and axial sections were obtained from the tendon-to-bone interfaces at the tibial and femoral tunnels. High resolution radiographs were made (Faxitron X-Ray Corporation, Wheeling, Ill). For histomorphometric analysis, the axial sections were fixed in 10% neutral buffered formalin, decalcified in Immunocal (Decal, Congers, NY), and embedded in paraffin. Five-micron thick sections were cut perpendicular to the bone tunnel and stained with hematoxylin and eosin and Alcian blue for routine histologic evaluation using light microscopy. Computerized image analysis (Image J, NIH) was used to measure tunnel diameter, tunnel cross-sectional area, width of new bone formation (NBF) at the tendon-bone interface, and the width of the tendon-bone interface (IF) (Figures 1 and 2). The interface width was the distance measured between the edge of the bone tunnel and the outer tendon. New bone formation was identified as newly formed woven bone along the edge of the bone tunnel. This new bone could be easily distinguished from native lamellar bone.
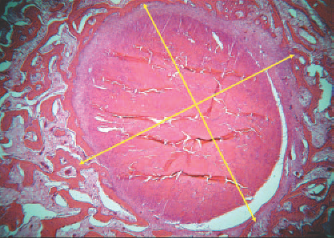
Representative axial section of the implanted tendon. The diameter of the tunnel (yellow line) was measured using computerized image analysis software.
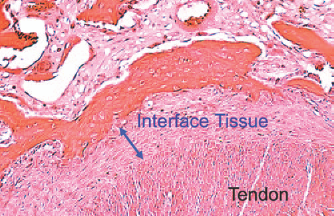
The width of the fibrous interface tissue and new bone formation was measured and averaged across 4 sampled areas along the tendon-to-bone interface. The interface width was the distance measured between the edge of the bone tunnel and the outer tendon (arrows). New bone formation was identified as newly formed woven bone along the edge of the bone tunnel.
Measurements were made at 4 locations along the tendon-bone interface and then averaged. Two observers performed the histomorphometric measurements separately. There were no significant differences between the measurements made by the 2 observers.
Biomechanical Analysis
The limbs that were used for biomechanical analysis were frozen at –80°C until testing. At the time of biomechanical testing, the limbs were thawed and all soft tissue was removed except the grafted tendon. All scar tissue and sutures at the tunnel exits were carefully removed. The femur-ACL graft-tibia complexes were fixed in specially designed clamps (Figure 3) allowing tensile loading along the axis of the graft in a materials testing machine. A preload of 1N was applied. After cyclic preconditioning of the constructs between elongation limits of 0 and 0.75 mm, a load-to-failure test was performed at an elongation rate of 10 mm/min. The failure load was recorded and stiffness (N/mm) was calculated from the slope of the linear region of the load elongation curve between 1.5 and 2 mm of elongation. The site of graft failure (femoral tunnel, midsubstance, or tibial tunnel) was recorded.
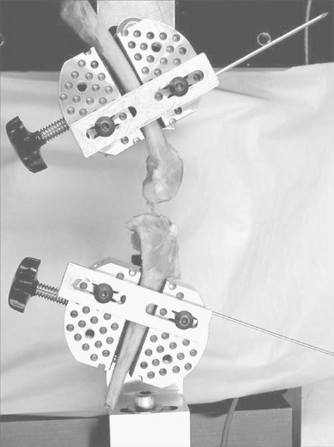
Biomechanical testing was done using a jig to align the ACL graft parallel to the tensile testing axis.
Statistical Analysis
For phase I of the study, the histomorphometric results were compared between the experimental and controls limbs using a paired Student t test. For phase II of the study, comparisons were made between the experimental and control groups using analysis of variance. Two-way ANOVA was performed with Fisher's partial least-squares difference used for post-hoc comparisons. Statistical significance was set at P < .05.
Results
Phase I Dose-Response Study
Healing occurred by formation of a fibrovascular interface tissue in the tendon-bone interface. There was progressive new matrix formation and bone ingrowth resulting in establishment of collagen fiber continuity between tendon and bone. A normal appearing enthesis with fibrocartilage between tendon and bone was not found. Treatment with rhBMP-2 resulted in a significant increase in width of NBF around the graft in a dose-dependent fashion (0.24-0.35 mm vs 0.13-0.16 mm in controls, Figure 4). There was a positive dose-dependent effect of rhBMP-2, with increases of 50%, 120%, and 118% in the width of NBF when compared with the contralateral control (P < .05). The width of the fibrous tendon-bone interface decreased 31%, 7%, and 39% with increasing rhBMP-2 doses compared with controls. High-resolution radiographs verified NBF and a decrease in tunnel diameter in the rhBMP-2 group.
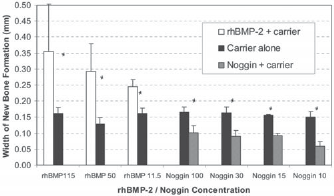
The width of new bone formation (mm ± SD) for the phase I study. The agents studied were rhBMP-2 (11.5, 50, or 115 μg) and noggin (10, 15, 30, or 100 ng). The contralateral side received calcium phosphate carrier only. Three rabbit limbs were used per dosage. *P < .05.
All dosages of noggin significantly inhibited NBF (measured as width of new bone in the tendon-bone interface) (0.06-0.1 mm vs 0.15-0.16 mm in controls) (P < .05); however, there was no significant difference in the inhibition of NBF between noggin dosages (Figure 4). There was a significant increase of 14%, 47%, 60%, and 45% in the width of the fibrous tendon-bone interface with increasing concentration of noggin (P < .05) without a dose-dependent effect. High-resolution radiographs did not reveal any significant changes in tunnel area when compared with the contralateral control.
There were no significant differences in the width of NBF or interface tissue when comparing the control limbs from the rhBMP-2 and noggin groups. There was no discernible effect of application of rhBMP-2 or noggin in one limb on the contralateral control limb, that is, no significant systemic effect was observed. Based on the results of phase I, the dosages of 115 μg rhBMP-2 and 30 ng noggin were chosen for the phase II study.
Phase II Study
Histomorphometric and Radiographic Analysis.
For the control groups, there were no significant differences between the limbs that received the calcium phosphate carrier only (without drug) or no carrier in tunnel diameter, width of NBF, and interface width at all time periods. Thus, these data were pooled for statistical analysis to increase statistical power.
In the rhBMP-2 group there was a significant increase of 81%, 89%, and 113% in the width of NBF at 2, 4, and 8 weeks, respectively, when compared with time-matched controls (P < .05) (Figure 5). There were no significant differences in the width of NBF at different time points within the rhBMP-2 group. There was a decrease in fibrous interface tissue width at later time periods; however, the differences were not significant. High-resolution radiographs demonstrated that tunnel diameters in the rhBMP-2 group became progressively smaller when compared with the carrier control group, with significant decreases of 15%, 25%, and 42% at increasing time periods (P < .05) (Figure 6).
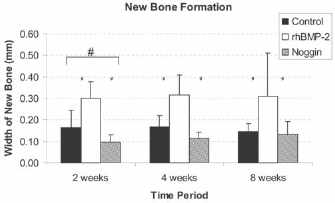
The width of new bone formation (mm ± SD) for the phase II study. *Represents significant difference compared with rhBMP-2 group (P < .05). #Represents significant difference compared with control group (P < .05). For each dosage of rhBMP-2 and noggin tested, 4 rabbit limbs were used for histomorphometric analysis.
In the noggin-treated group, the width of NBF was significantly decreased compared with the carrier control group (0.1 ± 0.03 mm, 59% of carrier) at 2 weeks (P < .05). However, the effect of noggin was not sustained as the width of NBF increased with time. There was no significant difference between the width of NBF in the noggin and the carrier groups by 4 weeks (Figure 5). There was a concomitant increase in the width of interface tissue when compared with the control group; however, this effect decreased with time (67% increase at 2 weeks, 33% increase at 4 weeks, and 25% increase at 8 weeks). High-resolution radiographs did not demonstrate any significant changes in tunnel diameter for the noggin group when compared with the control group (7% decrease at 2 weeks, 26% increase at 4 weeks, and 18% increase at 8 weeks). However, the tunnel diameters in the noggin-treated animals were significantly larger than in the rhBMP-2 group at the 4- and 8-week time points based on high-resolution radiographs (P < .05) (Figure 6).
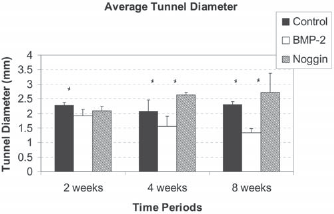
The average tunnel diameter (mm ± SD) measured on high-resolution radiographs in the phase II study. *Represents significant difference compared with rhBMP-2 group (P < .05).
Biomechanical Analysis.
All specimens failed by pullout from the femoral tunnel at 2 weeks, a mix of midsubstance failures and femoral tunnel pull-out at 4 weeks, and primarily midsubstance failures at 8 weeks. There were no differences between rhBMP-2, noggin, and control groups in failure sites. There were no significant differences between the limbs that received the calcium phosphate carrier only (without drug) or no carrier in ultimate failure load or stiffness. Thus, these data were pooled for statistical analysis to increase statistical power.
Ultimate Failure Load.
There were no significant differences in ultimate tensile load between the groups at 2, 4, and 8 weeks. The lack of difference is likely due to the relatively large standard deviations in the data and low statistical power (type-2 error). The failure loads increased over time, with significantly higher failure loads at both 4 weeks and 8 weeks compared with 2 weeks for the control and rhBMP-2-treated groups (P < .05) (Figure 7). Ultimate failure strength increased 72% and 74% for the 4-week and 8-week control group when compared with the 2-week control group. In the rhBMP-2-treated limbs, there were increases of 89% and 162% in ultimate failure strength for the 4-week and 8-week groups when compared with the 2-week group.
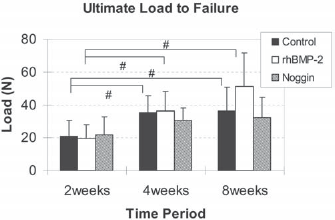
The average ultimate load-to-failure of the femur-ACL-tibia complex for the phase II study. #Represents significant difference when compared with the 2-weeks group (P < .05). For each dosage of rhBMP-2 and noggin, 8 rabbit limbs were used for biomechanical testing.
There were no significant differences in ultimate failure load between the 3 time points in the noggin group.
Stiffness.
There was a progressive increase in stiffness over time in the rhBMP-2 group (Figure 8). Stiffness in the 8-week rhBMP-2 group was significantly greater than the 2-week group (P < .05). In contrast, there were no significant differences in stiffness between the different time points in the control and noggin groups. The stiffness in the rhBMP-2-treated group was significantly greater than both the control and noggin groups at 8 weeks (P < .05).
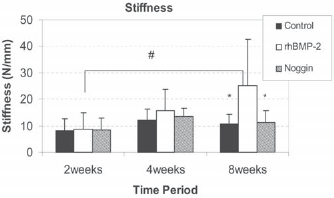
The average stiffness (N/mm) of the femur-ACL-tibia complex for the phase II study. #Represents significant difference when compared with the 8-weeks group (P < .05) *Represents significant difference compared with rhBMP-2 group (P < .05).
Discussion
Previous studies have found that tendon-to-bone healing proceeds by bone ingrowth to the fibrovascular granulation tissue that forms in the tendon-bone interface.18,19 In this study we sought to gain further understanding of this process by testing a known osteoinductive agent (rhBMP-2) and to gain further verification by testing a known BMP inhibitor (noggin). We found that rhBMP-2 has a strong, positive dose-dependent effect on osteointegration at the tendon-bone junction, while noggin had the opposite effect. The effect of rhBMP-2 was sustained throughout the 8-week study period.
Prior studies from our laboratory have shown that rhBMP-2 leads to accelerated bone ingrowth into a tendon graft with an associated improvement in tendon attachment strength at earlier time points in a canine model. 19 That study used an extra-articular model, whereas the current study tested a more clinically relevant intra-articular model. Martinek et al 14 reported that adenovirus-mediated BMP-2 gene transfer to the tendon-bone interface resulted in increased stiffness and ultimate load-to-failure for the transfected graft. Histological sections showed a direct type of tendon insertion for the transfected graft while the untreated controls showed an indirect insertion with Sharpey fibers. 14 Although these prior studies have found that BMP can improve tendon-to-bone healing, our results using noggin verify the role of BMP in bone formation at the healing interface.
An important result in this study was that bone formation in the tendon-bone interface was not preceded by bone resorption using the CPM carrier, in contrast to our prior study using absorbable collagen sponge to deliver BMP-2 to the bone tunnel. 19 This difference is likely due to slower BMP release from the CPM carrier. 20 Although bone resorption is followed by subsequent bone formation, excessive resorption may weaken the tendon-bone interface in the early healing period, potentially compromising graft fixation.
Our study demonstrates the potential for one-time application of an osteogenic protein to improve healing. Although gene therapy approaches provide the possibility of prolonged availability of a therapeutic protein (due to ongoing endogenous synthesis), there are concerns about adverse side effects due to excessively prolonged or uncontrolled expression of the transferred gene. Furthermore, many patients may not accept introduction of a virus. For these reasons we believe it is important to continue to refine techniques for direct application of therapeutic proteins to improve healing. Identification of appropriate carrier materials is an important part of such strategies.
The current study showed that rhBMP-2 improves bone ingrowth into the interface tissue around the transplanted tendon in a dose-dependent fashion, leading to a gradual decrease in tunnel diameter over time. We did not find consistent regeneration of a direct insertion with an intermediate fibrocartilage zone between tendon and bone. However, rhBMP-2 had an immediate and robust effect on bone formation, as demonstrated by the difference compared with controls by 2 weeks, with no significant further change over time in the volume of newly formed bone. The lack of further bone formation suggests that there is a maximum amount of bone that will form at the healing interface. We found similar results in prior studies. 19 The presence of the tendon in the tunnel may inhibit continued bone ingrowth. Further study is required to understand the cellular and molecular signals that govern the complex process of tendon-bone healing.
Although there was a progressive increase in stiffness and failure load of the femur-ACL-tibia complex with time in the BMP-treated animals, there were no significant differences in ultimate load-to-failure compared with controls, likely due to high variances in the biomechanical data. Lack of improvement in graft attachment strength at 8 weeks could also be due to inadequate quality and/or organization of the newly formed bone. The lack of improvement in attachment strength despite greater bone formation may be due to important structural and compositional factors. The newly formed bone may not yet have “anchored” the collagen fibers in the fibrous interface tissue. This bone is also likely to be incompletely remodeled and may not yet be fully mineralized. Clearly, formation of new bone is only one part of the healing process. Integration with the interface tissue and outer tendon are required to improve the structural properties of the femur-ACL-tibia complex.
As another possible explanation for the lack of improvement in graft attachment strength, we hypothesize that the rapid expression of genes required for NBF (due to BMP-2 stimulation) may inhibit expression of genes that are required for normal patterning and insertion site formation. Further study is required to delineate the cellular and molecular mechanisms of tendon-bone healing. However, the results of these studies show that BMP-2 can be used to manipulate the early tendon-to-bone healing process. Further studies are required to determine the optimal BMP-2 dose in humans and to develop appropriate delivery mechanisms.
Noggin is a recently identified molecule that plays an important role in BMP regulation by inhibiting the action of BMPs. Noggin binds BMP-2, BMP-4, and, to a lesser extent, BMP-7, preventing them from interacting with their receptors.30,31 Noggin decreases the stimulatory effect of BMPs on collagen synthesis and alkaline phosphatase activity in osteoblast cells. 6 Thus, noggin inhibits BMP-induced NBF. The important role of noggin in regulating BMP activity in skeletal cells is illustrated by knock-out studies where excess BMP activity in mice lacking noggin resulted in cartilage hyperplasia and failure to initiate joint formation, while noggin overexpression leads to complete absence of skeletal elements. 17 Addition of noggin to bone marrow cell cultures from normal adult mice inhibited both osteoblast and osteoclast formation, effects that were reversed by exogenous BMP-2. 1 These results suggest that BMPs are expressed in the bone marrow and control differentiation of both osteoblasts and osteoclasts, and that noggin may regulate and balance this process. To date, no studies have examined the effect of noggin on fracture healing or bone ingrowth. The results of this study demonstrated a significant inhibitory response on tendon-to-bone healing. There was a decrease in the extent of NBF and an increase in fibrous scar tissue in the tendon-bone interface in animals treated with noggin. The effect was not permanent, as the width of new bone increased with time. The application of noggin led to tunnel widening, likely due to initial bone resorption with delayed bone formation, but no significant changes were found in the biomechanical properties of the femur-ACL-tibia complex.
There have been a number of theories about the causes of tunnel widening after soft-tissue–graft ACL reconstruction.7,8,11,22,23,27,28 Biomechanical studies have shown that significant graft-tunnel motion is present for grafts that are fixed outside of the tunnel (so-called “suspensory fixation”). Despite concern about difficulties that could arise during graft revision, most clinical studies have failed to show any significant adverse effects of tunnel widening at midterm follow-up.5,13 However, a recent study reported a positive correlation between radiographic tunnel widening and postoperative knee laxity. 26 Other theories such as synovial fluid influx have not been proven. We hypothesize that osteoclastic bone resorption secondary to graft-tunnel motion plays a central role in the phenomenon of tunnel widening. The results of this study support the role of bone formation and resorption in tunnel widening. Inhibition of BMP activity by noggin resulted in delayed bone ingrowth and subsequent tunnel widening, suggesting a possible role for BMP/noggin signaling in tunnel widening.
In summary, the results of this study indicate that BMP signaling plays an important role in tendon healing to bone. We found that rhBMP-2 had a strong dose-dependent effect on osteointegration, while noggin inhibited this process. It may eventually be possible to use BMPs clinically to augment tendon-to-bone healing, potentially leading to more rapid rehabilitation, increased tendon-to-bone attachment strength, and diminished risk of recurrent instability.