
Abstract
Background: The results following open revision surgery following a failed arthroscopic Bankart procedure are not well documented.
Purpose: To evaluate the results of patients with a failed arthroscopic Bankart repair treated with a traditional, open Bankart repair.
Study Design: Case series; Level of evidence, 4.
Methods: Thirty patients (28 male and 2 female) who had a mean age of 24 years (range 15-36) at the time of operation were evaluated. The mean interval from the time of the operation to the final follow-up was 46 months (range 24-55). The rating systems of Rowe and the University of California at Los Angeles (UCLA) were recorded preoperatively and at the time of the final evaluation.
Results: After open repair, mean modified Rowe scores improved from 25 preoperatively to 84.2 points. The results were excellent in 2 (6.7%), good in 24 (80%), and fair in 4 (13.3%); there were no poor results. The UCLA shoulder score improved from a mean of 17 points preoperatively to 29 points (P = .001 for all comparisons). Twenty-six patients (87%) did not have an anchor placement inferior to the 4-o'clock position for a right shoulder or the 8-o'clock position for the left shoulder after the index arthroscopic repair. There were no rotator interval closures performed at the index arthroscopic Bankart repair, and 10 patients (33%) required an interval closure at the open revision procedure. Twenty-five patients (83%) immobilized the operated arm in a sling for less than 2 weeks following the index arthroscopic repair.
Conclusion: Patients with failed arthroscopic Bankart repairs can be successfully treated with a revision, open Bankart repair. Inadequate postoperative immobilization, large rotator intervals, and improper anchor placement are possible risk factors that may increase the incidence of failure of an arthroscopic Bankart repair.
The surgical treatment of recurrent anterior instability of the shoulder is evolving. The open Bankart repair 30 has become the preferred procedure because it directly repairs the capsulo-labral anterior-inferior defect and allows for capsular tightening. Many studies have shown that this repair is reliable and has favorable long-term results. 15 The disadvantages include stiffness 26 and subscapularis compromise. 32
Arthroscopic Bankart repair has become increasingly popular because it is less invasive and postoperative stiffness and subscapularis deficiency are minimized. 13 Long-term results are being reported, but the initial series had a higher incidence of recurrent instability than open repair.25,28,35 More recent reports have indicated that the results of an arthroscopic repair can compare favorably with an open procedure.3,6,9,10,12,27 Despite these improved outcomes, there is a concern that certain risk factors may make a patient an improper candidate for an arthroscopic repair.4,5
The purpose of this study was to evaluate the results of patients with a failed arthroscopic Bankart repair treated with a traditional, open Bankart repair. The hypothesis was that such a repair is useful in patients who have a failed previous arthroscopic repair. The second purpose of the study was to identify possible risk factors that may identify those patients who are more at risk for failing an arthroscopic Bankart repair.
Materials and Methods
From January 1999 to August 2003, 30 patients who had undergone an arthroscopic Bankart repair and developed postoperative recurrent anterior instability were included in the study group. Five patients had undergone the arthroscopic repair performed by the author, and 25 patients had their surgery at a different institution. The study group consisted of 30 patients who had a mean age of 24 years (range 15-36 years) at the time of operation. There were 28 male and 2 female patients. There were 24 right shoulders and 6 left shoulders, and in 24 cases the dominant arm was affected.
All of the patients had experienced a traumatic event that caused a dislocation (22 patients, 73%) or a subluxation (8 patients, 27%) after their arthroscopic procedure. The average time after the arthroscopic procedure until the first recurrence of instability was 2 years (range 8 months to 3 years). The mechanism of injury was sports related in 22 of these patients (73%), and 16 patients (53%) required a physician to relocate the shoulder.
The index arthroscopic Bankart repair included 16 patients (53%) with metallic anchors, 4 patients with absorbable anchors (13%), and 10 patients with an absorbable tack (34%). No rotator interval closures were performed at the index arthroscopic Bankart procedure. All of the operative notes of the initial arthroscopic procedure for each patient were obtained and reviewed. Twenty-five patients (83%) immobilized the operated arm in a sling for less than 2 weeks after the index arthroscopic repair. Five patients (17%) immobilized the operated arm in a sling between 2 and 3 weeks postoperatively. All of the patients were examined preoperatively, and sufficient data were collected to rate the shoulders according to the scoring system of Rowe and Zarins 31 and the University of California at Los Angeles (UCLA) shoulder score. 8 All of the patients had a positive apprehension test (with the arm in abduction and external rotation) and relocation test results. All of the patients had a full and equal range of motion compared with the opposite, uninvolved side. There was no loss of external rotation in any of the patients after the failed arthroscopic Bankart procedure. None of the patients had concomitant posterior, inferior, or multidirectional instability. None of the patients had voluntary glenohumeral instability.
All of the patients had preoperative radiographs including anteroposterior, axillary, West Point, and Stryker notch views. All of the radiographs were evaluated by the author, and the Hill-Sachs defect was measured in length in a cephalocaudal direction and in width on an axillary view. Hill-Sachs lesions were seen in 24 patients (80%) but none were greater than 20% of the humeral head. No signs of degenerative arthritis, glenoid dysplasia, or bony Bankart lesions were observed. All of the patients had a preoperative MRI arthrogram of the symptomatic shoulder. All of the patients had an avulsion of the anterior labrum from the glenoid (Bankart lesion). There was no radiographic evidence of implant failure or disruption of the glenoid or humeral head articular surfaces.
The average interval between the initial recurrent subluxation or dislocation after the initial arthroscopic surgery and the subsequent revision, open Bankart repair was 8 months (range 4-16 months). All of the patients were initially treated with at least 6 weeks of physical rehabilitation after their first recurrence of instability following their arthroscopic Bankart repair.
Intraoperative Findings
The shoulders were examined under general anesthesia, and anterior, posterior, and inferior instability was classified using the Altchek grading system. 1 The load and shift test with the arm between 70° and 90° was used to describe and quantify the level of anterior instability. All of the shoulders had a 2+ or 3+ anterior translation. Eight patients (27%) had a sulcus sign in adduction external rotation, which was 1+.
The procedure was performed with the patient in the beach-chair position. 34 Three arthroscopic portals were used including the posterior, anterior-superior, and anterior-inferior. The intraoperative findings are described in Table 1.
Arthroscopic Findings a
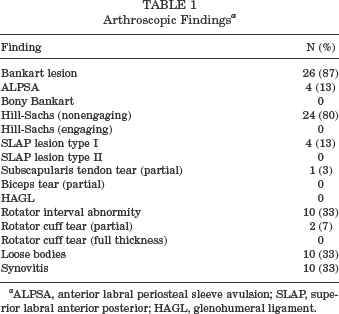
ALPSA, anterior labral periosteal sleeve avulsion; SLAP, superior labral anterior posterior; HAGL, glenohumeral ligament.
Twenty-six patients (87%) had a Bankart lesion (avulsion of the anterior inferior labrum) and 4 patients (13%) had an anterior labral periosteal sleeve avulsion (ALPSA) lesion. These were the principal lesions. There was no evidence that a rotator interval closure had been performed in any of the patients. Ten patients had a diagnosis of a rotator cuff interval lesion, which included redundancy of the capsule between the subscapularis and supraspinatis tendons, fraying of the superior border of the subscapularis tendon, and tearing of the superior glenohumeral ligament. 14
Twenty-six patients (87%) did not have an anchor or tack placement inferior to the 4-o'clock position for a right shoulder or the 8-o'clock position for the left shoulder after the arthroscopic repair. The anchor location was quantified by drawing a clock face at the time of surgery and assigning a clock number based on anchor position.
Operative Technique
The technique was similar to the repair described by Rowe et al. 30 The entire tendinous portion of the subscapularis, within 1 cm from the lesser tuberosity, was reflected off the capsule and retracted medially. The arthrotomy was performed longitudinally just lateral to the glenoid rim with the arm at 30° of external rotation. The medial capsule was mobilized if present and robust, and this was repaired to the glenoid with at least 3 suture anchors. All of the anchors were placed at the 5- or 7-o'clock positions. These sutures were then advanced to the remaining lateral capsule and tied down closing the arthrotomy. When the medial capsule was not easily mobilized or deficient, a classic Bankart repair was done suturing the anchors to the lateral capsule. 31 The subscapularis tendon was repaired in anatomical position with 4 to 6 No. 2 braided nonabsorbable sutures. An excessive gap in the rotator interval or a sulcus sign that did not decrease with external rotation was treated with closure of the rotator interval with sutures passed from the anterior border of the supraspinatus through the soft tissue superior to the subscapularis tendon. A sling was used postoperatively for the first 4 weeks, but the patient was allowed to use the affected hand with the elbow close to the side to avoid external rotation. The patient began physical therapy 4 weeks after the procedure, and range of motion exercises were begun. Patients were allowed to begin throwing at 4 months, and contact sports were allowed at 6 months postoperatively.
Statistical Analysis
The data were analyzed with the assistance of a clinical biostatistician. Preoperative and postoperative Rowe and UCLA scores were compared with the use of the Wilcoxon signed rank test. Comparisons of other preoperative and postoperative variables were compared with use of the Student t test, with the level of significance set at P < .05.
Results
The final follow-up examination was used as an end point to the study. All of the patients had postoperative radiographs. All of the evaluations were done by the operating surgeon and author. Two rating systems revealed significant improvement after surgery when the preoperative scores were compared with the scores at follow-up examination. The mean interval from the time of the operation to the final follow-up was 46 months (range 24-55). The Rowe scale 31 was used to evaluate function and pain (subjective) and stability and range of motion (objective). The subjective range was 10 to 35 preoperatively, and the objective range was 0 to 20 preoperatively. The subjective range was 25 to 60 postoperatively, and the objective range was 30 to 40 postoperatively. After open repair, mean Rowe scores improved from 25 preoperatively to 84.2 points after operation (P = .001). The results were excellent in 2 (6.7%), good in 24 (80%), and fair in 4 (13.3%). There were no poor results. There were no recurrences of instability, and all 30 patients had a negative apprehension test at final follow-up examination. The 24 patients (80%) rated as good had a loss of motion in external rotation of greater than 25% and a slight limitation in sports. The 4 patients (13.3%) rated as fair had loss of motion in external rotation of greater than 25% and a moderate limitation in overhead work, throwing a baseball and football, swimming the crawl stroke, or serving in tennis.
The UCLA shoulder score 18 improved from a mean of 17 points preoperatively to 29 points postoperatively (P = .001 for all comparisons, paired t test). Patients rated their level of satisfaction with the UCLA shoulder score. Preoperatively, none of the patients rated their satisfaction as good or excellent (4 or 5 of a possible 5 points). Postoperatively, all 30 patients (100%) rated their satisfaction as good or excellent (4 or 5 points).
Range of Motion and Strength
The mean loss of external rotation was 8° (range, 2°-12°) compared with the contralateral shoulder with the arm against the body and the elbow flexed at 90°. None of the patients had an increased external rotation postoperatively, and there were no positive liftoff tests. None of the patients were thought to have an incompetent subscapularis muscle based on these findings.
Return to Sports Participation
The 30 patients in this group included 16 high school or college football players; 6 high school, college, or recreational basketball players; 4 high school or college swimmers; 3 high school, college, or recreational baseball or softball players; and 1 college volleyball player. Twenty-six patients (87%) returned to their previous sports activity level. All of these patients had excellent or good results on the Rowe scale. Four patients (13%) rated fair did not return to their former sports activity level secondary to loss of external rotation and moderate limitation in overhead activities. Two high school swimmers and 2 high school baseball players were unable to return to their former sports activity levels.
Complications and Revision Operations
No major intraoperative or perioperative complications occurred. There were no infections and no complications related to the use of the suture anchors. At the most recent follow-up examination, no subsequent surgeries had been performed.
Discussion
The surgical treatment of anterior instability of the shoulder is evolving. Rowe et al 30 reported favorable long-term results of an open repair, and subsequent studies of either open or arthroscopic repair are compared with their results and conclusions. The initial arthroscopic procedures included transglenoid drilling16,25,28 and absorbable tacks,2,33,35 and the results were disappointing.
The use of suture anchors to repair the Bankart lesion and the practices of tightening the lax capsule and closing the rotator interval have improved the outcomes of arthroscopic repair in more recent reports.3,9,10,14,19,21,26
A recent meta-analysis, however, of arthroscopic versus open repair, which only included 11 articles that the authors believed were eligible for full review, concluded that open repair has a more favorable outcome with respect to recurrence and return to activity. 23
Therefore, even though the arthroscopic results are improving and may eventually surpass the open results, they still do not compare with open procedures with respect to recurrence and return to activity at this point in the literature review.6,7,8,15,16,28
A recent report by Sachs et al 32 reinforced why the open procedure is not perfect and why arthroscopic surgeons avoid it and search for an improved arthroscopic technique. The subscapularis muscle must be detached in an open procedure, and the function of this structure is frequently compromised even after it is repaired anatomically. The study demonstrated that a compromised subscapularis muscle, demonstrated by a positive liftoff test and minimal strength, had only a 57% satisfaction rate, and only 57% of the patients would have the same surgery again. The patients in this group removed their slings 2 days postoperatively and were told that they could only use their arm at the side and to avoid external rotation. The authors’ reliance on the patients’ compliance in the postoperative period may have led to the compromise of the subscapularis repair.
The purpose of this study was to evaluate the results of patients with a failed arthroscopic Bankart repair treated with a traditional, open Bankart repair. The results are favorable, with 26 good or excellent results (86.7%) and only 4 fair results (13.3%) as described by Rowe and Zarins. 31 The patients in this revision group maintained their sling for 4 weeks and only removed the sling to extend the elbow daily and to bathe. This regimen may explain the improved postoperative subscapularis function as compared with Sachs’ group, because none of the patients in the present group had a positive liftoff. The loss of external rotation was greater than in Sachs’ group, and the mean loss was 8° (range, 2°-12°). The improved subscapularis muscle function, however, may be secondary to the prolonged avoidance of external rotation, which led to a higher loss of external rotation in the present group. There were no recurrences in this group, but 4 patients (13.3%) had fair results and all of these had loss of external rotation that prevented them from returning to their previous sports activity level.
The results compared favorably with recent reviews of primary open Bankart repairs in similar patient groups.6,9,10,15,19,23 The second purpose of this study was to identify possible risk factors that may identify those patients who are at risk for a failed arthroscopic repair. Intraoperative findings at the time of revision surgery confirmed that there were no anchor or tack placements inferior to the 4-o'clock position for a right shoulder and the 8-o'clock position for a left shoulder after the arthroscopic repair. Previous reports of revision Bankart repair have reported this as well.20,22,24 Garofalo et al 12 discussed the difficulty of inferior anchor placement and yet reported favorable arthroscopic results using knotless suture anchors (Mitek, Westwood, Mass). Others have described the importance of inferior anchor position to enhance repair.5,7 The results in this study appear to confirm the importance of inferior anchor position, which can more adequately pull up loose anterior/inferior capsule as a vital step in the arthroscopic repair. This is merely an observation, however, and there are no data in this study to definitively state that anchor position is a definite risk factor for arthroscopic failure.
Ten patients had absorbable tacks (34%) at the index procedure. The capsular redundancy inherent in anterior instability cannot be adequately repaired with a tack, and perhaps an appropriate arthroscopic procedure would have had superior results. There was no intraoperative evidence that either a capsular plication or a closure of the rotator interval had been performed after the index arthroscopic repair. Ten patients (33%) had evidence of a defect in the rotator interval as described by Gartsman et al 14 and had inferior translation that was not eliminated by external rotation of the shoulder. All 10 patients had a rotator interval repair at the revision, open surgery. The role of the rotator interval in preventing anterior, inferior, and posterior instability is described,17,29, 37 and favorable surgical outcomes are described after interval repair.11,14,31,36
The results in this study appear to support the observation than an enlarged and/or pathologic rotator interval should be repaired to prevent persistent anterior-inferior laxity following labral repair. This, again, is merely an observation, and there are no data in this study to definitively state that the absence of a rotator interval closure when indicated is a definite risk factor for arthroscopic failure.
Twenty-five patients (83%) immobilized the operated arm in a sling for less than 2 weeks and 5 patients (17%) between 2 and 4 weeks after the arthroscopic repair. None of the patients in this group of failed arthroscopic repairs had a loss of external rotation at preoperative evaluation. It may be that a prolonged avoidance of postoperative external rotation with a subsequent loss of external rotation is necessary to decrease the incidence of postoperative instability. Gartsman et al 13 described a minimal loss of external rotation (mean 2%) after arthroscopic repair and still described favorable results compared with open surgery, but their patients used a sling for 6 weeks postoperatively. Recommendations regarding the length of avoidance of external rotation and the use of a postoperative sling are evolving, but it appears from this study that the strict use of a sling to prevent external rotation 4 weeks postoperatively may decrease postoperative instability.
Conclusion
The conclusions of this article are that a failed arthroscopic Bankart repair can be effectively treated by an open Bankart repair. The recurrence rate and compromise of subscapularis muscle function can be minimized, but a loss of external rotation can be expected. In this population of failed arthroscopic Bankart repairs, a large number of patients had minimal postoperative immobilization, large rotator intervals, improper anchor placements, and inadequate fixation techniques (bioabsorbable tack). These factors may have contributed to the failure of initial arthroscopic Bankart repair. The study is limited, however, because there was no control group; the best conclusion is that this group of patients had these characteristics, but it is not known whether these are risk factors because it is not known how many patients without failure have these characteristics.