
Abstract
Background: Fresh osteoarticular allograft transplantation has a long history of clinical success. These grafts have typically been implanted less than 1 week from donor asystole.
Hypothesis: Osteoarticular allografts stored 4 to 6 weeks represent a viable alternative to treat full-thickness cartilage and osteochondral defects of the distal femur as measured by clinical, histologic, and magnetic resonance imaging (MRI) criteria.
Study Design: Case series; Level of evidence, 4.
Methods: Osteoarticular allografts were implanted after a mean graft storage time (at 4°C) of 36 days (range, 28-43). Sixty-seven patients received massive hypothermically stored osteoarticular allografts. Ten knees in 8 of these patients underwent second-look arthroscopic evaluation and biopsy at a mean of 40 months (range, 23-60) after implantation. Clinical assessment was performed using multiple outcome measures and sequential MRI evaluations. Biopsy specimens were obtained from the graft as well as from native articular cartilage at the time of second-look arthroscopy for histologic analysis.
Results: The mean International Knee Documentation Committee scores were as follows: preoperative, 27 (range, 9-55); postoperative, 79 (range, 56-99); P = .002. The mean Lysholm scores were as follows: preoperative, 37 (range, 12-47); postoperative, 78 (range, 55-90); P = .002. The mean Short Form-36 physical scores were as follows: preoperative, 38 (range, 24-55); postoperative, 51 (range, 39-61); P = .002. The mean Tegner scores were as follows: preoperative, 4.3 (range, 1-9); postoperative, 5.3 (range, 4-7); P = .16. The mean International Cartilage Repair Society score at follow-up was 10 (nearly normal) (range, 7-11). The mean modified Outerbridge scores were as follows: preoperative, 4.3 (range, 3-5); postoperative, 0.6 (range, 0-1); P = .002. The mean graft and native cartilage cellular density and viability were not statistically different.
Conclusions: Fresh-stored osteoarticular grafts for full-thickness articular surface defects of the distal femur appear to offer a viable biological method to restore knee function. Our study suggests that osteoarticular grafts stored in cell culture medium at 4°C for 4 to 6 weeks provide successful short-term clinical outcomes.
Full-thickness cartilage loss in the knee is a difficult clinical problem, especially in young patients. Defects involving loss of subchondral bone are particularly challenging to treat in this population. Osteochondral allograft transplantation is one option currently used to address these lesions (Figure 1). This study focuses on the clinical, radiographic, and histologic outcome of large osteoarticular allografts stored 4 to 6 weeks.
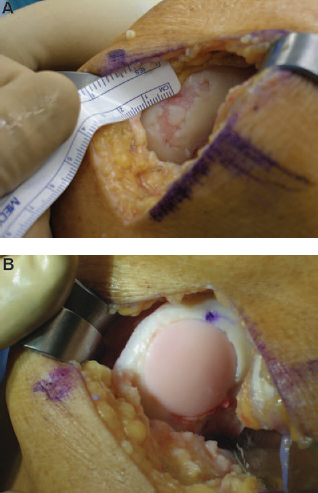
A, defect before osteoarticular graft. B. Defect after graft
Osteochondral allograft transplantation should be considered in the context of a comprehensive treatment algorithm for addressing chondral damage, as well as concomitant lesions, in the injured knee. Treatment of the articular defect depends on the size, location, and depth of the cartilage and potential bone defect. Stability, alignment, meniscal status, and other factors must be taken into account when formulating a surgical plan that may include osteochondral allografting.
Articular defects that may be appropriately indicated for osteochondral allografts include symptomatic lesions of various origins deemed too large for autogenous osteochondral transplantation, osteochondritis dissecans, avascular necrosis, osteonecrosis, or articular injuries associated with subchondral bone loss.
Many authors have reported successful clinical outcomes of fresh osteochondral allografts implanted generally less than 7 days after donor death.4,6,7,11,13,19,22 However, concerns over patient safety and logistical challenges have led to the increased clinical use of hypothermically stored osteochondral allografts. These grafts are maintained hypothermically, at 4°C, in culture medium while donor testing and recipient size-matching are conducted, up to a maximum of approximately 45 days. The weeks after donor death are used to investigate potential donor risk factors and to complete relevant microbial surveillance. These efforts are all designed to maximally ensure recipient safety. Additionally, the extended period between donor death and implantation allows for enhanced use of these donated tissues with better size-matching and more efficient procedure scheduling.
This study describes the clinical outcome of grafts aseptically processed and hypothermically stored in culture medium a minimum of 4 weeks following a mean of 40 months implantation duration. The viability, metabolic, and biomechanical effects of hypothermic storage on osteoarticular grafts maintained similarly to those in this study have been variously reported.1,2,23,26
Methods
After Institutional Review Board approval, patients who had received a hypothermically stored osteoarticular allograft and were approximately 2 years posttransplantation were recruited to participate in the current study. Sixty-seven patients received massive osteochondral allografts over a 5-year period. All of our osteochondral allograft transplant patients are asked to follow up annually. After approval and initiation of this study, those patients sequentially returning to the clinic for follow-up, at 2 years and more from their index surgery, were invited to participate. Fourteen patients were solicited to participate in this study; 6 declined and 8 accepted. The first 10 knees, in 8 patients, that completed this study constitute our study population. All of the grafts were from a single source (CryoLife, Inc, Kennesaw, GA). Before implantation, grafts were maintained at 4°C in a serum-free cell culture medium. They were shipped in temperature-controlled packaging for surgery. Two patients had bilateral surgery, yielding 10 knees in 8 patients for the study. Multifaceted analysis, including follow-up biopsy of graft and native cartilage, sequential MRI scanning, and clinical evaluation was performed on all of the cohort patients. At the time of second-look surgery, the grafts were biopsied at the center of the cylinder. Native cartilage was sampled from a healthy appearing, central weightbearing area away from the graft. For 1 patient with bilateral implants, only 1 sample was obtained from the patient's native cartilage, although biopsy samples from grafts in both knees were obtained.
Surgical indication for osteochondral allograft was a symptomatic full-thickness chondral or osteochondral lesion greater than 2 cm2. Six of the procedures involved the medial femoral condyle alone, 2 of the procedures involved the femoral trochlea, and 2 involved both the medial femoral condyle and the trochlea.
Clinical evaluation was quantified using the International Knee Documentation Committee (IKDC), 19 Lysholm, 18 Tegner, 24 and Short Form-36 (SF-36) 25 scoring systems. The International Cartilage Repair Society (ICRS) cartilage repair index (ICRS Cartilage Injury Evaluation package,© ICRS, Zollikon, Switzerland) was used to assess the repairs intraoperatively at the time of second-look arthroscopy. This quantified analysis tool evaluates multiple parameters, including level of repair relative to surrounding cartilage, integrity of grafted surfaces, graft-host integration, and macroscopic appearance. This system employs a 1 to 12 scale, with 1 being severely abnormal and 12 being normal.
Surgical technique at index surgery involved arthroscopy and arthrotomy. A medial arthrotomy was performed in each case. The recipient site was prepared first, using low-speed drilling and irrigant cooling to minimize thermal damage. The recipient site depth varied between 7 and 15 mm, depending on defect site geometry. The donor graft was prepared to precisely match the recipient site. Grafts were press-fit with minimal force insertion technique to avoid chondrocyte trauma. All grafts were cylindrically shaped using the Arthrex Giant osteoarticular equipment (Arthrex, Naples, Florida). Eight grafts were orthotropic and 2 were not. In all cases, grafts were size-matched between donor and recipient to optimize radius of curvature. Grafts were cut to match the recipient socket on the cancellous side. No fixation was used. All patients participated in an identical rehabilitation protocol postoperatively. Patients were maintained on limited weightbearing with crutches for 6 weeks postoperatively. Patients undergoing ligament reconstruction or osteotomy used a long leg hinged brace, with the hinge released to full motion at 3 weeks. Continuous passive motion was used for 3 weeks postoperatively, or until nearly full range of motion was restored. Patients began full weightbearing after 6 weeks. Outpatient rehabilitation was maintained through the third postoperative month. Return to sports and full activities was allowed 6 months postoperatively.
Concomitant procedures included 1 anterior cruciate ligament allograft reconstruction, 1 posterior cruciate ligament allograft double-bundle reconstruction, 2 distal patellar realignments with tibial tubercle osteotomy, 1 meniscal repair, 1 partial meniscectomy, and 4 cases of isolated resurfacing procedures.
The 8 patients in the study group had an elective second-look arthroscopy and cartilage biopsy under general anesthesia at a mean of 40 months after the initial procedure. Histologic analysis was conducted on osteochondral biopsy specimens harvested from the center of the graft. Native tissue was sampled from the most normal appearing, weightbearing aspect of the femoral condyle outside of the osteoarticular graft. An 8.9-cm Jamshedi (Allegiance Healthcare Corporation, McGraw Park, Ill) bone marrow biopsy aspiration needle, 13-gauge with luer lock adaptor, was used to obtain a 1.5-cm deep osteochondral plug. The specimen was harvested perpendicular to the articular surface. The mean biopsy specimen diameter was 1.5 mm. The collected biopsy specimens were placed into a physiologic tissue culture solution (Dulbecco's Modified Eagle's Medium [DMEM]) and placed on ice immediately after collection and maintained on ice until analysis. The next day, the biopsy specimens were analyzed. Before preparation of the biopsy specimens for analysis, each one was photographed and measured for cartilage thickness. They were then prepared for viability analysis.
Viability of the articular cartilage was determined by a fluorescent dual labeling procedure. 8 The full-thickness articular cartilage was removed from the subchondral bone and sectioned, yielding coronal slices of cartilage approximately 0.5 mm thick. These slices were then placed in a solution of Hoechst 33342 (Aldrich Chemical Co, Milwaukee, Wis), and ethidium homodimer (Molecular Probes, Eugene, Ore). 20 Hoechst 33342 is a lipophilic membrane-permeant DNA intercalating dye that crosses the plasma membrane and stains the nuclei of all cells blue.12,17 Ethidium homodimer is a membrane-impermeant fluorescent dye that will only cross damaged cell membranes and labels the nuclei of dead cells red. 9 The cartilage slices were incubated for 2 hours at room temperature and then placed on microscope slides, coverslipped, and viewed with a fluorescent microscope using a triple-band pass filter.
The entire sample from the superficial to the deep zone was captured at 10× magnification using a high-resolution video camera (Hamamatsu, Hamamatsu City, Japan). Depending on cartilage thickness, 2 or 3 images were taken of each specimen. The numbers of live and dead chondrocytes were determined and the percentage of viable cells per sample was calculated and averaged for each specimen. Cell density was calculated per square millimeter (Figure 2). The remaining cartilage and the subchondral bone were placed into 10% neutral buffered formalin for histologic analysis.
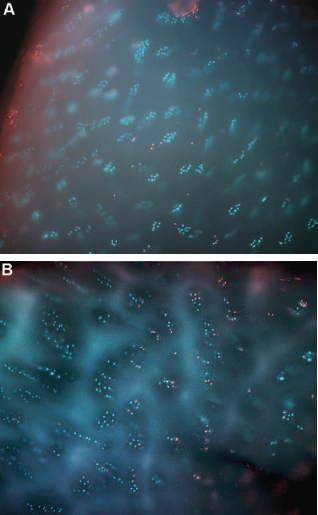
A, live-dead staining of osteoarticular graft biopsy specimen. B, live-dead staining of native biopsy specimen (same patient [control]).
Approximately 1 week before second-look surgery, multi-planar multisequence MRI, optimized for articular cartilage, was performed with a 1.5-T magnet, using the following protocol: axial intermediate T2-weighted fast spin echo (FSE) sequence (repetition time [TR] = 2000, echo time [TE] = 35, echo train length [ETL] = 8), sagittal proton density-weighted spin echo (TR = 2000, TE = 15), sagittal T2-weighted FSE sequence (TR = 2000,TE = 70, ETL = 8) with chemical fat saturation, sagittal 3-dimensional spoiled gradient (3D SPGR) (TR = 60, TE = 5, flip angle [FA] = 40) with chemical fat saturation, coronal T1-weighted FSE sequence (TR = 500, TE = 20, ETL = 3), and coronal T2-weighted FSE (TR = 2000, TE = 80, ETL = 8) with chemical fat saturation. After image acquisition, MRI studies were filmed and interpretation was performed by a fellowship-trained musculoskeletal radiologist. Results were measured according to a variant of the modified Outerbridge classification. The articular cartilage was graded as follows: grade 0 indicated normal cartilage; grade 1, cartilage edema and swelling; grade 2, superficial fraying; grade 3, surface irregularity and partial-thickness chondral loss; grade 4, full-thickness cartilage loss; and grade 5, transchondral fracture (Figure 3).5,13,19,21 Additionally, MRI scans were analyzed to assess bony incorporation of the grafts.
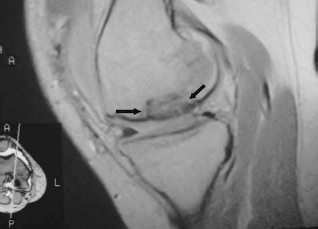
MRI of osteoarticular graft (arrows) in situ postoperatively.
Weightbearing posteroanterior and lateral radiographs were obtained preoperatively and at the time of second-look evaluation. Maintenance of joint space and bony incorporation were analyzed. The joint space was measured using scaled radiographs, and bony incorporation was evaluated according to bony trabeculation and presence or absence of lysis or cyst formation.
Statistical Methods
Descriptive statistics (means and standard deviations) were calculated for all variables. Data populations were evaluated for normality using the Lilliefors test for normality. A paired t test was performed for normally distributed data and the Wilcoxon paired signed rank test was performed for all nonnormally distributed data. Simple linear regression was employed to look for any potential relationships between graft storage time and follow-up time with cellular viability, density, and clinical outcome scores. All statistical analyses were completed using GraphPad Prism version 3.00 for Windows (GraphPad Software, San Diego, Calif). A P value < .05 was considered to be statistically significant. Power calculations were not performed for this data set but are assumed to be low because of the small sample size.
Results
Demographics for the 8 patients in the study group included a mean age of 32.6 years (range, 21-48). The cause of the chondral or osteochondral lesion was osteochondritis dissecans in 5 knees and trauma in 5 knees. There were 4 women and 4 men; the 2 bilateral cases were both women. The mean defect size was 6.2 cm2 (range, 2.5-17.2). Graft demographics included a mean donor age of 24.7 years (range, 15-45). Mean days between donor death and implantation was 36 (range, 28-43). The mean interval between implantation and biopsy was 40 months (range, 20-60) (Table 1).
Patient, Donor, and Graft Storage Data a
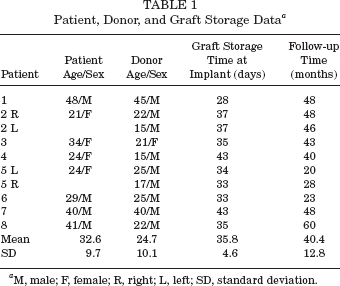
M, male; F, female; R, right; L, left; SD, standard deviation.
Demographic data for the cumulative group of 67 patients, inclusive of the 8 study patients included to constitute the study cohort, were a mean age of 35.5 years (range, 14-72). There were 37 men and 30 women. The mean defect size was 5.4 cm2 (range, 0.5-17.2). The mean days between donor death and implantation were 37 (range, 15-45). The demographic constitution of the 8 study patients is similar to the larger group of 67 from whom the patients were recruited. Additionally, graft characteristics were similar between these 2 groups.
The mean preoperative IKDC score for the study group of 10 knees was 27 (range, 9-55) and the postoperative mean was 79 (range, 56-99). This improvement was statistically significant (P = .002). The IKDC scores for the cumulative group of 67 patients preoperatively averaged 27 (range, 6-56) and the postoperative mean was 77 (range, 42-99). This summary score system incorporates patient subjective data on functionality, pain, perceived physical parameters, and quality of life. The IKDC score has been validated as a measurement tool for articular cartilage lesions. 16 Furthermore, the ICRS has elected to use this outcome measurement as a standardized method with which to evaluate patients undergoing cartilage repair procedures. The Lysholm scores improved from a preoperative mean of 37 (range, 12-47) to a postoperative mean of 78 (range, 55-90); this was statistically significant (P = .002). The mean preoperative Tegner activity level was 4.3, with a mean postoperative level of 5.3 (P = .160, not significant). Only 2 patients had decreased scores, both representing lifestyle changes unrelated to their knees. SF-36 data was collected for both the mental and physical component of self-assessment. The SF-36 mean physical scores improved from 38 (range, 24-55) to 51 (range, 39-61). This improvement was significant (P = .002). The SF-36 mean mental scores showed minimal improvement and were not significantly different from preoperative scores (P = .322). The ICRS mean overall repair assessment score was 10 (nearly normal) (range, 7-11) (Table 2). Linear regression analysis showed no correlation of graft storage time or postoperative follow-up time with IKDC, Tegner, Lysholm, SF-36, or ICRS scores.
Clinical Outcome Scores a
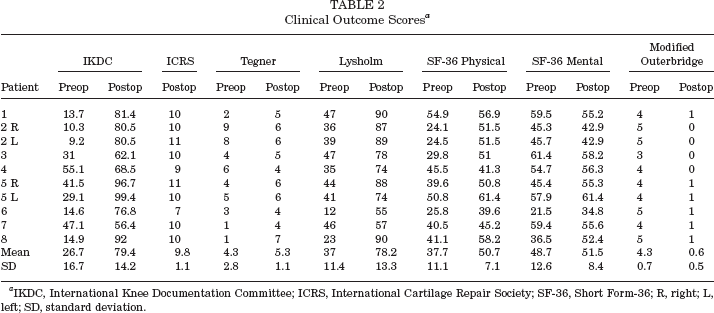
IKDC, International Knee Documentation Committee; ICRS, International Cartilage Repair Society; SF-36, Short Form-36; R, right; L, left; SD, standard deviation.
At the time of the second-look arthroscopy, 10 graft and 9 native biopsy samples were taken for analysis as described. The mean thickness of the articular surface of the biopsy specimens from the grafts was 3.2 mm (range, 1-4). Native cartilage biopsy specimen thickness was 3.3 mm (range, 2-4) (Table 3). The 2 groups were not statistically different with P = .625 (Wilcoxon paired signed rank test). Graft biopsy specimens from the 10 knees at second-look arthroscopy demonstrated mean chondrocyte cellular viability of 78% (range, 53%-92%). The 9 biopsy specimens taken from the patients’ native cartilage had a cellular viability mean of 71% (range, 22%-97%). Chondrocyte cell density for the 10 graft biopsy specimens was a mean of 429 cells/mm2 (range, 69-896). Cell density from the 9 biopsy speciemens from the patients’ native cartilage was a mean of 345 cells/mm2 (range, 144-824) (Table 3). Neither percent viability (P = .555) nor cell density (P = .129) were statistically different by paired t test between the graft cartilage and the patient's own cartilage. Linear regression analysis demonstrated that graft storage time had no influence on cell density (P = .118, R 2 = .277) or cellular viability (P = .515, R 2 = .055) at biopsy. Follow-up time had no significant effect on graft viability (P = .576, R 2 = .0410) but did show a slightly negative influence on cell density (P = .007, R 2 = .619). Histologic examination of the biopsy samples showed chondrocyte cloning in some of the grafts and native tissue. 3
Graft and Native Cellular Viability and Density Data a
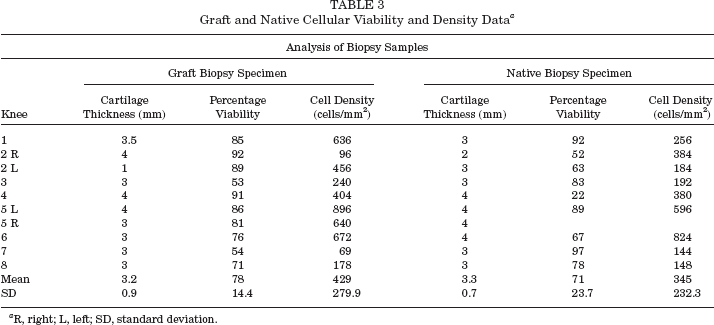
R, right; L, left; SD, standard deviation.
The gross appearance of the grafts at the time of second-look arthroscopy demonstrated persistence of a small seam surrounding the cylindrical grafts. In all cases, the border surrounding the graft was visible at the time of biopsy. All grafts were firm to palpation and grossly similar to native cartilage elsewhere in the knee. The 1 case with an ICRS score of 7 (abnormal) was noted to have partial fibrillation on a small segment of the allograft seen at the time of biopsy.
Magnetic resonance imaging evaluation demonstrated improvement in all patients. The MRI scans demonstrated complete incorporation of the bony component of the graft in each case. The mean preoperative score of 4.3 improved to 0.6 postoperatively. This improvement in MRI scores was significant (P = .002) (Table 2). Preoperative MRI scanning showed exposed subchondral bone in 7 of 9 patients. At the time of index surgery, all patients had exposed subchondral bone. All 8 patients at the time of biopsy were classified as normal (n = 4, grade 0) or nearly so (n = 6, grade 1 [softness, swelling or edema]). Simple linear regression showed no correlation of graft storage time or postoperative follow-up time with the MRI evaluation scores.
Plain radiographs demonstrated bony incorporation in all grafts. Weightbearing images showed maintenance of joint space in all cases.
Discussion
Osteochondral allograft transplantation is a method of biological restoration for full-thickness cartilage and osteochondral loss in a diarthrodial articulation. This study analyzed hypothermically stored osteochondral allografts of the distal femur. We have evaluated the study patients and the surgical results using a multiplicity of clinical measurement instruments while analyzing the grafts with systematic arthroscopic inspection, biopsy, and sequential MRI imaging. The multiple goals of biological restoration include decreasing pain, increasing function, restoring functional histologic architecture, preventing degenerative changes, and avoiding early arthroplasty. Our data in this case series indicate that we were successful, in the relatively short term, in diminishing pain, increasing measured functionality, reestablishing functional articular cartilage anatomy, and avoiding arthroplasty. The mean follow-up period of 40 months is too brief to determine the efficacy of avoiding degeneration and the long-term prevention of the need for arthroplasty in these relatively young patients. These challenging goals must all be accomplished while maintaining patient safety.
The osteochondral transplant procedure appears to have been effective in our subgroup of 10 knees, as measured by the various clinical assessment tools we used. We used a variety of measurement instruments to query and quantify our results. Each of the tools (IKDC, Tegner, Lysholm, and SF-36) provides somewhat different perspectives on clinical outcome. Each of these scores showed improvement in our patients undergoing osteochondral transplantation with fresh-stored grafts during the follow-up period.
The arthroscopically observed quality of the cartilage repair was measured at the time of second-look arthroscopy. The appearance at second-look evaluation was measured and reported according to the ICRS repair score. Although preoperatively all patients had exposed subchondral bone, at follow-up nearly normal restoration of cartilage was found to be achieved in all but 1 patient. These results demonstrated a very successful outcome, surgically restoring the congruity of the articular surface with the osteochondral allograft procedure in our patients.
The grafts maintained gross integrity as measured macroscopically. Measured thickness of graft and native cartilage was nearly identical. The cartilage of the osteoarticular graft did not thin or undergo visible degeneration after transplantation.
Histologic analysis was performed by measuring cellular viability and cellular density, comparing graft to native cartilage. Cellular density and cellular viability showed no statistically significant differences between the native and grafted cartilage. The grafts appeared to maintain cellular viability during implantation, although the observation of chondrocyte cloning in some grafts is of concern. 3 It is well known that chondrocyte cloning is an indicator for native cartilage degeneration, but no studies have shown that the same mechanism is occurring in transplanted allograft cartilage. Further studies to elucidate the cause and effects of this cloning would be of vital interest. In general, the fresh-stored osteoarticular grafts maintained favorable histologic criteria as measured in this study at the time of biopsy.
Magnetic resonance imaging analysis demonstrated maintenance of allograft cartilage appearance in all knees evaluated at the time of biopsy. In each knee, MRI evaluation documented improvement in cartilage appearance of at least 1 grade of Outerbridge classification. There was a mean improvement of 3 Outerbridge grades. Bony incorporation was evident on MRI and plain radiographs in all cases. The interface between graft and host bone showed no bone loss or cyst formation. Magnetic resonance imaging appears to be a useful tool to monitor osteochondral allografts, but further study with larger numbers of patients may clarify the exact MRI parameters associated with the status of these grafts. Perhaps enhanced MRI protocols could yield greater diagnostic accuracy for clinical utility.
The present study evaluated hypothermically stored osteoarticular allografts. These must be differentiated from fresh grafts. Fresh grafts have typically been implanted at less than 7 days after donor asystole. Many authors4,6,7,11,13,14 have reported on the long-term and intermediate-term success of these fresh grafts. Ghazavi et al 13 reported 85% successful transplantation with fresh grafts up to 2 decades after transplantation. Failures in their series of 126 knees were correlated to age over 50 years, malalignment, a bipolar defect, and the presence of a workers’ compensation claim. Czitrom et al 7 demonstrated 69% to 78% chondrocyte viability of fresh osteochondral allografts of the femoral condyle with biopsy specimen analysis performed 2 years after implantation. Chu et al 6 reported 73% good or excellent results in patients more than 10 years after fresh osteochondral allograft transplantation. They used an 18-point scale, with 6 points each for pain, range of motion, and function. Overall, they report 84% good or excellent results in 43 patients with unipolar fresh osteochondral allografts. Bugbee and Convery 4 successfully performed hundreds of osteochondral allograft procedures on isolated femoral condylar lesions. They report rare failure in short-term follow-up of fresh monopolar allografts. These authors highlight the fact that fresh grafts present practical difficulties with limited availability, logistical challenges, and safety concerns when implanting fresh grafts. Garrett 11 has also reported good and excellent success with fresh transplantation for osteochondritis dissecans. In his series, 16 of 17 cases were deemed successful at a minimum follow-up of 2 years.
While fresh grafts may represent an ideal situation theoretically, several mitigating factors favor the use of stored grafts. The foremost parameter motivating the trend toward stored grafts is patient safety. Additionally, both the US Food and Drug Administration, through its Good Tissue Practices Regulations, 10 and the American Association of Tissue Bank guidelines 15 make the use of fresh grafts difficult, if not impossible. In contrast, an elongated time between donor asystole and graft implantation allows for increased pathogen testing and exhaustive donor screening. Many bacterial and viral assays are time-consuming and can only be completed within an extended time frame. Furthermore, autopsy data, when available, may only be released by authorities several weeks after donor death. An elaborate, maximum safety system to identify a myriad of risks takes many weeks to complete. Storage of grafts also has the added benefit of increasing use of this donated tissue. Under the current screening system, much donor tissue is discarded while testing and donor data are unavailable. Extending the storage time of these grafts also enhances the logistics of matching donor to recipient and scheduling surgery. Patient safety and logistics of graft transplant are both enhanced by the storage of osteochondral allografts. The results of our study suggest that fresh-stored osteochondral allografts may offer an acceptable alternative to fresh grafts.
Many studies have characterized osteochondral tissue after hypothermic storage. Pearsall et al 23 recently published their data on hypothermically stored osteochondral allografts used for transplantation within the knee. At the time of implantation, these investigators found a mean chondrocyte viability of 67% in 16 grafts stored an average of 30 days (range, 17-44) from asystole to implantation.
Allen et al 1 also analyzed osteochondral allografts stored hypothermically at the time of implantation. They reported decreased chondrocyte viability, cell density, and metabolic activity at a mean of 20 days compared with their fresh grafts. They concluded that analysis of fresh-stored grafts, such as those in the present report, are necessary to ascertain the significance of their findings. Ball et al 2 performed analyses of fresh-stored osteochondral allografts stored up to 28 days. In specimens maintained in typical culture medium, they reported a chondrocyte viability mean of 83%. They found equivalent rates of decline in viability in each of the different cartilage zones. The greatest absolute decline in cellular viability was found in the superficial zone. These authors also observed a decline in chondrocyte synthesis of proteoglycans over time. Biomechanical testing of their specimens showed no significant decline in compressive modulus or permeability over the testing period. Our study provides clinical, radiographic, and functional correlation of these findings on grafts similarly stored and followed a mean of 40 months after transplantation.
The time between donor death and transplantation has potential implications impacting cellular viability, cellular density, metabolic characteristics, and mechanical integrity. In our study, we found no correlation between graft storage time at implantation and cellular viability or cellular density after a mean of 40 months implant duration. In fact, cell viability in our biopsy specimens after implant was in line with that observed by Pearsall et al 23 before implant. It is possible that study of chondrocyte metabolism may have demonstrated a negative effect of storage time, but that was not measured in this series. We sought to correlate outcomes on MRI, IKDC, Tegner, Lysholm, SF-36, and ICRS repair scores related to graft storage time. Unfortunately, with a low number of patients and relatively uniform graft storage times, we were unable to statistically correlate the effect of graft storage time on our results. Pearsall et al, 23 evaluating grafts at implantation, found excellent viability in grafts stored up to 44 days before implantation while noting a time-related decrement in matrix staining scores. They used a 2-color fluorescent assay method to measure chondrocyte viability. Williams et al 26 also evaluated the effects of storage on osteochondral grafts maintained hypothermically. At 28 days, they found a significant decrease in chondrocyte viability and density and decreased proteoglycan synthesis. They found no diminished glycosaminoglycan content, compressive modulus, permeability, or tensile modulus in grafts stored 28 days. While some properties of hypothermically stored grafts are reported to degrade during storage, and may have negative implications, grafts stored up to 43 days in this study fared well according to our measured parameters. Continued longitudinal study of these patients will be necessary to evaluate continued graft survival and to further identify potential consequences of graft storage.
Success of the osteochondral grafts in our study may be related to factors associated with the procedure, the graft, the recipient, or a combination of these. The graft donor age was younger than the recipient with respective means of 25 and 33 years. The grafts were not only from younger donors, but also potentially from healthier knees. Knees with any significant pathologic change are not processed for implantation. Before surgery, the knees of our patient population were subject to a multitude of potentially damaging forces associated with a variety of comorbidities. These pathologic forces degrade the homeostasis of the recipient knees. Instability, enzymatic degradation from exposed subchondral bone, the effect of loose bodies, vascular compromise associated with osteochondritis dissecans, and meniscal tears all serve to degrade the host cartilage before allograft implantation. Another possible factor leading to ambient cartilage degradation is underlying chondrosis of a genetic variety. Perhaps there was a predisposition to cartilage damage in certain patients. All these factors would offer a potential explanation for the relative success of the fresh-stored osteochondral grafts compared with the native cartilage in these patients.
The small study population of 8 patients and 10 knees has been demonstrated to be reflective at several levels of the larger patient population of 67 patients from which this small subgroup was recruited. Demographic data including age, gender, time between graft harvest and implantation, graft size, and IKDC scores were all similar when comparing these 2 populations. While the study would have been strengthened to gather detailed information, including second-look biopsy data on all 67 patients, this is simply not practical in the context of an invasive follow-up methodology.
There are several limitations of the current study. This study was retrospective, which precluded analysis of the graft tissue at the time of implantation. Analysis was undertaken in a non-andomized, limited number of patients. This important constraint reflects the intrinsic difficulty of performing invasive analysis on patients who are generally doing well. We attempted to limit selection bias in this study population by sequentially recruiting volunteers to undergo further study once they were approximately a minimum of 2 years from index surgery. There exists a potential selection bias, insofar as we have recruited sequentially to participate in this study; of the 14 patients solicited, 6 declined to participate. The reasons for declining participation were varied, but mostly they thought they were doing well and did not want to have an invasive procedure. Of the 8 patients that accepted participation in the study, to provide 10 knees for analysis, the majority were simply curious as to the graft status and function of their knee(s) after having undergone an extensive reconstructive surgery. A larger cohort would have enabled more powerful statistical analysis of multiple variables. Analysis of the grafts could have included intraoperative quantified stiffness analysis, but unfortunately that equipment was not available for our use. Additionally, we chose to evaluate chondrocyte viability and density, but we did not perform any analysis of cartilage metabolism or matrix sulfated glycosaminoglycan content. Future studies should certainly include those data. Lastly, longer follow-up is needed to determine whether an important goal of cartilage restoration is actually achieved, namely prevention of future degenerative changes and avoidance of early arthroplasty.
Conclusion
Our data indicate that osteoarticular allografts hypothermically stored 4 weeks or longer successfully improved the measured clinical, histologic, and MRI parameters over a mean 40-month follow-up period. In this series, hypothermically stored osteochondral allografts have successfully achieved several goals of biological restoration of full-thickness cartilage defects of the distal femur. Specifically, we have demonstrated diminished pain, increased function, restoration of functional histologic architecture, and prevention of short-term degenerative change. Further study will determine whether prevention of long-term degeneration and avoidance of early arthroplasty can be achieved with this procedure.