
Abstract
Background: Restoring the anatomical footprint may improve the healing and mechanical strength of repaired tendons. A double row of suture anchors increases the tendon-bone contact area, reconstituting a more anatomical configuration of the rotator cuff footprint.
Hypothesis: There is no difference in clinical and imaging outcome between single-row and double-row suture anchor technique repairs of rotator cuff tears.
Study Design: Randomized controlled trial; Level of evidence, 1.
Methods: The authors recruited 60 patients. In 30 patients, rotator cuff repair was performed with a single-row suture anchor technique (group 1). In the other 30 patients, rotator cuff repair was performed with a double-row suture anchor technique (group 2).
Results: Eight patients (4 in the single-row anchor repair group and 4 in the double-row anchor repair group) did not return at the final follow-up. At the 2-year follow-up, no statistically significant differences were seen with respect to the University of California, Los Angeles score and range of motion values. At 2-year follow-up, postoperative magnetic resonance arthrography in group 1 showed intact tendons in 14 patients, partial-thickness defects in 10 patients, and full-thickness defects in 2 patients. In group 2, magnetic resonance arthrography showed an intact rotator cuff in 18 patients, partial-thickness defects in 7 patients, and full-thickness defects in 1 patient.
Conclusion: Single- and double-row techniques provide comparable clinical outcome at 2 years. A double-row technique produces a mechanically superior construct compared with the single-row method in restoring the anatomical footprint of the rotator cuff, but these mechanical advantages do not translate into superior clinical performance.
Arthroscopic management of rotator cuff tears has evolved from simple debridement to arthroscopic repair providing anatomical reconstruction.3-6,15 Restoring the anatomical footprint may improve the healing and mechanical strength of repaired tendons. 2 A single row of suture anchors may not be effective for this purpose. A double row of suture anchors increases the tendon-bone contact area, reconstituting a more anatomical configuration of the rotator cuff footprint. 12
We evaluated the results of a randomized controlled trial of arthroscopic repair in patients with large and massive rotator cuff tears in whom the repair was effected using a single- or double-row arthroscopic technique.
Materials and Methods
Our institutional review board approved the study, and all patients gave written informed consent to participate in this clinical trial.
Eligibility Criteria
Patients were included in the study if they had a rotator cuff tear diagnosed on clinical grounds, no episodes of shoulder instability, no radiographic signs of fracture of the glenoid or the greater or lesser tuberosity, MRI evidence of cuff tear, duration of symptoms of at least 3 months, inadequate response to nonoperative management (including nonsteroidal anti-inflammatory drugs, physical therapy, rest, and 1 local corticosteroid injection), and an unretracted and sufficiently mobile full-thickness rotator cuff lesion to allow a double-row repair found at the time of surgery.
Patients were excluded from the study if they had inflammatory joint disease, retracted and insufficient mobile lesions to allow a double-row repair found at the time of surgery, prior surgery on the affected shoulder, or inability to complete questionnaires because of language problem or cognitive disorder.
Recruitment and Randomization
Patients were recruited among those referred by primary care doctors because of symptoms of rotator cuff tears. Eligible patients were enrolled by the examining orthopaedic surgeon. Each patient was given full verbal and written information about the trial, and written informed consent was obtained by the operating surgeon.
Recruitment started in February 2004 and was completed in September 2004. Of 197 patients screened for eligibility, 60 patients were eligible and were randomized: 30 patients to single-row anchor repair and 30 patients to double-row anchor repair. All patients received the allocated treatment.
Of 60 participants randomized to 1 of the 2 treatments, 2-year results were available for 52. Eight patients (4 in the single-row anchor repair group and 4 in the double-row anchor repair group) did not return at the final follow-up (Figure 1).
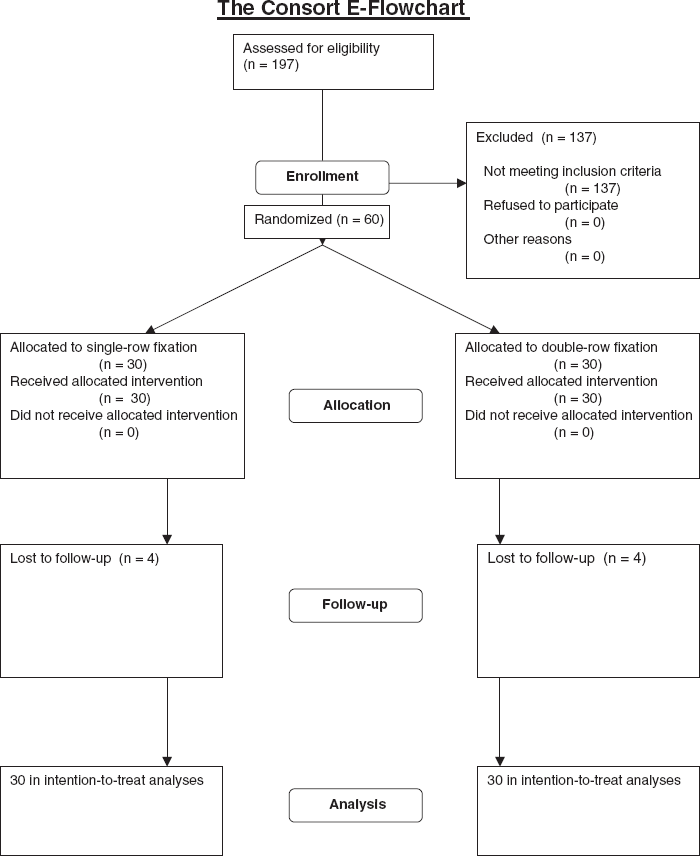
Patients’ consort statement.
Evaluation
We performed preoperative evaluations the day before surgery and reported the results of postoperative evaluation at a final follow-up mean of 22.5 months (range, 18-25 months) from the operation. Each patient was evaluated for arm dominance, trauma history, duration and type of preoperative symptoms, type of lesion, preoperative and postoperative range of motion (ROM), and preoperative and postoperative modified shoulder score (University of California, Los Angeles [UCLA]).
Imaging
All patients received a standard preoperative assessment using standard radiographs (anteroposterior projections; neutral, external, and internal rotation; a lateral view of the scapula; and an axillary view) and MRI scans. Oblique coronal, oblique sagittal, and axial T2-weighted spin-echo MRIs (repetition time, 3200 milliseconds; echo time, 85 milliseconds) were obtained in all patients.
All patients received a postoperative MR arthrography at the final follow-up appointment. The joint was injected with 1.5 mL of gadolinium and 8.5 mL of normal saline solution under fluoroscopic control. The MRI was performed with a 1.5-T scanner. We employed T2-weighted, gradient echo spectral presaturation inversion recovery sequences in true axial scans and T1-weighted, gradient echo spectral presaturation inversion recovery sequences in oblique coronal planes that were parallel to the course of the supraspinatus muscle and oblique sagittal planes that were parallel to the glenoid fossa. Imaging time was approximately 18 minutes. All MR arthrography was performed and evaluated by the same fully trained board-certified radiologist with a special interest in musculoskeletal imaging.
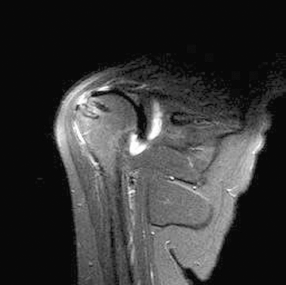
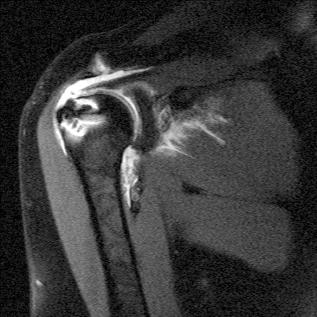
The rotator cuff was reported as intact (Figure 2) or torn using previously published MR arthrography criteria. Partial tears (Figure 3) were diagnosed in the presence of contrast fluid signal filling a partial tendon defect. Full-thickness tears (Figure 4) were diagnosed in the presence of extravasation of contrast material to the subacromial-subdeltoid space.14,17,22

Coronal T1-weighted image showing intact tendon after single-row repair.
Coronal T1-weighted image showing partial rotator cuff tear with delamination. Note the absence of contrast material in the subacromial-subdeltoid space after double-row repair.
Coronal T1-weighted image showing a moderate fluid accumulation in the subacromial-subdeltoid bursa, a finding indicative of a full-thickness tear at the attachment site after double-row repair.
Functional Assessment
A modified UCLA 7 shoulder rating scale was used to evaluate preoperative and postoperative shoulder pain, function and ROM, strength, and patient satisfaction. The maximum score obtainable is 35, and the results were classified as excellent (34-35 points), good (28-33), fair (21-27), or poor (0-20).
Range of Motion
A standard universal goniometer was used for measurement with scales marked in 1° increments. Patients were positioned supine on an examining couch with the shoulder at 90° of abduction in the scapular plane (approximately 15° anterior to the coronal plane). Measurement of supine forward elevation (sagittal plane) and internal and external rotation (90° of abduction) was obtained using standard measurement guidelines. 1 Care was taken to fix the scapula with one hand while the examiner's other hand rotated the shoulder into position. One examiner (L.R.) held the shoulder position while a second examiner (U.G.L.) obtained the measurement after a firm endpoint was established. The forearm was held in neutral rotation during rotational measurement. Three measurements were taken for each shoulder, and the mathematical mean was used for statistical purposes.
Randomization Procedure
After a diagnostic arthroscopy assessing the status of the shoulder joint and the presence and size of the rotator cuff tear, we ascertained whether the tear was mobile evaluating the medial-to-lateral and anterior-to-posterior mobility of the tear margins with a soft tissue grasper. If this was the case, at that stage, patients were randomized into 1 of 2 groups, to receive either a single-row suture anchor repair technique (group 1) or a double-row suture anchor repair technique (group 2).
We used a random-numbers table to allocate subjects. Starting with an arbitrary point in the table, we selected 52 sequential random numbers. The first 26 numbers were assigned to the single-row group, and the next 26 were assigned to the double-row group. These assignments were then arranged in an ascending order. This procedure produced a random sequence of consecutive treatment allocations. Sealed, opaque numbered envelopes containing the treatment assignments were prepared, with care being taken to make sure that the order of the envelopes exactly matched the allocation schedule.
All surgical interventions were performed by the same surgeon (F.F.). After diagnostic arthroscopy, the extent of the tear was assessed, the tendon margins were debrided, and a bone bed was prepared by means of a power shaver so as not to decorticate the bone. The rotator cuff tears were classified according to the size, shape, and location. At that time, the envelope was opened, and the patient was allocated to either group 1 (single row) or group 2 (double row).
In group 1 (single-row suture anchor repair technique), there were 12 men and 14 women (mean age, 63.5 years; range, 43-76 years). The dominant arm was affected in 20 patients. The rotator cuff tear was large (3-5 cm) in 18 patients and massive (>5 cm) in 8 patients. There were 12 crescent lesions, 4 L-shaped lesions, and 10 U-shaped lesions. The tear involved the supraspinatus tendon in 12 patients, the supraspinatus and infraspinatus tendons in 11 patients, and the supraspinatus and subscapularis tendons in 3 patients.
In group 2 (double-row suture anchor repair technique), there were 16 men and 10 women (mean age, 59.6 years; range, 45-80 years). The dominant arm was affected in 19 patients. The rotator cuff tear was large (3-5 cm) in 21 patients and massive (>5 cm) in 5 patients. There were 14 crescent lesions, 6 L-shaped lesions, and 6 U-shaped lesions. The tear involved the supraspinatus tendon in 15 patients, the supraspinatus and infraspinatus tendons in 9 patients, and the supraspinatus and subscapularis tendons in 2 patients.
Arthroscopic Technique
Patients underwent brachial plexus block, associated in 7 cases with general anesthesia, and were placed in a lateral decubitus position. The arm was suspended at approximately 45° of abduction and 20° of forward flexion. Distraction of the shoulder joint was accomplished with 4.5 to 6.5 kg of traction. Four to 6 portals were used. A posterior portal was produced, and the arthroscope was inserted into the glenohumeral joint. A diagnostic arthroscopy was then performed to evaluate the extent of the rotator cuff tear, any lesions of the biceps tendon, and other associated lesions. The main subacromial portals were the posterolateral viewing, the anterolateral, and the lateral working portal, with an 8.25-mm cannula. To control bleeding, we used radiofrequency, adrenalin admixture to the irrigation fluid and asked the anesthesiologist to lower the systolic blood pressure to 90 mm Hg if possible. An arthroscopic pump maintained fluid pressure at 40 mm Hg, increasing it temporarily on demand.
A spinal needle was introduced percutaneously to determine the precise location for placement of the anterolateral portal produced approximately 2 to 3 cm anterior and lateral to the anterolateral corner of the acromion. If the subscapularis tendon was involved, an anterior midlateral portal was produced just superior to the lateral half of the subscapularis tendon. The lateral portal was used to mobilize the rotator cuff back to its bony insertion. The mobility of the rotator cuff was assessed. The footprint of the greater tuberosity was abraded by a bur through the lateral portal.
The single-row anchor repair was performed by placing 1 row of suture anchors double loaded with No. 2 Fiberwire (Biocorkscrew, Arthrex, Naples, Fla) just inside the lateral aspect of the footprint. Both sutures were passed through the tendon in a mattress fashion.
The double-row anchor repair technique was performed as described previously. 12 Briefly, 1 row of anchors was placed in the medial aspect of the footprint, just lateral to the articular surface of the humeral head. Both sutures were passed through the tendon in a mattress fashion. A lateral row of anchors was then placed on the lateral aspect of the footprint, slightly proximal to the greater tuberosity (Figure 5). The lateral row sutures were passed in a simple suture fashion. Just 1 of the 2 sutures was passed through the tendon. The anchors used were Biocorkscrew (Arthrex) double loaded with No. 2 Fiberwire (Arthrex).
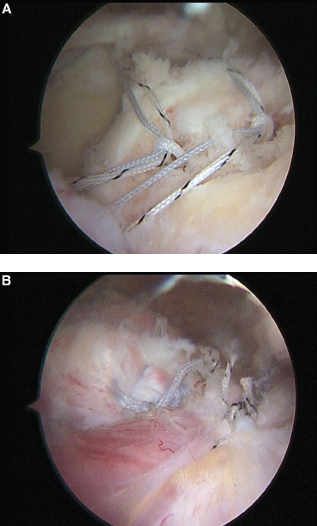
A, arthroscopic view from a posterolateral portal showing the insertion of medial and lateral double-loaded anchors adjacent to the articular margin of the humeral head. B, arthroscopic view from a posterolateral portal showing a completed double-row repair after knot tying.
The number of suture anchors varied with the size of the tear and the type of repair techniques; we used 1.9 (range, 1-2) anchors in group 1 (single row) and 2.3 anchors (range, 2-4) in group 2 (double row).
The L-shaped and U-shaped tears were first repaired with a side-to-side suture, providing margin convergence of the 2 edges of the cuff, before fixation of the cuff to bone.
Postoperative Management
Postoperative management was the same for both groups. The arm was supported using a sling with an abduction pillow for 6 weeks. Active elbow flexion and extension were allowed, but terminal extension was restricted. Passive external rotation was started from the first day after surgery and maintained within a comfortable range. Overhead stretching was restricted until 6 weeks postoperatively to avoid damaging the repair. At 6 weeks, the sling was removed, and overhead stretching with a rope and pulley was started. Isoinertial strengthening and rehabilitation of the rotator cuff, deltoid, and scapular stabilizers were initiated at 10 or 12 weeks after the operation. Rehabilitation was continued for 6 months. Heavy manual work and overhead activities were allowed after a good restoration of shoulder strength, which occurred 6 to 10 months after surgery.
Statistics
Statistical analyses were blinded and performed according to the intention-to-treat principle. Descriptive statistics were calculated. The results of surgery in the 2 groups were compared using the Wilcoxon signed rank test. Significance was set at P < .05.
Results
The mean operative time for group 1 patients (single-row suture repair) was 42 ± 18.9 minutes (range, 35-64 minutes). The mean operative time for group 2 patients (double-row suture repair) was 65 ± 23.4 minutes (range, 45-87 minutes). The difference was statistically significant (P = .005). No infection or neurological or vascular complications were experienced.
Group 1
The UCLA rating system showed a statistically significant improvement from a preoperative mean rating of 11.5 (range, 6-14) to a mean of 32.9 (range, 29-35) postoperatively (P < .05). Forward flexion averaged 110° (range, 30°-140°) preoperatively and 159° (range, 150°-170°) at final follow-up (P < .05). The mean external rotation improved from 83.2° (range, 65°-95°) preoperatively to 132.4° (range, 90°-140°) at final follow-up (P < .05). Internal rotation increased from a mean of 27.3° (range, 20°-33°) preoperatively to a mean of 37.3° (range, 27°-42°) at final follow-up (P < .05) (Table 1).
Clinical Findings a
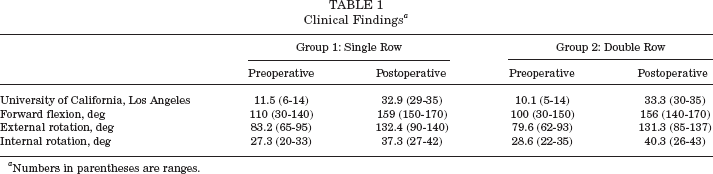
Numbers in parentheses are ranges.
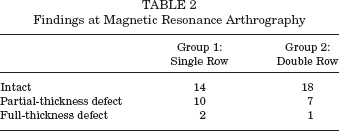
Postoperative MR arthrography examination at 2-year follow-up showed intact tendons in 14 patients, partial-thickness defects in 10 patients, and full-thickness defects in 2 patients (Table 2).
Findings at Magnetic Resonance Arthrography
Group 2
The UCLA rating system showed a statistically significant improvement from a preoperative mean rating of 10.1 (range, 5-14) to a mean of 33.3 (range, 30-35) postoperatively (P < .05). Forward flexion averaged 100° (range, 30°-150°) preoperatively and 156° (range, 140°-170°) at final follow-up (P < .05) (Table 1).
The mean external rotation improved from a mean value of 79.6° (range, 62°-93°) preoperatively to 131.3° (range, 85°-137°) postoperatively (P < .05). Internal rotation increased from a mean of 28.6° (range, 22°-35°) preoperatively to a mean of 40.3° (range, 26°-43°) at final follow-up (P < .05).
Postoperative MR arthrography at final follow-up showed an intact rotator cuff in 18 patients, partial-thickness defects in 7 patients, and full-thickness defects in 1 patient (Table 2).
There were no statistically significant differences in rates of healing between Group 1 and Group 2 patients when assessed by MRI arthrography (P > .05). There was no statistically significant difference in total postoperative UCLA scores when comparing single-row suture anchor repairs to double-row suture anchor repairs. The ROM did not differ between the 2 groups: it improved in all the directions measured (P > .05).
Discussion
We compared the clinical and imaging outcome of large and massive rotator cuff tears repaired arthroscopically using a standard single- or double-row technique. In our hands, the single- and double-row techniques provide comparable clinical outcomes. Compared with the single-row method, a double-row technique produces a mechanically superior construct in restoring the anatomical footprint of the rotator cuff, but these mechanical advantages do not translate to superior clinical performance.
To our knowledge, this is the first randomized controlled trial to compare the outcome of arthroscopic single-row or double-row anchor suture repair rotator cuff surgery using both clinical and imaging criteria. We acknowledge that we did not perform a formal power analysis, and that we planned the choice of the number of patients to enroll in the study according to what we knew our unit could deliver within the time we chose to allocate to the study. However, despite this partial weakness of the present investigation, our selection and recruitment process, our assessment criteria, and our follow-up were extremely rigorous, and performed in strict scientific fashion. Also, with the numbers of patients enrolled, the results of our study are unequivocal.
We used MR arthrography to evaluate the anatomical appearance after operative rotator cuff repair because this technique affords several advantages over conventional MRI, including better definition of the rotator cuff and tendon defects and a better differentiation of rotator cuff degeneration from partial or complete rotator cuff tears. 16 Other strengths of this study include the use of a single surgeon and its prospective randomized nature.
We followed up patients clinically and with imaging for 22.5 months. Although this may be considered a relatively short time, we believe that by then the results of surgery would have stabilized and recovery effected. Also, this length of follow-up was chosen because we wished to minimize the number of patients defaulting from the study; we thought that it would have been difficult to ask patients to return for assessment several years later for clinical assessment and imaging.
It is difficult to compare the findings of the present study with those of previous reports, as we know of no other prospective studies performed using MR arthrography to compare the clinical and anatomical outcomes of large and massive rotator cuff tears repaired arthroscopically using single- or double-row anchors.
Biomechanical studies comparing single- and double-row suture anchor techniques for rotator cuff repair show that a double row of suture anchors increases the tendon-bone contact area and restores the anatomical rotator cuff footprint, 12 providing a better environment for tendon healing (S. W. Meier et al, unpublished data, 2004). 2
The transosseous technique and the arthroscopic single-row fixation technique restore 85% and 65%, respectively, of the normal surface area, failing to restore the normal footprint of the supraspinatus tendon to the greater tuberosity. 2 Double-row suture anchor fixation fully reproduces the original supraspinatus footprint,11,13 decreases the gap formation and strain over the footprint, and improves its initial strength and stiffness when compared with a conventional single-row repair. 18 Single-row repairs were similar to double-row repairs in load to failure, cyclic displacement, and gap formation. 13
In comparative retrospective studies, the clinical outcomes of single-row and double-row anchor suture technique were comparable, although rotator cuff integrity was more likely to be maintained with double-row repair. 21 Sugaya et al 18 performed the above study using MRI, which is sensitive and specific for diagnosis of full-thickness tears but has a sensitivity of only 20% for partial-thickness tears. 16 Instead, MR arthrography is more sensitive for this purpose. 16
Rotator cuff surgery aims to provide tendon fixation secure enough to hold the repaired tendon in place until biological healing occurs.3-6,9 Several factors may be implicated in failure of rotator cuff repairs, including suture or knot failure, inadequate tendon-to-bone fixation, and lack of tendon-to-bone healing.8,10,20 As we reinsert tendinous tissue into bone, theoretically, only the reconstitution of enthesial fibrocartilage can guarantee an optimal outcome. 19
The concept of restoration of the anatomical footprint is appealing, but we did not find any statistical difference between the 2 techniques. Also, double-row repair requires longer surgical time, is more expensive as a greater number of suture anchors is required, and may well be technically more demanding.
In conclusion, our study shows that there are no advantages in using a double-row suture anchor technique to restore the anatomical footprint. The mechanical advantages evidenced in cadaveric studies do not translate into superior clinical performance when compared with the more traditional, technically less demanding, and economically more advantageous technique of single-row suture anchor repair.