
Abstract
Background: Several previous studies have described reconstructive methods for the treatment of an injury to the ulnar collateral ligament of the thumb. However, there are few biomechanical studies to date to analyze the strength of the surgical reconstruction.
Purpose: To evaluate 2 reconstruction techniques with use of a cadaveric model: (1) reconstruction with the use of a free tendon graft placed in a figure-of-8 fashion through drill holes in the metacarpal and proximal phalanx of the thumb, and (2) reconstruction with the use of the Bio-Tenodesis Screw System.
Study Design: Controlled laboratory study.
Methods: Eight matched pairs of cadaveric specimens underwent removal of the proper and accessory ulnar collateral ligaments. One of the 2 reconstruction methods was performed, and specimens were mounted on a materials-testing machine. The specimens were subjected to valgus stress to failure at 30° of flexion. Failure was defined as valgus laxity of 30° at the metacarpophalangeal joint.
Results: The peak load to failure was 23.5 ± 11.4 N for the figure-of-8 reconstruction and 24.3 ± 12.3 N for the reconstruction using the Bio-Tenodesis Screw System. Comparing the 2 groups, there was no statistically significant difference in peak loads to failure (P = .88).
Conclusion: There was no statistically significant difference between the peak loads to failure of the 2 reconstructions.
Clinical Relevance: The Bio-Tenodesis Screw System may provide another viable option for surgical reconstruction of the ulnar collateral ligament of the thumb.
Injury of the ulnar collateral ligament of the first metacarpophalangeal joint is a common injury often caused by excessive radial deviation of the thumb proximal phalanx.4,5,22,23 In 1955, Campbell 3 coined the eponym “gamekeeper's thumb” to describe the chronic laxity of the ulnar collateral ligament. The name is derived from a condition commonly associated with European gamekeepers. Gamekeepers repetitively killed their game by grasping the head of the animal between the thumb and index finger to break the animals’ necks. These acts resulted in a chronic pattern of injury to the ulnar collateral ligament of the thumb of the gamekeepers. In 1981, Gerber et al 9 used the phrase “skier's thumb” to describe an acute injury of the ulnar collateral ligament because of the high prevalence seen in that sport. When a skier falls with his or her hand caught in a ski pole or planted into the snow, the thumb's ulnar collateral ligament may sustain significant stresses. In 1962, Stener 23 described a lesion observed in many cases of complete rupture of the ulnar collateral ligament of the thumb. Stener lesions are an adductor aponeurosis interposition between the distally avulsed ulnar collateral ligament and the ligament's insertion into the base of the proximal phalanx of the thumb. 23 Stener concluded that failed ligament healing would result from a lack of contact at the site of ligament rupture and that such complete ruptures necessitated surgical repair.
The Bio-Tenodesis Screw System (Arthrex, Naples, Fla) is a bioabsorbable construct that eliminates the need for transosseous tunnels in ligament reconstruction and tendon repair. Bio-Tenodesis screws have been used successfully in proximal and distal biceps tendon repairs as well as ligament reconstruction in the ankle.14,16 Previous biomechanical studies have shown that the peak load to failure of the Bio-Tenodesis Screw System was nearly twice that of suture anchors in ligament reconstruction. 13 The Bio-Tenodesis Screw System employs a bone socket into which the tendon graft and a bioabsorbable interference screw are inserted. The recent development of smaller screws provided another surgical option for ligament reconstruction in the hand.
To date, there are no published data on the biomechanical strength of ligamentous reconstruction of the ulnar collateral ligament of the thumb. The purposes of this study were to determine the peak load to failure of an existing reconstructive method using bone tunnels and a figure-of-8 tendon weave and to investigate a new technique for ligamentous reconstruction with the use of the Bio-Tenodesis Screw System. This study tested the hypothesis that there was no significant difference in loads to failure between the 2 methods.
Materials and Methods
Eight matched pairs of human cadaveric upper extremities were frozen at –20°C. The specimens were obtained from 6 male and 2 female donors who had a mean age of 60 years (range, 50-68 y) at the time of death. The cadaveric specimens were thawed in a warm water bath 1 hour before preparation. The extensor indicis proprius tendon was harvested and set aside for later use. The thumb ray to the carpometacarpal joint was isolated. The skin and subcutaneous tissue were removed from the first metacarpophalangeal joint preserving the volar plate, the joint capsule, and the collateral ligaments. The proper and accessory ulnar collateral ligaments were then removed.
The thumb rays, right and left, were randomly assigned to 1 of 2 groups. The first group consisted of 8 reconstructions using a standard figure-of-8 tendon weave as described by Hsieh et al. 12 Three-millimeter holes were drilled into the locations of the ulnar collateral ligament's insertions onto the proximal phalanx and onto the metacarpal. Additional holes were drilled approximately 10 mm volar to the metacarpal hole and approximately 10 mm dorsal to the hole in the proximal phalanx. The 2 holes in each bone were connected using curettes while taking care to preserve the bony bridge. The extensor indicis proprius tendon graft was guided through the osseous tunnels and weaved in a figure-of-8 configuration (Figure 1). The graft was tensioned and sutured to itself using 3-0 Ethibond suture (Ethicon, Somerville, NJ).
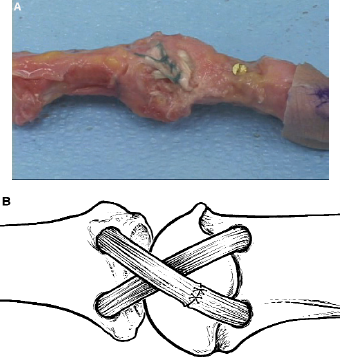
Ulnar collateral ligament reconstruction using the figure-of-8 technique. A, photograph; B, drawing.
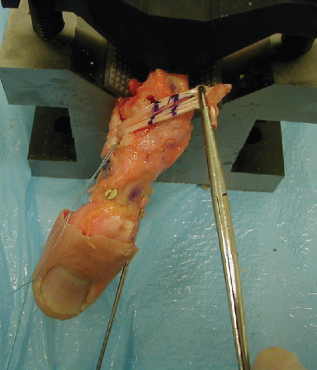
The second group consisted of 8 reconstructions using the Bio-Tenodesis Screw System. Holes were drilled at the locations of the insertions of the proper collateral ligament onto the first proximal phalanx and onto the first metacarpal (Figure 2). The holes had a diameter of 4 mm and a depth of 10 mm. The tendon graft was doubled, and a running, locking stitch was placed on 1 end using a 2-0 FiberWire suture (Arthrex). Different sutures were used in the 2 experimental groups to re-create the clinical scenario of ulnar collateral ligament reconstruction: the Bio-Tenodesis screw is provided with 2-0 FiberWire suture, and the figure-of-8 reconstruction may be achieved using 3-0 Ethibond suture. The graft in the second experimental group was fixed to the proximal phalanx using a Bio-Tenodesis screw. The proximal phalanx was reduced, and a mark was made on the graft at the tunnel opening on the metacarpal. Approximately 8 mm distal to this first mark on the graft, another mark was made to allow the graft to be seated at the bottom of the tunnel before screw insertion (Figure 3). A running, locking suture was placed between the 2 aforementioned marks, and the excess tendon length was excised. A Bio-Tenodesis screw was then inserted into the metacarpal head while applying tension to the graft (Figure 4).

Drill holes before graft insertion.
Graft marked at the appropriate length at the entrance of the tunnel.
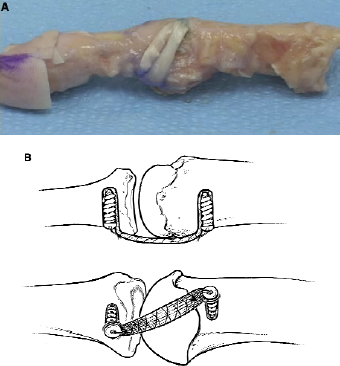
Ulnar collateral ligament reconstruction using the Bio-Tenodesis Screw System. A, photograph; B, drawing.
The specimens were loaded onto an apparatus for biomechanical testing (Figure 5). The samples were loaded at a point 2 cm distal to the metacarpophalangeal joint. This point of loading was selected because it was easily reproducible in the specimens by measuring with a caliper and because of correlation with the clinical scenario. The specimens were secured to the fixture in the appropriate orientation on a materials testing system (MTS Systems, Eden Prairie, Minn). Valgus load was applied to the metacarpophalangeal joint with the joint flexed to 30°. Flexion was maintained to isolate the valgus load on the ulnar collateral ligament. 7 The tensile load was applied at a rate of 0.1 mm/s. 7 This rate was chosen to simulate the loading rate experienced during a rehabilitation protocol. 7 The specimens were loaded to failure. When the ulnar collateral ligament is ruptured in the clinical setting, the metacarpophalangeal joint reveals valgus laxity of 30° or greater. Thus, reconstruction failure in this study was defined as valgus laxity of 30° at the metacarpophalangeal joint. Using a protractor, the failure angle was measured between the metacarpal and proximal phalanges at the time of ulnar collateral ligament reconstruction failure. Using the load displacement curve, the load required to produce 30° of deflection was recorded. The mechanism of failure was also recorded.
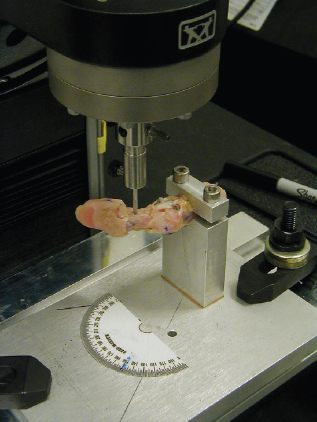
A specimen mounted in the testing fixture.
The data were analyzed using a paired, 2-tailed Student t test for comparison between the groups at a confidence level of P < .05 to determine significant differences in peak load to failure between the 2 reconstructions.
Results
The mean peak load of the figure-of-8 reconstruction group was 23.5 ± 11.4 N. The mean peak load of the Bio-Tenodesis reconstruction group was 24.3 ± 12.3 N. In 5 specimens—4 from the Bio-Tenodesis group and 1 figure-of-8 reconstruction—the grafts stretched beyond 30°; however, the load at 30° was used as the peak load. Comparing the 2 groups, there was no statistically significant difference in peak load to failure (P = .88).
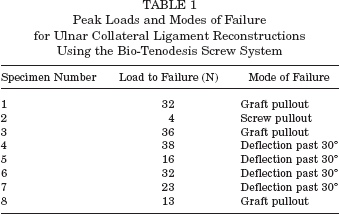
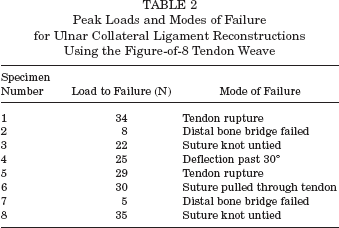
The most common mode of failure in the Bio-Tenodesis group was stretching of the graft beyond 30° (Table 1). Other causes of failure were graft pullout and screw pullout. The figure-of-8 reconstructions displayed more diverse modes of failure, including fracture of the bone bridge, suture breakage, extensor indicis proprius tendon rupture, and tendon stretch (Table 2).
Peak Loads and Modes of Failure for Ulnar Collateral Ligament Reconstructions Using the Bio-Tenodesis Screw System
Peak Loads and Modes of Failure for Ulnar Collateral Ligament Reconstructions Using the Figure-of-8 Tendon Weave
Discussion
A variety of surgical techniques have been described for the reconstruction of the ulnar collateral ligament of the thumb. These techniques may be divided into static and dynamic reconstructions. Dynamic reconstructions have included a dynamic tendon transfer to replace the incompetent ulnar collateral ligament as well as those involving capsulorrhaphy and adductor advancement.17,19 The descriptions of static reconstructions have included the use of static tendon transfers or free tendon grafts.2,6,8,10,18,20–22,24 The reports on the use of free tendon grafts are varied with a number of different reconstructive techniques used. Previously described reconstructive techniques have included the use of a single hole in the proximal phalanx with a pullout wire to secure the graft, multiple drill holes in the proximal phalanx, and grafts secured with suture anchors.10,18,22
This study explored reconstruction of the ulnar collateral ligament of the thumb metacarpophalangeal joint using a Bio-Tenodesis Screw System. Surgical reconstruction recently has become the focus of several biomechanical studies. The importance of achieving an anatomic reconstruction was confirmed by Bean et al 1 as nonanatomic reconstruction of the ulnar collateral ligament altered normal metacarpophalangeal joint range of motion. Lee et al 15 showed that reconstruction tunnel position of a triangular configuration with the apex proximal was optimal for stabilization of the metacarpophalangeal joint while preserving range of motion. After comparing several methods for reconstruction, Hogan et al 11 concluded that anatomic reconstruction with interference knot fixation of the tendon graft displayed better strength and stiffness characteristics.
This study represents biomechanical data on ligament reconstruction of the ulnar collateral ligament of the thumb. The failure load of the intact ulnar collateral ligament of the metacarpophalangeal joint of the thumb is 294.3 ± 28.2 N. 7 In a previous study, Firoozbakhsh et al 7 reported that the failure load of the repaired ulnar collateral ligament using a mini-Mitek bone suture anchor was 43.8 ± 6.2 N · cm/mm. In this study, the mean peak load to failure of the figure-of-8 reconstruction was 23.5 ± 11.4 N. Thus, the strength of current ulnar collateral repairs and the strength of ulnar collateral ligament reconstruction methods are inferior to native ulnar collateral ligaments. In addition, these findings impart the importance of consideration for surgical repair in the setting of an acute ulnar collateral ligament rupture. These results also support the need for postoperative immobilization and emphasize the need to develop stronger reconstruction techniques. Improved reconstructions may allow patients to receive a shorter duration of postoperative immobilization and subsequently yield a faster return to daily activities.
This cadaveric biomechanical study had several limitations. The age of the specimens may have affected the composition of osseous and soft tissue structures, especially when compared with the younger patient population in whom ulnar collateral ligament injuries may be more likely to occur. In addition, the loads imparted may not have simulated the precise stresses on the first metacarpophalangeal joint during normal activities of daily living or traumatic incidents. Furthermore, peak load to failure may not predict reliably the ultimate strength of the reconstruction after healing occurs. Cyclic loading may better mimic repetitive stresses encountered by the reconstruction in daily life; however, peak loads were employed to reproduce the adverse effects of a traumatic episode. Different sutures were used in the experimental groups to replicate the clinical scenario. No failures in either cohort were due to suture breakage. However, failures in the figure-of-8 group were related to the suture pulling through the tendon and the suture knot untying. Use of different suture materials may have altered the results. Finally, the use of the Bio-Tenodesis Screw System for ulnar collateral ligament reconstruction may prove more technically difficult than the standard figure-of-8 reconstruction.
Despite these shortcomings, reconstruction with the Bio-Tenodesis Screw System did not exhibit a significant difference in peak load to failure when compared with figure-of-8 reconstruction. Further studies are necessary to qualify the utility of this recently developed technique. Thus, the Bio-Tenodesis Screw System may provide another viable option for surgical reconstruction of the ulnar collateral ligament of the thumb.