
Abstract
Background: Fixation of an anterior cruciate ligament graft at the joint line with an interference screw restores anterior laxity better than low-stiffness distal fixation with double staples and sutures tied to a post at implantation in porcine bone.
Hypothesis: Fixation of an anterior cruciate ligament graft with a high-stiffness distal fixation device restores anterior laxity and knee stiffness as well as joint line fixation with an interference screw in human bone.
Study Design: Controlled laboratory study.
Methods: Eleven cadaveric knees with foam reinforcement of the bone were reconstructed with a double-looped tendon graft and fixed with an interference screw and 3 high-stiffness methods of fixation (tandem washer, WasherLoc, and WasherLoc with bone dowel). Anterior laxity at 225 and 110 N of anterior load and knee stiffness were measured at 0°, 30°, 60°, 90°, and 120° of flexion with a 6 degrees of freedom load application system.
Results: The increase in anterior laxity and knee stiffness with the interference screw was not significantly different from that with the high-stiffness distal methods.
Conclusion: In the human knee, the use of high-stiffness fixation devices placed distal to the joint line restored anterior laxity and knee stiffness as well as joint line fixation with an interference screw at implantation.
Clinical Relevance: The stiffness provided by each method of fixation should be considered along with the length of the graft when determining anterior laxity and knee stiffness.
Keywords
Proponents of fixation of an ACL graft at the joint line with an interference screw base their opinions on several studies.19,30,31,33,40 The seminal study, in porcine knees, showed better restoration of anterior laxity with joint line fixation with an interference screw than with double staples inserted distal to the tibial tunnel. 19 A subsequent study in human knees showed better restoration of anterior laxity with an interference screw than with sutures tied to a post inserted distal to the tibial tunnel. 33 The explanation offered for the better restoration of anterior laxity with joint line fixation with an interference screw over distal fixation with double staples and sutures tied to a post was that joint line fixation shortens the effective length of the graft, which increases the stiffness of the knee.19,31,33
There is no dispute that a shorter graft is stiffer than a longer graft is, as long as the grafts have the same cross-sectional area. However, the addition of fixation devices in series with the graft might profoundly affect the overall stiffness of the graft–fixation device complex. Therefore, the stiffness provided by each of the fixation devices might be an important factor to consider along with the length of the graft when determining the overall stiffness of the graft– fixation device complex and when determining how well the complex restores anterior laxity and knee stiffness.
Our interpretation of more recent studies suggests that the decision to use double staples, 19 sutures tied to a post, 33 and porcine knees 24 32 in the evaluation of the effect of the level of fixation on the restoration of anterior laxity and knee stiffness might have unintentionally overestimated the importance of joint line fixation because they did not consider the effect of the stiffness of the fixation method and the type of bone. To our knowledge, the restoration of anterior laxity with an interference screw has only been compared with low-stiffness distal fixation devices (ie, <200 N/mm), which include double staples (174 N/mm) 19 and sutures tied to a post (70 N/mm). 33 The restoration of anterior laxity with an interference screw has not been compared with high-stiffness distal fixation devices (>400 N/mm) such as tandem screws and washers (414 N/mm), WasherLoc (506 N/mm), and WasherLoc and bone dowel (565 N/mm). 18 24 The use of high-stiness distal fixation devices might restore anterior laxity as well as an interference screw fixation does because they are 22% to 66% stiffer than is an interference screw in young human tibia (340 N/mm). The greater stiffness of high-stiffness distal fixation devices might offset the decrease in stiffness from the use of a graft with a longer effective length and restore anterior laxity and knee stiffness just as effectively.
The results from 2 other more recent studies suggest that the use of porcine knee by Ishibashi et al 19 might not have been a reasonable surrogate for a human knee for evaluating the level of joint line fixation with an interference screw. 24 32 The stiffness of the interference screw is 40% greater in porcine bone (476 N/mm) than that in young human tibia (340 N/mm) because the density of cancellous bone in a porcine knee is greater than that in young human bone. 24 The use of human bone instead of porcine bone might sufficiently decrease the stiffness of the interference screw so that the use of high-stiffness distal fixation devices restores anterior laxity and knee stiffness just as well at implantation.
The purpose of the present study was to use high-stiffness distal fixation devices instead of low-stiffness double staples and sutures tied to a post and to use a human knee instead of a porcine knee to determine whether the use of high-stiffness distal fixation devices restores anterior laxity and knee stiffness as well as an interference screw at the time of implantation. We hypothesized that high-stiffness distal fixation devices, which include tandem screws and soft tissue washers placed distal to the tibial tunnel, a WasherLoc at the distal end of the tibial tunnel, and a WasherLoc with compaction of a bone dowel in the tibial tunnel, restore anterior laxity and stiffness as well as an interference screw does placed at the joint line.
Materials and Methods
Knees from elderly humans (N = 11; mean age, 63 years; range, 46-77 years) were harvested and stored at -20°C. The cause of death was not known. Bone density was not measured because the tibia was reinforced with foam using a technique that is described later. Any specimen with degenerative arthritis or chondrocalcinosis as determined by radiographs or visual inspection at the time of ACL reconstruction was excluded from the study.
Aligning, Preconditioning, and Measuring Anterior Laxity and Stiffness of the Intact Knee
A 6 degrees of freedom load application system was used to apply a preconditioning and testing protocol to test each knee 2 (Figure 1). To prepare the knee for testing, all soft tissue 7 cm proximal and distal to the joint line was removed. The method of attaching and aligning the knee in the load application system with use of the functional axes method has been previously described. 2 4
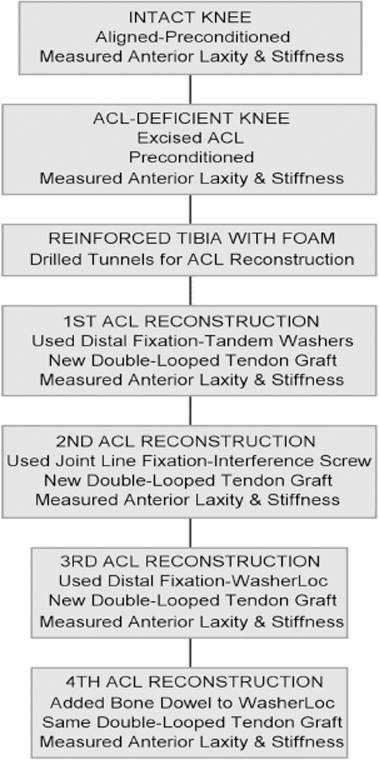
A flowchart depicting the sequence of steps, measurements, and treatments applied to each knee to determine whether the use of high-stiffness distal fixation devices restores anterior laxity and knee stiffness as well as an interference screw does at the time of implantation. Each knee had 4 ACL reconstructions and used 3 new double-looped tendon grafts.
The intact knee was preconditioned at 0°, 30°, and 90° in random order using a previously described protocol. 2 Five load cycles were applied at each flexion angle. Each load cycle consisted of the application and removal of an anterior and posterior load of 250 N to the tibia. This preconditioning protocol produces a repeatable load-displacement cycle in the intact knee 2 and preconditions the 2 bundles of the ACL. 29 A 2.5-N·m extension moment was applied, which defined 0° of knee flexion. 26
The intact knee was tested at 0°, 30°, 60°, 90°, and 120° of flexion using a previously described testing protocol. 8 The knee was initially placed in 30° of flexion, and the unloaded position of the tibia relative to the femur was determined. The unloaded position of the tibia relative to the femur was the position of the tibia after applying and removing a 45-N anterior load and a 45-N posterior load (Figure 2). The anterior limit of motion was the position of the tibia at 225 N of anterior load after increasing the load in 25-N increments. Anterior laxity at 225 N was calculated as the difference between the anterior limit of motion at 225 N of load and the unloaded position of the tibia. Anterior laxity was also calculated at 110 N of load from the load-displacement curve, which was used to compare the results from the present study to those of Ishibashi et al. 19 Knee stiffness was the slope of the load-displacement curve between 100 N and 225 N of anterior load determined by simple linear regression. 8 The determinations of anterior laxity at 225 N and 110 N of load and stiffness were repeated in the intact knee at 0°, 60°, 90°, and 120° in random order.
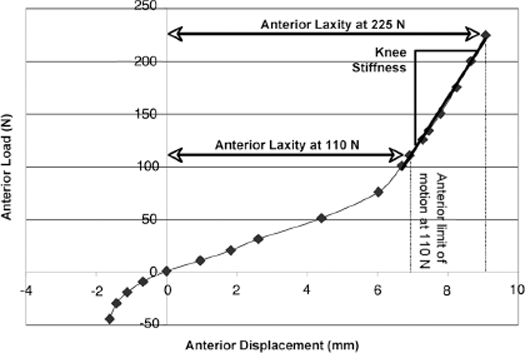
A typical load-displacement curve showing the method for determining anterior laxity at 225 N of load, anterior laxity at 110 N of load, and knee stiffness. Anterior laxity at 225 N and 110 N of anterior load was calculated as the difference in displacement between the unloaded position of the tibia (ie, 0,0 point on the graph) and the anterior limit of motion at 225 N and 110 N, respectively. Knee stiffness was the slope of the curve between 100 N and 225 N of anterior load.
Preparation and Stiffness Measurement of Double-Looped Tendon Grafts
Double-looped tendon grafts were constructed from bovine extensor tendons. The viscoelastic, structural, and material properties of bovine extensor tendons are similar to those of human hamstring grafts when the cross-sectional area is matched. 6 In contrast to human hamstring tendons, bovine extensor tendons are readily available, minimize the risk of transmitting human immunodeficiency virus and hepatitis to laboratory personnel, are lower in cost, and have been used in many cadaveric studies.3,11,12,18,20,21,34,36 Each double-looped bovine tendon (DLBT) graft was trimmed until the cross-sectional area ranged from 41 to 45 mm 2 as measured with an area micrometer. 6 13 Four centimeters of the end of each strand were whipstitched using a No. 1, braided, nonabsorbable suture (Ethibond, Ethicon Inc, Somerville, NJ).
Because the sequential insertion and removal of the fixation devices might damage the DLBT graft, introducing an unwanted carryover effect, a fresh graft was used for the tandem washer, interference screw, and WasherLoc. The stiffness of each of the 33 grafts was measured using a previously described technique. 3 Briefly, the stiffness of each DLBT graft was computed from a load-displacement test administered by a computer-controlled materials testing machine (Teststar IIs, v2.2 software, model 858, MTS Systems Corp, Minneapolis, Minn) with a 5-kN load cell (1010AF-1K-B, Interface, Scottsdale, Ariz). The DLBT graft was looped over a 6.3-mm-diameter steel bar attached to the base of the materials testing machine. A liquid nitrogen freeze clamp bolted to the shaft of the actuator was used to grip the free ends of the graft. Before gripping the graft, each strand was equally tensioned by hanging a 0.5-kg weight and passed over a pulley. While the strands were weighted, the freeze clamp was applied. The grip-to-grip length of the DLBT graft was 65 mm. Tension was applied to the graft with the actuator of the materials testing machine by cyclically loading the graft 11 times between 20 and 1000 N at a loading rate of 400 N/s. The first 10 cycles preconditioned the graft. Stiffness was computed from the load-displacement curve obtained during cycle 11.3,6,13 The applied tension of 1000 N is 2.5 times less than the mean ultimate load (2901 N) and well within the elastic range of the DLBT graft. 6
The 33 grafts were ranked in order based on stiffness and divided into 11 groups of 3 consecutive grafts. A group was then randomly assigned to each specimen. Within each group, a randomization protocol was used to allocate the graft to the tandem screws and soft-tissue washers, the interference screw, and the WasherLoc (and WasherLoc and bone dowel). A 1-factor analysis of variance showed that the mean stiffness of the grafts allocated to the interference screw (682 ± 35 N/mm), the WasherLoc and the WasherLoc and bone dowel (684 ± 34 N/mm), and the tandem washer and screws (682 ± 41 N/mm) was the same (P = .9916).
Measurement of Anterior Laxity and Stiffness of the ACL-Deficient Knee
The ACL was removed from the intact knee through a medial and lateral parapatellar incision. The ACL-deficient knee was replaced in the load application system. The anterior laxities at 225 N and 110 N of load and stiffness were determined using the same preconditioning and testing protocol described for the intact knee.
Reinforcement of the Tibia with foam and Placement of the Tunnels for ACL Reconstruction
The proximal metaphysis of the tibia was reinforced with foam using a previously described technique.3,11,12,36 The Food and Drug Administration accepts the use of a foam bone analog for evaluating the structural properties of fixation devices (http://www.fda.gov/cdrh/ode/odegr914.html). Foam reinforcement of the tibia from elderly cadavers provides fixation structural properties of stiffness, strength, and resistance to slippage similar to those of young human tibia. 3
The tibial tunnel was positioned with use of a guide (Howell 65-Degree Tibial Guide, Arthrotek, Warsaw, Ind) so that the graft did not impinge against the intercondylar roof and posterior cruciate ligament, and the tension pattern of the graft matched that of the intact ACL during passive flexion-extension. 12 34 The position of the tibial guide wire was checked with radiographs before drilling the tibial tunnel. The tibial tunnel was drilled using a 9-mm cannulated reamer. A 9-mm femoral aimer (Size-Specific Femoral Aimer, Arthrotek) was used to place a femoral guide wire with the transtibial technique. An open-ended femoral tunnel was drilled using a 15.9-mm cannulated reamer. An assembly consisting of the femoral fixation device and a tensiometer was inserted inside a bushing, which was made from Delrin AF to minimize friction (Figure 3). The tension in the graft was adjusted by turning the tensioning nut. The bushing was cemented in the femoral tunnel with the distal end of the bushing flush with the intercondylar roof.
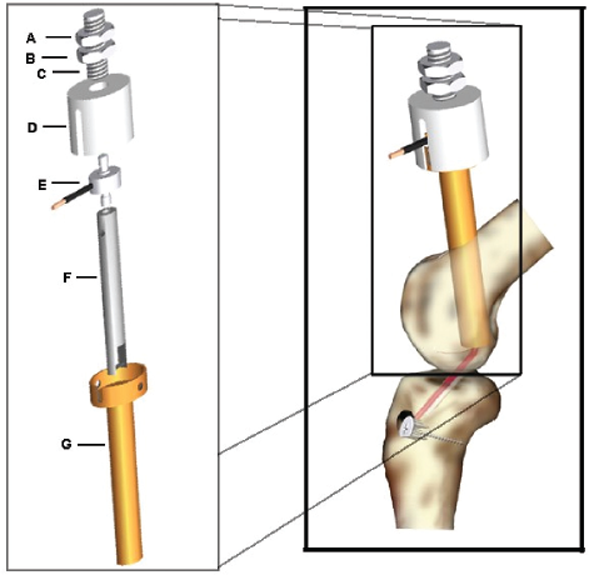
The assembly for fixing, tensioning, and measuring the tension of the double-looped tendon graft in the femoral tunnel. The double-looped tendon graft is looped around a crossbar at the distal end of the femoral fixation device (F). Proximal to the femoral fixation device is a locking nut (A), tensioning nut (B), threaded spindle (C), load cell housing (D), and load cell (E) (model 11, 1115 N, Honeywell Sensotec, Columbus, Ohio). The entire assembly is inserted into a bushing (G), which is made from Delrin to minimize friction. The bushing is rigidly fixed in the femoral tunnel with bone cement. Tension in the double-looped tendon graft is adjusted by turning the tensioning nut. Once the desired tension is applied, the locking nut is tightened to maintain the tension.
Reconstruction of the Knee with 4 Different Tibial Fixation Techniques
Each specimen was reconstructed with 4 tibial fixation techniques, which included the tandem screws, soft-tissue washers, and bicortical screws (18-mm-diameter soft-tissue anchor washers, 4.5-mm bicortical screws, Arthrotek); bioabsorbable interference screw (10 × 28-mm biointerference screw, Arthrex, Naples, Fla); WasherLoc (18-mm diameter with 4 extended spikes, Arthrotek); and WasherLoc with compaction of a bone dowel (Figure 4). Because the insertion and removal of the distal fixation devices could have affected the purchase of the interference screw, a nonrandomized testing sequence was used to minimize carryover effects. The tandem washers were tested before the interference screw was tested, which did not affect the purchase of the interference screw because the tandem washers were placed distal to the tibial tunnel. The interference screw was tested before the WasherLoc was tested.
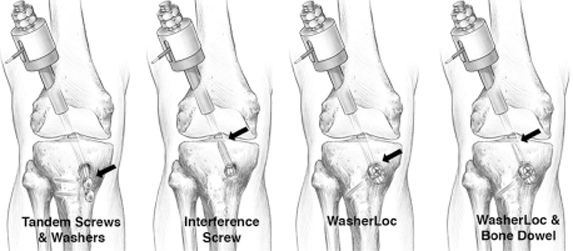
The arrow points to the level of fixation. The tandem screws and soft-tissue washers were placed distal to the tibial tunnel. The bioabsorbable interference screw was placed at the joint line. The WasherLoc was placed at the distal end of the tibial tunnel. The WasherLoc with supplemental fixation with the bone dowel moved the level of fixation to inside the tibial tunnel and closer to the joint line.
Technique for Distal Fixation with Tandem Washers
Distal fixation with the tandem washers and bicortical screws was performed by passing the DLBT graft around the crossbar of the femoral fixation device (Figure 3) and through the femoral and tibial tunnels. A 3.2-mm-diameter bicortical drill hole was made 11 mm distal to the distal exit of the tibial tunnel on the medial cortex. A second drill hole was made 19 mm distal and parallel to the first. The holes were threaded using a 4.5-mm tap. The washers were inserted to within 10 mm of the cortex by advancing the two 4.5-mm-diameter cortical screws. One strand from each tendon was wrapped in an S-shaped configuration around both screws, the other strands were wrapped in the opposite direction, and the strands were fixed using a previously described technique. 3 24 The knee was placed in full extension. The strands of each tendon were tied together to form a loop. A 55-N weight was suspended from each loop to tension the graft. The screws were tightened, which compressed the washers and graft against the tibia.
The reconstructed knee was replaced in the load application system at 0° of flexion. The graft was tensioned to 110 N by adjusting the tensioning nut. The knee was preconditioned using the same protocol used for the intact knee. After preconditioning, the knee was placed at 0° of flexion, and the graft was retensioned to 110 N. After a 10-minute wait period to allow for stress relaxation, the graft was once again tensioned to 110 N. The anterior laxity and stiffness were determined after applying the same preconditioning and testing protocol described for the intact knee.
Technique for Joint Line Fixation with Interference Screw
Joint line fixation with the interference screw was performed after removal of the tandem washers, screws, and double-looped tendon graft. A new double-looped tendon graft was prepared by tying the 2 strands of each tendon together to form a loop and suspending a 55-N weight from each loop. The section of the graft that would be inside the tibial tunnel was marked, and the 4 strands were sewn together with a No. 2 suture (Polysorb, United States Surgical, Inc, Norwalk, Conn) with use of a modified baseball stitch. The graft was passed through the knee, and the strands and a guide pin were inserted between the graft and the posterior wall of the tibial tunnel. A 55-N weight was suspended from each loop to tension the graft. A 10 × 28-mm soft-tissue interference screw was advanced over the guide pin until it was flush with the joint line. The anterior laxity and stiffness were determined after applying the same preconditioning and testing protocol described for the intact knee.
Technique for Fixation at the End of the Tibial Tunnel with WasherLoc
Fixation at the distal end of the tibial tunnel with the WasherLoc was performed after removal of the interference screw and double-looped tendon graft. A 17-mm-diameter counterbore was prepared in the distal end of the tibial tunnel to recess the WasherLoc. The new graft was passed through the knee and tensioned as previously described. The WasherLoc was threaded on an awl. The awl was positioned in the hole created by the counterbore, and 1 strand from each tendon was placed on opposite sides of the awl between the 4 long peripheral spikes of the WasherLoc. The WasherLoc was impacted into the counterbore. A 6.0-mm-diameter self-tapping cancellous screw was inserted through the lateral tibial cortex and tightened to compress the graft.3,18,23,24
Technique for Compaction of Bone Dowel into the Tibial Tunnel Proximal to the WasherLoc
Fixation with the bone dowel inside the tibial tunnel was performed with the WasherLoc and DLBT graft still in place. A 25-mm-long, cone-shaped dilator was driven into the tibial tunnel anterior to the double-looped tendon graft to the level of the joint line. A 35-mm-long, 8-mm-diameter bone dowel was harvested from a calf tibia with an age of 16 to 24 weeks with a dowel harvester. Calf tibias were chosen for the bone dowel because the density of the proximal tibia closely approximates that of young human bone. The bone dowel was compacted into the dilated opening. 18 The anterior laxity and stiffness were determined.
Statistical Analysis
Statistical analysis was performed with a 2-factor analysis of variance with a split-plot design to determine (1) the effect of fixation device and flexion angle on anterior laxity at 225 N of load, (2) the effect of fixation device and flexion angle on anterior laxity at 110 N of load, and (3) the effect of fixation device and flexion angle on knee stiffness. For each 2-factor analysis, the main factor was fixation device at 4 levels (tandem washers, interference screw, WasherLoc, and WasherLoc and bone dowel), and the subfactor was flexion angle at 5 levels (0°, 30°, 60°, 90°, and 120°). Because fixation devices were tested in a nonrandom order to minimize carryover effects, a split plot was used instead of a repeated-measures design. Anterior laxity at 225 N of load was referenced to the intact knee by subtracting the anterior laxity of the intact knee from that of the reconstructed knee. Hence, a positive value indicated that the anterior laxity at 225 N of load was greater than that of the intact knee. The anterior laxity at 110 N of load was normalized to compare the results in the present study to those of Ishibashi et al. 19 The knee stiffness also was normalized. Dividing the value of the reconstructed knee by the corresponding value of the intact knee and expressing the result as a percentage normalized anterior laxity at 110 N of load and knee stiffness. Hence, a percentage greater than 100 indicated that anterior laxity at 110 N of load and knee stiffness was greater than that of the intact knee. Post hoc analysis was performed with the Tukey test to determine significant differences between fixation levels. Significance was set at P < .05. In 2 specimens, the fixation with the interference screw failed. In these 2 specimens, the data concerning the anterior laxity and stiffness with the interference screw were not used in the statistical analysis.
Results
Anterior Laxity at 225 N of Load
Anterior laxity at 225 N of load referenced to the intact knee averaged across all flexion angles was 0.4 ± 1.9 mm for the interference screw, which was not significantly different from that of the tandem washers (0.0 ± 2.3 mm), the WasherLoc (0.7 ± 2.6 mm), and the WasherLoc and bone dowel (0.3 ± 2.6 mm) (Figure 5). The anterior laxity at 225 N of load with tandem washers was 0.3 mm less than with the WasherLoc (P = .0104). The anterior laxity at 225 N of the intact knee was 8.6 ± 1.3 mm at 0°, 14.8 ± 2.6 mm at 30°, 12.4 ± 2.1 mm at 60°, 10.1 ± 1.3 mm at 90°, and 10.4 ± 1.6 mm at 120° of flexion.
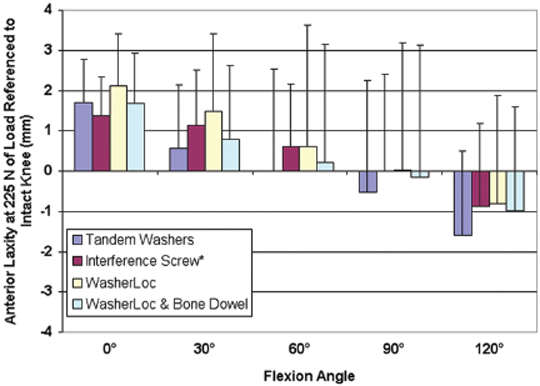
The mean anterior laxity referenced to the intact knee at 225 N of load for 4 different fixation levels at 5 different flexion angles. A value greater than 0 indicates that the anterior laxity was greater than that of the intact knee. The distal fixation devices of tandem washers, WasherLoc, and WasherLoc and bone dowel each restored anterior laxity as well as the interference screw did. Only 1 fixation level restored anterior laxity different than the others. The anterior laxity with the tandem washers was 0.7 mm less than that of the WasherLoc (P = .0104). Error bars indicate 1 SD. The asterisk indicates that the data concerning the performance of the interference screw from 2 specimens were excluded from the statistical analysis because the graft slipped past the screw.
Anterior Laxity at 110 N of Load
Anterior laxity at 110 N of load normalized to that of the intact knee at 30° of flexion was 98% ± 22% for the interference screw, which was not significantly different from that of the tandem washers (91% ± 25%), the WasherLoc (100% ± 29%), and the WasherLoc and bone dowel (96% ± 27%) (Figure 6). The anterior laxity at 110 N of load with tandem washers was less than with the WasherLoc (P = .0071).
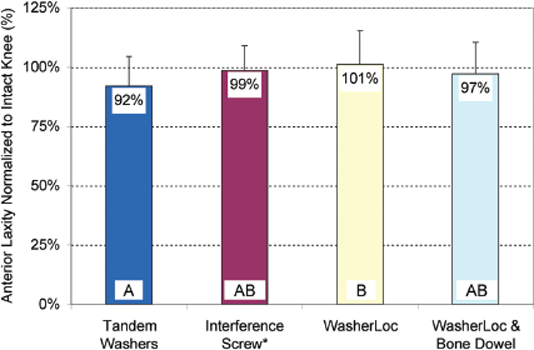
The mean anterior laxity normalized to that of the intact knee at 110 N of load for 4 different fixation levels at 30° of flexion in human bone in the present study. A value less than 100% indicates that the anterior laxity was less than that of the intact knee. The distal fixation devices of tandem washers, WasherLoc, and WasherLoc and bone dowel each restored anterior laxity as well as the interference screw did. The most likely explanation for the distal fixation devices restoring anterior laxity as well as the interference screw did is that each distal device provided high stiffness. Data points with different letters are significantly different.
Knee Stiffness between 100 and 225 N of Anterior Load
Knee stiffness normalized to that of the intact knee averaged across all flexion angles was 87% ± 15% for the interference screw, which was not significantly different from that of the tandem washers (82% ± 20%), the WasherLoc (83% ± 20%), and the WasherLoc and bone dowel (86% ± 21%) (Figure 7). No fixation device restored knee stiffness differently than another (P = .1138). The knee stiffness of the intact knee was 44.3 ± 5.9 N/mm at 0°, 35.8 ± 5.9 N/mm at 30°, 38.0 ± 4.0 N/mm at 60°, 41.7 ± 2.9 N/mm at 90°, and 42.2 ± 3.8 N/mm at 120° of flexion.
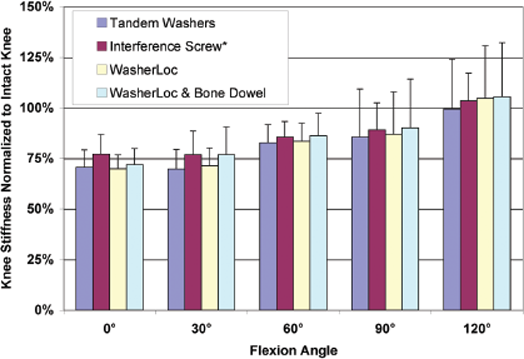
Knee stiffness normalized to that of the intact knee for 4 different fixation levels at 5 different flexion angles. A value less than 100% indicates that knee stiffness was less than that of the intact knee. The distal fixation devices of tandem washers, WasherLoc, and WasherLoc and bone dowel each restored knee stiffness as well as the interference screw did.
Discussion
The most important finding of the present study is that the use of a high-stiffness distal fixation device, such as tandem screws and washers, WasherLoc, and WasherLoc plus bone dowel, restored anterior laxity and knee stiffness as well as joint line fixation with an interference screw at implantation. The results of the present study support the principle that the stiffness of the fixation devices should be included along with the length of the graft when determining the stiffness of the graft-fixation complex. Consequently, the surgeon should consider the stiffness and slippage resistance of each fixation device and not just the length of the graft when performing an ACL reconstruction.
Interpretation and Clinical Relevance of Results
The clinical relevance of the level of fixation has been elusive because the ideal study design for determining the effect of level of fixation on anterior laxity and knee stiffness cannot currently be performed. The ideal study design requires the use of a single fixation device that provides the same stiffness when inserted at different distances from the joint line. Keeping the stiffness of the fixation the same at each level is not possible because currently available fixation devices can only be inserted either inside or distal to the tibial tunnel, and there is not a distal or intratunnel fixation device that provides the same stiffness.3,18,24,37
The study by Scheffler et al, 33 the study by Ishibashi et al, 19 and the present study each used different fixation devices with different stiffness at each site of fixation, which requires a discussion of the effect of these differences on the clinical relevance. The study by Scheffler et al used sutures tied to a post with a mean stiffness of 70 N/mm as the distal fixation (ie, low stiffness compared with interference screw) and an interference screw with a mean stiffness of 340 N/mm as the joint line fixation. They concluded that joint line fixation restored anterior laxity better than did distal fixation. 33 The study by Ishibashi et al used double staples with a mean stiffness of 170 N/mm as the distal fixation (ie, low stiffness compared with interference screw) and the interference screw with a mean stiffness of 340 N/mm as the proximal fixation. They also concluded that joint line fixation restored anterior laxity better than did distal fixation. 19 The present study used tandem screws and soft-tissue washers with a mean stiffness of 414 N/mm, the WasherLoc with a mean stiffness of 506 N/mm, and the WasherLoc with bone dowel with a mean stiffness of 565 N/mm as the distal fixations (ie, high stiffness compared with interference screw) and the interference screw with a stiffness of 340 N/mm as the proximal fixation. The conclusion of the present study was different in that high-stiffness distal fixation with tandem screws and soft-tissue washers, the WasherLoc, and the WasherLoc and bone dowel restored anterior laxity and knee stiffness as well as joint line fixation with the interference screw.
One reason for the different conclusions between the present study and the previous studies by Scheffler et al 33 and Ishibashi et al 19 is that the present study used high-stiffness distal fixation devices, and the 2 previous studies each used low-stiffness distal fixation devices. The use of high-stiffness fixation devices in the present study increased the stiffness of the graft-fixation complex according to the springs-in-series equation (described later), which better restored anterior laxity and knee stiffness. Collectively, these results suggest that the restoration of anterior laxity and knee stiffness at the time of implantation is determined more by the stiffness of the fixation device than by where the fixation device is placed with respect to the joint line.
The effect of the stiffness of the tibial and femoral fixation devices and the stiffness of the graft on the stiffness of the graft–fixation device complex can be understood with use of a springs-in-series model. The effect that the stiffness of the tibial fixation device (Kt), the stiffness of the graft (Kg), and the stiffness of the femoral fixation device (Kf) each has on the stiffness of the graft-fixation complex (Kgfc) is represented by the following equation
37
:
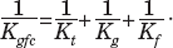
Predicting how the stiffness of the graft (ie, a shorter graft is stiffer than a longer graft as long as the cross-sectional area is the same6,13,37) and how the stiffness of the tibial and femoral fixation devices each determines the stiffness of the graft-fixation complex requires a clinically relevant understanding of the differences in the stiffness between each component. For example, consider a bone-tendon-bone graft (high stiffness) fixed to the femur with bone cement (high stiffness) and fixed to the tibia by a 7-0 suture tied to a post (extremely low stiffness because of the compliance of the thin suture bridge). The stiffness of the elastic suture determines the stiffness of the graft-fixation complex because it is the least stiff or most compliant component. In this case, the use of a bone-tendon-bone graft with a shorter tendon length, which increases the stiffness of the graft, does not increase the stiffness of the graft-fixation complex because the low stiffness from the suture is much less than the stiffness of the shorter graft.
The stiffness of soft-tissue grafts used in humans is either stiffer or similar in stiffness to fixation devices that are currently in clinical use.7,13,15,20,24,37 When a soft-tissue graft is used, 1 method for increasing the stiffness of the graft-fixation complex is to use a stiffer fixation method such as either high-stiffness distal fixation or the interference screw fixation, both of which are stiffer than are sutures tied to a post and double staples. 24 37 Another method is to use more than 1 fixation device such as supplementing the distal fixation by adding either a bone dowel 18 or an interference screw in series, inside the bone tunnel, and alongside the soft-tissue graft. 25 Two mechanisms by which the use of an intratunnel fixation to supplement distal tibial fixation increases the stiffness of the graft-fixation complex are that the bone dowel and interference screw in series with the distal fixation (1) stiffen the fixation and (2) stiffen the graft by shortening the functional length. 18 25
The mechanical consequences of using intratunnel fixation with an interference screw, high-stiffness distal fixation, or a bone dowel as a supplement to distal fixation to increase stiffness at time of implantation should be weighed against the biologic consequences after implantation. One biologic consequence is that the use of an interference screw significantly decreases stiffness and strength 4 weeks after implantation in contrast to the use of high-stiffness distal cortical fixation, which significantly increases stiffness. 35 The decrease in stiffness and strength after implantation results from the interference screw blocking approximately half of the surface area of the tunnel wall from healing to the tendon graft, resulting in 1-sided healing, 38 and from a loss in the mechanical fixation of the graft by the interference screw. 35 In contrast, the increase in stiffness after implantation from high-stiffness distal fixation results from the entire surface area of the tunnel wall healing circumferentially to the soft-tissue graft and the maintenance of the mechanical fixation by the device. 35 A second biologic consequence is that the interference screw causes tunnel widening. The insertion of large interference screws not only compresses the graft in the bone tunnel but also significantly enlarges the bone tunnel itself. 5 In contrast, the bone dowel prevents tunnel widening at 4 months and 1 to 2 years, which simplifies revision surgery. 27 Therefore, the use of high-stiffness distal fixation and the use of supplemental fixation with the bone dowel have both mechanical and biologic advantages by providing high stiffness at implantation, increasing stiffness after implantation, maintaining mechanical fixation after implantation, and preventing tunnel widening.18,27,35
Slippage is common with a wide variety of tibial fixation devices,9,24,28,32 and studies have shown that slippage has a profound effect on graft tension and the anterior laxity of the knee. A small 30-N loss in graft tension from slippage can increase anterior laxity 1 mm. 12 Slippage of a millimeter or more causes a millimeter-for-millimeter increase in anterior laxity. 12 22 These findings suggest that the use of fixation devices that resist slippage under cyclic load is a more important consideration for restoring anterior laxity than where the device is placed with respect to the joint line.
Joint line fixation slips more than does high-stiffness distal cortical fixation because the interference screw purchases cancellous bone, which is 30 times weaker than is the cortical bone purchased by high-stiffness distal fixation.9,24,28 Furthermore, there is a direct correlation between the holding strength of fixation devices and the thickness of cortical bone, so it is recommended that fixation devices be placed away from the joint line, into cortical bone if possible. 1 Hence, the use of slippage-resistant, high-stiffness distal fixation placed in cortical bone might better maintain anterior laxity after implantation than will the use of the interference screw, which has required backup with cortical fixation in females to reduce slippage. 16
At the time of implantation, a high-stiffness graft-fixation complex requires substantially less initial tension than does a low-stiffness graft-fixation complex to restore anterior laxity. 7 20 When the initial tension is not maintained postoperatively, a high-stiffness graft-fixation complex may be advantageous in avoiding a recurrence of knee instability because a high-stiffness fixation device partially compensates for the loss in tension. 20 However, several weeks after implantation, the stabilizing effect from the use of high-stiffness fixation devices diminishes as the fixation shifts from mechanical to biologic incorporation of the graft to the tunnel wall. 35 41 Therefore, a fixation device that has structural properties of resisting slippage under cyclic load and providing high stiffness might be more likely to restore anterior laxity during the first few weeks of implantation than will a fixation device that slips under cyclic load and provides low stiffness.
Methods Issues
One methods issue is whether the inability of the interference screw to restore anterior laxity better than high-stiffness distal fixation was caused by the stiffness of the femoral fixation device. Based on the springs-in-series equation, 37 we designed a high-stiffness femoral fixation to maximize the likelihood of detecting any difference in stiffness between the tibial fixation devices and their effect on anterior laxity. 20 The high stiffness of the femoral fixation device is similar to that of a cross-pin and was owing to the use of stainless steel components that abutted the Delrin bushing, which was cemented in the femoral tunnel. 20 37 The use of a femoral fixation device that was stiffer than all 4 fixations used in this study and the use of the same femoral fixation for each device combined to isolate the effect of the tibial fixation device on the restoration of anterior laxity and knee stiffness. Therefore, the use of a high-stiffness femoral fixation device was not the reason that high-stiffness distal fixation restored anterior laxity and stiffness as well as did joint line fixation with an interference screw.
A second methods issue is whether the inability of the interference screw to restore anterior laxity better than the WasherLoc and the WasherLoc and bone dowel was caused by tunnel dilation from the insertion and removal of the interference screw that compromised the subsequent purchase of the WasherLoc and WasherLoc and bone dowel. A carryover effect caused by tunnel dilation from testing the interference screw before the WasherLoc and WasherLoc and bone dowel is a best-case scenario for the interference screw and a worst-case scenario for the WasherLoc and WasherLoc and bone dowel. It is possible that the restoration of anterior laxity and knee stiffness might have been better with the WasherLoc and the WasherLoc and bone dowel than with the interference screw if the interference screw had been tested last. However, the carryover effect from tunnel dilation did not affect the conclusion that high-stiffness distal fixation restored anterior laxity and stiffness as well as did joint line fixation with an interference screw.
A third methods issue is whether the inability of the interference screw to restore anterior laxity better than did high-stiffness distal fixation with the tandem screws and soft-tissue washers, WasherLoc, and WasherLoc and bone dowel was caused by the use of a 28-mm interference screw instead of a longer 35-mm interference screw. The use of a longer 35-mm interference screw would not have increased the stiffness by shortening the functional length of the graft because the tips of both screws are placed at the joint line in the subchondral cortical bone. The use of a longer 35-mm interference screw might have proportionally increased the stiffness to 425 N/mm based on the 340 N/mm stiffness of the 28-mm screw. The potential increase in stiffness from the use of a longer 35-mm interference screw is still less than the stiffness of the WasherLoc and the WasherLoc and bone dowel and is similar to that of the tandem screws and soft-tissue washers. Although the stiffness at implantation with the longer interference screw might have been greater than with the shorter screw, the stiffness after implantation with the longer interference screw might be less. The use of a longer screw blocks more surface area of the tendon from healing to the tunnel wall than with the shorter screw, which decreases both the stiffness and strength of tendon-tunnel healing. 10 35 Therefore, the use of a 35-mm interference screw in the present study would not have changed the conclusion that the 3 high-stiffness distal fixation methods restored anterior laxity and knee stiffness as well as joint line fixation with the interference screw because all the tested fixation methods still had similar stiffness. Additional studies are required to determine whether there is a clinical benefit to the use of a longer interference screw.
A fourth methods issue is whether the inability of the interference screw to restore anterior laxity better than the high-stiffness distal fixation methods tested in our study was caused by the use of elderly cadaveric knees in which the tibial metaphysis was reinforced with foam instead of using young human knees. For the foam to have caused the interference screw not to restore anterior laxity and knee stiffness better than did distal fixation as was shown by Ishibashi et al 19 and Scheffler et al, 33 the stiffness of the interference screw fixation in foam would have had to be less than the stiffness in young human tibia, and/or the stiffness of the distal fixation methods in foam would have had to be greater than the stiffness in young human tibia. We chose to reinforce the tibial metaphysis with foam because the stiffness with the interference screw, WasherLoc, and tandem screws and soft-tissue washers in foam-reinforced tibia is similar to that in young human tibia.3,12,36 Porcine tibia, which was used in the study by Ishibashi et al, was not used in the present study because in comparison to young human cadaveric tibia, graft slippage is underestimated using porcine tibia, stiffness is overestimated, and failure load is overestimated. Hence, porcine tibia is not a reasonable surrogate for human cadaveric tibia for evaluating ACL reconstructions. 24 32 Therefore, the use of foam-reinforced tibia is a better surrogate than is porcine bone and was not the reason that the 3 high-stiffness distal fixation methods restored anterior laxity and knee stiffness as well as joint line fixation with the interference screw because the stiffness of all the tested fixation methods in foam-reinforced and young human tibia was similar.
A final methods issue is whether the inability of the interference screw to restore anterior laxity better than high-stiffness distal fixation with the WasherLoc and a bone dowel compacted in the tibial tunnel was caused by the use of a bone dowel from calf tibia instead of from young human tibia. Fresh proximal calf tibia (age, 16-24 weeks) was used in this study because calf proximal tibia approximates the density of young human bone, according to a previously reported model.17,39,40 The increase in stiffness of 58 N/mm from compacting a calf bone dowel in the tibial tunnel 18 is similar to the reported increase in stiffness of 41 N/mm from compacting human bone reamings in the femoral tunnel. 37 Therefore, the use of a bone dowel from proximal calf tibia instead of from young human tibia was not the reason that joint line fixation with the interference screw did not restore anterior laxity and knee stiffness better than a bone dowel did.
In summary, the results of the present study in conjunction with the results of previous studies by Ishibashi et al 19 and Scheffler et al 33 support the principle that the stiffness of the fixation devices should be included along with the length of the graft when determining the stiffness of the graft-fixation complex at implantation. In vitro, the use of high-stiffness distal fixation devices such as tandem washers, WasherLoc, and WasherLoc and bone dowel restores anterior laxity and knee stiffness as well as joint line fixation with an interference screw and better maintains anterior laxity when there is a loss in graft tension. 12 20 These in vitro findings suggest a biomechanical explanation for the clinical observation that the use of distal fixation restores anterior laxity as well as joint line fixation 2 years after reconstruction. 14