
Abstract
Background:
The International Knee Documentation Committee Subjective Knee Evaluation Form is a knee-specific instrument composed of 18 questions. It is commonly used in adult and pediatric studies as a surgical outcome measure. Normative data exist for an adult population, but there have been no published normative results for younger subjects.
Purpose:
To compile and report pilot normative International Knee Documentation Committee Subjective Knee Evaluation Form scores in a preadolescent population.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The International Knee Documentation Committee Subjective Knee Evaluation Form was administered to 146 seventh-grade students (aged 12–14 years) at 2 local schools. The form was administered in its original format. Demographic and descriptive results were compiled.
Results:
One hundred twenty-five completed responses were eligible for analysis. The mean age was 13.2 years (SD, 0.5; range, 12.2–14.2 years); 15% of participants had a history of knee injury or pain. The mean International Knee Documentation Committee score for all respondents was 89.4 (SD, 10.5; 95% confidence interval, 87.6–91.3; range, 52–100).
Conclusion:
This study provides pilot normative data for mean International Knee Documentation Committee scores in a preadolescent population. The mean score in this younger cohort is consistent with normative data of adults age 35 years or younger. Although the International Knee Documentation Committee Subjective Knee Evaluation Form is often used in adolescent surgical studies, its validity in these populations remains to be established. Further work to establish the psychometric properties of the current form in younger age groups would be of significant benefit to clinicians.
Keywords
Isolated midsubstance injuries to the ACL in skeletally immature children were previously thought to be rare, with up to 80% of children younger than 12 years reportedly suffering tibial spine avulsions during ACL disruption. 7 More recent case studies have suggested that midsubstance tears are significantly more common than previously reported.3,8,9,12,14,15 In both adult and pediatric studies, the outcomes of ACL injuries are typically assessed by physical examination (positive anterior drawer, Lachman, or pivot-shift test results), KT-1000 arthrometer testing, radiographic imaging, and functional outcome questionnaires. A variety of knee-specific questionnaires have been developed and validated in the literature. These tools are typically created using adult population data yet are often employed in pediatric studies because no child-specific knee outcome measure currently exists.
The International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form is a commonly used knee function assessment tool. It is a knee-specific, rather than disease-specific, instrument comprising 18 questions. Its maximum score is 100 points. The form has been adopted by the American Orthopaedic Society for Sports Medicine; the European Society of Sports Traumatology, Knee Surgery and Arthroscopy; and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine. Its validity, responsiveness, and normative data have each been established for adult populations.2,5,6 The IKDC form is offered in 6 different languages and is available online at http://www.sportsmed.org/research/index.asp.
Within the pediatric literature, the IKDC Subjective Knee Evaluation Form has been used to characterize the success of various ACL reconstructive techniques.1,4,10,11,13 Because the IKDC form was not developed for children, it is difficult to ensure the validity of these reported scores. Recently, a large cross-sectional study reported normative data for the IKDC form of 5246 adult knees. 2 The purpose of our study was to provide normative pilot data of IKDC scores in a preadolescent population.
Methods
This was a cross-sectional pilot study designed to provide normative data for the IKDC Subjective Knee Evaluation Form in a population of grade 7 students. Seventh-grade students were selected because they represent our target population of 12- to 13-year-old girls and boys who are at risk for significant knee injuries, but they have not reached skeletal maturity. The Demographic Form and the Current Health Assessment Form created by the IKDC were also administered.
Recruitment
After receiving approval from our institutional review board, potential participants were identified from 2 local single-sex private schools. Seventh-grade students were summoned during their physical education classes to an educational lecture. All students were given the opportunity to participate or decline. After informed consent was obtained, participants completed all 3 IKDC forms: the Demographic Form, the Current Health Assessment Form, and the Subjective Knee Evaluation Form. These forms were administered by 1 of the authors in their original formats, without any modifications. The students were instructed to provide responses that reflected the function of their worst knees. On completion of the questionnaires, participants were provided with a presentation on knee function and anatomy. The presentation did not include any material regarding the IKDC forms, other questionnaires, or any other related research.
Data Analysis
Scores for the Subjective Knee Evaluation Form were calculated based on an updated method described by the IKDC. 2 Forms with fewer than 90% of the questions answered were considered incomplete and were excluded. Participants who had previously sought medical attention for knee pain or injury were identified and included in the results; these subjects also were reported separately. Data analysis was performed in consultation with a full-time statistician. Demographic and descriptive statistics were calculated using S-Plus 7.0 software (Insightful Corp, Seattle, Wash). Because of the exploratory nature of collecting pilot data, a priori hypotheses were not established. Therefore, performing inferential tests was thought to be inappropriate, and the results are reported as mean values with 95% confidence intervals (CIs). These results will facilitate hypotheses generation for subsequent studies.
Results
The IKDC Subjective Knee Evaluation Form was completed by 146 respondents: 73 boys and 73 girls. No student declined to participate; however, 21 submitted forms were excluded because they were incomplete. Most incomplete forms were missing numerous responses, and no specific questions were identified as being frequently unanswered. Therefore, there were 125 (86%) eligible forms for analysis (Table 1). Fifteen percent (19/125) of eligible respondents indicated a history of knee injury as reported on the IKDC Demographic Form.
Number and Gender of Respondents Included in Analysis
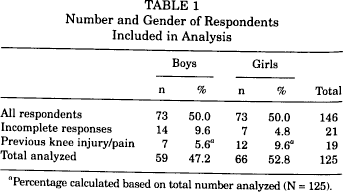
Percentage calculated based on total number analyzed (N = 125).
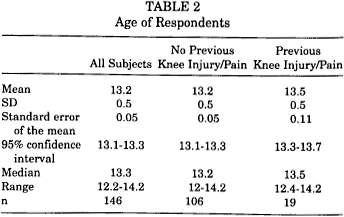
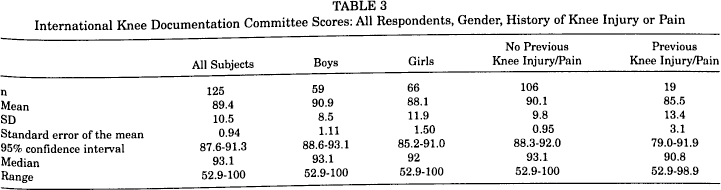
The mean age of the participants was 13.2 years (SD, 0.5; 95% CI, 13.1-13.3; range, 12.2-14.2 years) (Table 2). The results of the IKDC scores are presented in Table 3. The mean score for all respondents was 89.4 (SD, 10.5; 95% CI, 87.6-91.3; range, 52.9-100). Respondents with a history of knee injury or pain were included in the compiled data. In addition, the results from these participants were stratified and analyzed separately; their results are also found in Table 3. Participants with a history of knee injury or pain included 12 girls and 7 boys.
Age of Respondents
International Knee Documentation Committee Scores: All Respondents, Gender, History of Knee Injury or Pain
Discussion
The primary purpose of this study was to provide clinicians with preliminary normative scores for preadolescent knees. These descriptive data should help facilitate future studies involving the IKDC Subjective Knee Evaluation Form in pediatric and adolescent populations.
The mean IKDC score of all respondents was similar to the young adulthood data published recently in a study performed by members of the IKDC. Anderson et al 2 reported that there was no difference in scores among the age categories of respondents 18 to 34 years old (mean scores, 89.1 and 88.9; ages 18-24 and 25-34 years, respectively); however, there was an inverse relation between scores and age groups older than 34 years. The authors went on to suggest either that the IKDC Subjective Knee Evaluation Form has limited sensitivity among highly functioning knees or that there really is no difference in the function of younger adult knees. Our results support the suggestions made by the IKDC and extend into the preadolescent age group.
A stratified review of the mean scores for participants with previous knee pain compared to scores of subjects without any previous knee pain revealed substantial overlap between the 95% CIs. This is most likely because of the large differences in sample sizes between the 2 groups. The prior knee injury group was composed of 19 subjects, and its mean score had a wide CI from 79.0 to 91.9. Conversely, the larger injury-free group's mean CI was noticeably narrower (88.3-92.0). If the sample sizes were to be increased, we would expect the CIs to narrow and the overlap to decrease or resolve.
There are some limitations to this pilot study. It is a cross-sectional design that only included 2 private schools within our center's local catchment. The physical education requirements for these students are the same as those for all independent and public schools within the province. We do not believe the functional health of our cohort's knees should differ significantly from that of their peers in other schools; however, as this is not a random sample, we cannot ensure its external validity. In addition, it only included 1 age group and may not reflect a broader age distribution. Furthermore, in this initial pilot study, we are unable to comment on the form's reliability, validity, or responsiveness in our population.
The current IKDC Subjective Knee Evaluation Form was developed and tested in adult populations. The mean age was 37.5 years (SD, 16.2), and 83.2% had graduated high school. 5 These demographics are significantly different from the pediatric and adolescent populations that have used this form. One must remember that the psychometric properties are established for an instrument within a specific population, not just for the measurement tool alone. Vitale et al 16 clearly highlighted this point when they demonstrated that the popular adult quality-of-life measures, the Short Form–36 and the EuroQol, are not valid in adolescent patients with orthopaedic problems (aged 10-18 years). To ensure the form is reliable, valid, and responsive in pediatric and adolescent age groups, additional studies will be required.
Conclusion
The results of this study provide clinicians with some initial normative IKDC scores for a preadolescent population. These pilot data are consistent with recently published young adult normative scores (age < 35 years). Although the IKDC Subjective Knee Evaluation Form provides a quantifiable, knee-specific measurement tool, its reliability, validity, and responsiveness in adolescent and pediatric populations have not been studied. Further work to establish the psychometric properties of the current IKDC form in younger age groups would be of significant benefit to clinicians.