
Abstract
Background:
Previous studies have shown comparable biomechanical properties of double-row fixation versus double-row fixation with a knotless lateral row. SutureBridge is a construct that secures the cuff with medial row mattress suture anchors and knotless lateral row fixation of the medial suture ends. Recent completely knotless constructs may lead to lesser clinical outcomes if the construct properties are compromised from lack of suture knots.
Hypothesis:
A completely knotless construct without medial row knots will compromise the biomechanical properties in both cyclic and failure-testing parameters.
Study Design:
Controlled laboratory study.
Methods:
Six matched pairs of cadaveric shoulders were randomized to 2 groups of double row fixation with SutureBridge: group 1 with medial row knots, and group 2 without medial row knots. The specimens were placed in a materials test system at 30° of abduction. Cyclic testing to 180 N at 1 mm/sec for 30 cycles was performed, followed by tensile testing to failure at 1 mm/sec.
Results:
Data included cyclic and failure data from the materials test system and gap data using a video digitizing system. All data from paired specimens were compared using paired Student t tests. Group 1 had a statistically significant difference (P < .05) for gap formation for the 1st (3.47 vs 5.05 mm) and 30th cycle (4.22 vs 8.10 mm) and at yield load (5.2 vs 9.1 mm). In addition, there was a greater energy absorbed (2805 vs 1648 N-mm), yield load (233 vs 183.1 N), and ultimate load (352.9 vs 253.9 N) for group 1. The mode of failure for the majority (4/6) of group 2 was lateral row failure, whereas all group 1 specimens failed at the clamp.
Conclusion:
Although lateral row knotless fixation has been shown not to sacrifice structural integrity of this construct, the addition of a knotless medial row compromises the construct leading to greater gapping and failure at lower loads.
Clinical Relevance:
This may raise concerns regarding recently marketed completely knotless double row constructs.
The goal of rotator cuff repair is to obtain optimal initial fixation with anatomic reproduction of the footprint to decrease stresses at the tendon-bone interface and increase the surface area for healing. 10 The supraspinatus retear rate has varied in clinical studies, depending on initial tear characteristics.2,11 Ultrasound and MRI imaging studies have shown a 76% to 94% retear rate after surgical repair.2,9 In the classic study by Harryman et al, 11 the correlation of postoperative rotator cuff integrity and clinical outcome was thoroughly examined. Several other studies have shown that cuff integrity is correlated with better function and strength postoperatively.3,8,10 It is this correlation of cuff integrity and clinical outcome that has shifted surgeons to focus on the variables of repair technique and strength of construct to improve the initial repair strength. In principle, a rotator cuff repair construct with superior biomechanical properties at the time of fixation should provide a better environment for tendon healing and lead to a superior clinical result.
Initial arthroscopic rotator cuff repairs were performed with simple suture configurations with suture anchors in the supraspinatus footprint. Traditional double-row fixation involves repair with 2 anchors medially at the articular margin and 2 anchors laterally at the edge of the footprint. 14 Multiple biomechanical studies have shown traditional double-row fixation to provide better initial rotator cuff repair characteristics than single row,13,15,17,22 although 1 study showed equivalent load to failure and displacement under cyclic loads for double- and single-row fixation. 16 Despite the superior biomechanical properties of double-row fixation and its variants (M. J. Siskovsky et al, unpublished data, 2007),13,15,17,18,20,22 it is not yet clear if this translates to improved clinical results.
The SutureBridge with PushLocks (Arthrex, Naples, Fla) is a construct that can be performed arthroscopically and simplifies double-row fixation by allowing for knotless lateral row fixation using an interference fit of the medial row sutures. This technique, as well as the “transosseous equivalent” repair precursor, has been shown in biomechanical studies to have superior biomechanical properties, greater footprint contact area, and pressure than traditional double-row fixation (M. J. Siskovsky et al, unpublished data, 2007).18,20 Rotator cuff repair constructs have recently been marketed that presumably allow for a technically easier and faster surgery from elimination of any knot tying. The purpose of this study was to determine the biomechanical importance of medial row knot fixation in the SutureBridge with PushLocks (Arthrex) construct. Our hypothesis was that medial row knots will protect the supraspinatus footprint area from gap formation in cyclic loading and increase the yield load, ultimate load, and the energy absorbed by the construct in failure loading.
Materials and Methods
Specimen Preparation
Six matched pairs of fresh-frozen cadaveric shoulders stored at -20°C were obtained for biomechanical testing. All cadaveric specimens were removed from freezing 24 hours before dissection. No preexisting shoulder injuries were noted in the specimens. The average age of the specimens was 59.7 years (range, 54–65). All specimens were from male cadaveric specimens. Starting medially at the muscle bellies that were dissected from the scapula, the interval between the infraspinatus and supraspinatus was identified to allow accurate identification of the posterior border of the tendon. The infraspinatus was removed. The long head of the biceps tendon was used to identify the rotator interval and the anterior border of the supraspinatus. The rotator interval was removed, but the subscapularis was left intact for another experiment. The supraspinatus tendon was sharply dissected from the greater tuberosity, and the distal 10 mm of the supraspinatus tendon was resected to simulate a 1-tendon, medium-sized rotator cuff tear with distal tendon loss. The footprint of the supraspinatus tendon was debrided of soft tissue with a scalpel. The mean dimensions of the supraspinatus footprint were 26.37 mm from anterior to posterior and 14.83 mm from medial to lateral. A shoulder of each matched pair was randomized to a SutureBridge with Pushlock (Arthrex) construct with (group 1) or without (group 2) medial row horizontal mattress knots.
Repair Technique
Constructs were performed with a similar configuration to previous studies (M. J. Siskovsky et al, unpublished data, 2007).13,18,19 Each construct consisted of two 6.5-mm fully threaded metallic anchors (Arthrex) with a single loaded No. 2 Fiberwire (Arthrex). The medial row anchors were placed adjacent to the cartilage-footprint junction at 45° to the longitudinal axis of the humerus. As per the manufacturer's protocol, the anchor was used to create a pilot hole with a mallet and self-tapping. The anterior anchor was placed 5 mm posterior to the bicipital groove, while the posterior anchor was placed 12 to 13 mm posterior to it. Both sutures from each anchor were passed through the tendon in a horizontal mattress configuration. Sutures were passed for the medial row anchor 5 to 7 mm apart centered about each anchor in the sagittal plane. The medial row tendon suture passes were passed with Keith needles to re-create the full footprint attachment of the remaining supraspinatus tendon out to the lateral edge. This typically led to a suture placement 15 mm medial to the tendon edge. The sutures were tied in a horizontal mattress configuration without a knot pusher in group 1 using a sliding 3 half-hitch knot followed by 3 alternating half-hitches. The same construct was created for group 2 with the only exception that the medial row horizontal sutures were not tied (Figure 1). For both groups, lateral row fixation was performed with 1 suture end from each of the medial row anchors with two 4.5-mm PushLocks (Arthrex). The Pushlock is a knotless suture fixation device that creates an interference fit of the suture against the bone. Before lateral row fixation, the sutures were pretensioned to 4 kg with a manual tensiometer. A pilot hole was made 1 cm lateral to the edge of the supraspinatus footprint using the Pushlock 3.5-mm punch. For group 2, the anterior sutures and posterior sutures from each medial row anchor, respectively, were grouped and fixed with two 4.5-mm PushLocks for the lateral row without crossing the sutures or each anchor. Thus, the only variable between group 1 and group 2 was the presence of a medial row horizontal mattress knot for the anterior and posterior anchors (Figure 1).
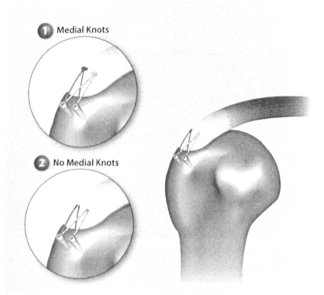
Diagram of the supraspinatus repair construct. The inset diagrams show our experimental groups: group 1 (medial row knots) and group 2 (completely knotless) variations of the SutureBridge with PushLocks (Arthrex, Naples, Fla).
Biomechanical Testing
An Instron materials testing machine (Canton, Mass) was used to measure the biomechanical properties of each specimen at an abduction angle of 30°, similar to previous studies (M. J. Siskovsky et al, unpublished data, 2007).20,22 The proximal humerus was cut at a length of 15 to 20 cm. The humeral shaft was potted into PVC tubing using plaster. Two screws were placed at 90° to further secure the bone to the PVC tube. The PVC tube was then fixed with multiple interference screws into a metal sleeve that directly mounted to the materials testing machine. A large bolt was placed through the center of the construct to further anchor the metal sleeve to the humeral shaft and PVC tubing. The humeral head was cut obliquely to remove approximately the medial 30% of the humeral head to allow placement of the tendon clamp as distal as possible on the supraspinatus. Care was taken to leave at least 10 mm of lateral humeral articular surface to avoid compromise of the medial row anchors. The supraspinatus tendon was whipstitched with two No. 2 Fiberwire sutures (Arthrex) and fixed into the clamp with double-sided fine sand paper at the tendon-clamp interface, typically within 10 to 15 mm of the repair site. Black paint was used to make paired markers on the superior surface of the specimen at the greater tuberosity, the free tendon edge, and 15 mm medial to the free tendon edge (Figure 2). We created 2 rows of data points both anteriorly and posteriorly on the tendon. Each repair underwent cyclic stress testing from a 10-N preload to 180 N at 1 mm/s for 30 cycles. The cyclic loading protocol is a modification of the original protocol of Burkhart et al 4 and similar to previous studies (M. J. Siskovsky et al, unpublished data, 2007). 20 Subsequently, a tensile test to failure was performed with a 10-N preload loaded at 1 mm/s. If the tendon grossly slipped from the clamp during cyclic testing, it was reclamped and tested for 30 more cycles. Only 2 specimens had gross clamp slippage before completion of the first cycle of testing and were reclamped. The repair sites were judged to be intact at the time of reclamping, and the resultant data were similar to the other specimens. All specimens were reclamped routinely before failure testing. A Video Digitizing System (VDS) (WINanalyze, Germany) was used to calculate data from the points painted on the superior surface of the supraspinatus repair construct that were video-recorded during testing. The difference in displacement of the black markers on the tendon edge was determined relative to the markers on the greater tuberosity with the VDS system; thus any small degree of clamp slippage or slight variation in marker placement was made irrelevant.
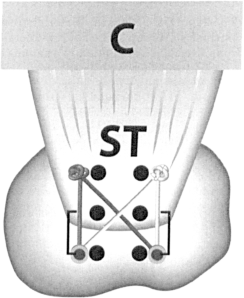
Diagram of the materials testing system and placement of markers on the bursal surface of the supraspinatus tendon. The paired markers are placed near the medial row, the tendon edge, and on the greater tuberosity. The brackets represent the difference in displacement of the tendon edge relative to the greater tuberosity calculated by the VDS system to measure gap formation. C, clamp; ST, supraspinatus tendon.
Statistical Analysis
Paired Student t tests were performed to compare paired specimens. Data were analyzed using the anterior markers, posterior markers, and the averages of the 2 markers between the 2 testing groups. Anterior and posterior markers within each specimen were found to be similar, and thus the mean values could be used for statistical analysis. The level of statistical significance was set at P < .05. Previous studies in our laboratory have shown that 6 matched pairs of specimens are needed to detect a minimum of 4-mm difference with a 5% level of significance and achieve a power of 97.2%.18,20
Results
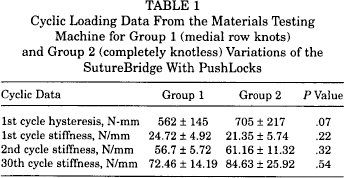
Cyclic data included 1st cycle hysteresis and stiffness at the 1st, 2nd, and 30th cycle. These data were obtained using the materials testing machine. Stiffness for the 1st, 2nd, and 30th cycles and failure were similar between groups (Table 1). The second cycle stiffness was double the stiffness of the first cycle in both groups. Hysteresis for the first cycle had a higher mean for group 2, but the P value of .07 was not significant.
Cyclic Loading Data From the Materials Testing Machine for Group 1 (medial row knots) and Group 2 (completely knotless) Variations of the SutureBridge With PushLocks
Gap formation was measured by VDS as the difference in marker displacement between the edge of the supraspinatus and the greater tuberosity markers. Gap was calculated for the 1st cycle, 30th cycle, at yield load, and at failure load (Table 2). Group 1 had a statistically significant difference (P < .05) with less gap formation for the 1st (3.47 vs 5.05 mm) and 30th cycle (4.22 vs 8.10 mm) and at yield load (5.2 vs 9.1 mm). The statistically significant differences in gap formation led to an increase in 1st cycle gap, 30th cycle gap, and gap at yield load of 45%, 92%, and 78%, respectively, in group 2 compared with group 1. Gap formation at ultimate load had a P value of .053 for the mean data despite having a statistically significant P value of .04 for the posterior markers only. Of all the data, 2 data points for gap formation had slight differences across paired specimens for the anterior and posterior data points. For first cycle gap formation, despite the statistically insignificant difference in the posterior cuff markers (P = .109), the anterior markers (P = .041) and mean (P = .048) were significant. For gap at ultimate load, it was the only VDS gap data category with a P value greater than .05 (.053). The anterior and posterior data points had P values of .095 and .04, respectively. Thus, the difference in posterior data point was statistically significant, although the mean data P value was greater than .05.
Gap Data From the Video Digitizing System (VDS) Analysis for Group 1 (medial row knots) and Group 2 (completely knotless) Variations of the SutureBridge With PushLocks
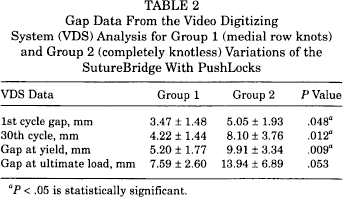
P < .05 is statistically significant.
Failure loading data from the materials testing machine included load and displacement at yield and ultimate load and energy absorbed (Table 3). There was a statistically significant greater energy absorbed (2805 vs 1648 N-mm), yield load (233 vs 183.1 N), and ultimate load (352.9 vs 253.9 N) for group 1 compared with group 2. The statistically significant differences in the load transmission led to a decrease in the yield load, ultimate load, and energy absorbed of 22%, 28%, and 41%, respectively, in group 2 compared with group 1.
Failure Loading Data From the Materials Testing Machine for Group 1 (medial row knots) and Group 2 (completely knotless) Variations of the SutureBridge With PushLocks

P < .05 is statistically significant.
The mode of failure for all group 1 specimens was at the tendon-clamp interface, whereas the majority (4/6) of group 2 had lateral row failure (Figure 3). The remaining specimens in group 2 failed at the tendon-clamp interface. The conclusions regarding mode of failure are simply trends since statistical analysis is not possible given the small numbers. Our study was not powered to examine modes of failure.
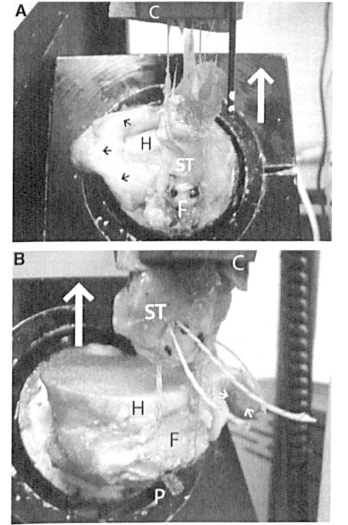
A, Group 1 specimen failure after the tendon shredded from the soft-tissue clamp. The white arrow denotes the direction of loading. The little black arrows point to the subscapularis. C, clamp; ST, supraspinatus tendon; F, footprint on greater tuberosity; P, Pushlock. B, Group 2 specimen failure at the lateral row. The PushLocks (Arthrex, Naples, Fla) in the lateral row have been ejected from the direct pull on the underlying bridge sutures. The large white arrow denotes the direction of loading; little white arrows point to the subscapularis. C, clamp; ST, supraspinatus tendon; F, footprint on greater tuberosity; P, Pushlock.
Discussion
The evolution of arthroscopic double-row fixation to a technically easier procedure is ongoing. Techniques such as the SutureBridge with PushLocks (Arthrex) have evolved to reduce the number of suture knots with a knotless lateral row to simplify the arthroscopic repair of supraspinatus tears. Recently available, completely knotless repair constructs have not been evaluated with biomechanical or clinical studies.
Our study used the SutureBridge with PushLocks construct as a model to demonstrate the importance of medial row knots with a knotless lateral row. This partially knotless construct evolved from the “transosseous equivalent” repair. Using the medial sutures to compress the supraspinatus onto the footprint with lateral biotenodesis screw fixation created 30% more footprint contact pressure, nearly double the footprint contact area, and a significantly greater mean ultimate load to failure.18,20 The SutureBridge with PushLocks eliminates the need for suture knots laterally over the biotenodesis screw. When compared with traditional double-row fixation, this construct has been shown to have significantly greater mean ultimate strength and energy absorbed to failure but had no statistically significant difference in footprint gap formation or yield strength (M. J. Siskovsky et al, unpublished data, 2007).
Our study shows a compromise in many biomechanical parameters when the SutureBridge with PushLocks construct is performed without medial row knots. Although the cyclic data were very similar, several statistically significant differences were found in failure testing and gap measurements. Yield load, ultimate load, and energy absorbed decreased by 22%, 28%, and 41%, respectively. Gap formation increased in the 1st cycle gap, 30th cycle gap, and gap at yield load by 45%, 92%., and 78%, respectively. This increase in gapping at the repair site and decrease in load transmission show the importance of the medial row knots in protecting the repair site from biomechanical stresses. Changes to the construct to make it completely knotless sacrifice many of the properties that make it comparable, and for some biomechanical parameters superior, to traditional double-row fixation.
Biomechanical studies of rotator cuff repair constructs that fail at points other than the repair site show the flaws in biomechanical testing studies. In the “transosseous equivalent” repair study, there were 2 greater tuberosity fractures and 4 musculotendinous junction failures. 20 SutureBridge with PushLocks constructs had 100% (6/6) failure within the supraspinatus muscle or tendon itself (M. J. Siskovsky et al, unpublished data, 2007). Our study also showed this trend as all group 1 failures and only 2 group 2 failures failed at the tendon-clamp interface because the stresses were bypassed away from the repair site to the clamp. This trend suggests that the loads transmitted may have been even larger had the tendon-clamp interface or the proximal tendon not failed. Despite this fact, load transmission was significantly greater in group 1 with medial row knots. Unlike bridging suture techniques with knotless lateral row fixation, traditional double-row fixation fails in biomechanical studies at the footprint repair site.13,20
Despite the superior biomechanical properties of double-row fixation and its variants (M. J. Siskovsky et al, unpublished data, 2007),13,15,17,18,20,22 it is unclear if this translates to improved clinical results, and questions have been raised about resultant ischemia at the repair site. 21 Relatively few clinical studies exist using double-row fixation techniques, and even fewer are prospective comparisons.1,6,7,12,23,24 Two studies comparing single-row to double-row fixation with relatively short-term follow-up showed no differences in clinical outcome but found better tendon-healing rates for the double-row constructs.5,23 There are no clinical studies yet published for SutureBridge with PushLocks, the “transosseous equivalent,” or completely knotless repair constructs.
Efforts to simplify the technique for surgeons should not compromise the biomechanical properties of the construct, which may result in poor clinical outcomes or higher supraspinatus retear rates. Whereas a knotless lateral row for double-row fixation has been validated in a recent biomechanical study with the SutureBridge with PushLocks (M. J. Siskovsky et al, unpublished data, 2007), we found that the lack of medial row knots in the construct dramatically changed the biomechanical cyclic and failure characteristics, leading to greater gapping and decreased loads on failure testing. The medial row knots appear to protect the knotless lateral row, as shown by the lack of lateral row failure in group 1. Furthermore, although gap and displacement values were recorded for both groups, group 1 never had a true bone-tendon gap, as the tendon always remained in contact but displaced from the lateral edge of the footprint. Group 1 failures routinely occurred from the supraspinatus tendon shredding from the clamp (Figure 3A). In the 4 group 2 failures, the cuff glided on the bridging lateral row sutures as they slowly slackened out of the PushLocks of the lateral row (Figure 3B). After the sutures have pulled from the lateral row, the PushLocks ejected in 2 specimens. The behavior of the construct was more similar to a single-row supraspinatus repair in mode of failure. It is uncertain if the same conclusions can be extrapolated to other knotless repair constructs because they were not specifically tested.
Inherent in our study design are several weaknesses. By placing markers on the bursal surface of the supraspinatus tendon, we may not be adequately measuring the displacement of the deeper layers of the tendon during biomechanical testing. Furthermore, our study protocol does not account for rotational forces that occur in vivo. A rotational testing model may better represent the postoperative forces on the repair construct. 19 Use of 6.5-mm anchors is not typical in the clinical setting, but they were chosen to minimize the contribution of the humeral head bone density to the construct as is consistent with previous studies. Although dual energy X-ray absorptiometry (DEXA) scanning was not performed before testing for each specimen, each pair was divided into the 2 testing groups in an attempt to standardize the bone density quality. Experimental repairs were done without arthroscopic equipment; thus we were not specifically evaluating the arthroscopic technique. The infraspinatus was removed in this study to create a consistent 1-tendon tear model for repair with 2 columns of anchors and does not necessarily reflect large tears.
The greatest strength of this study design is the presence of a single variable of medial row knots in the repair construct design. Rather than compare a completely knotless repair construct to a traditional double row or a knotless lateral row construct such as the SutureBridge with PushLocks, we chose to study a repair construct with only 1 variable to allow more accurate conclusions.
Our study may raise concerns for the completely knotless rotator cuff repair systems, some of which use a similar concept of bridging suture knotless lateral row fixation of the SutureBridge with PushLocks. Double-row fixation suture-bridging techniques, based on this study model, should not be performed without suture knots in the medial row.