
Abstract
Background:
Adequate size matching and anatomically correct positioning must be recognized as essential factors influencing the outcome of meniscal transplantation.
Hypothesis:
Nonanatomical insertion and incongruence of meniscal transplants has an influence on the development of degenerative changes.
Study Design:
Controlled laboratory study.
Methods:
Ten female sheep were used for this animal study. Both knees (N = 20) were divided into 3 groups, subjected to either meniscectomy (group I; n = 10), to a medial meniscal autograft transplantation with a nonanatomical insertion of the anterior and posterior horn (group II; n = 5), or a meniscal autograft transplantation from the opposite knee as an incongruent meniscal autograft (group III; n = 5). After 6 months, radiographic (Fairbank's criteria), macroscopic (Jackson score), and histological evaluation by light microscopy (Mankin score) and scanning electron microscopy of the articular cartilage was performed.
Results:
All applied evaluation methods demonstrated that nonanatomical insertion of meniscal transplants resulted in the highest amount of degenerative cartilage changes. The histological assessment even revealed a significantly enlarged cartilage damage for the non-anatomic-positioned meniscal transplants in relation to the meniscectomized knees. Furthermore, the incongruent meniscal transplants demonstrated a significantly better cartilage situation than nonanatomically inserted meniscal transplants.
Conclusion:
The histological evaluation demonstrated clearly that a nonanatomically inserted meniscal transplant leads to degenerative cartilage changes that are worse than that after meniscectomy.
Clinical Relevance:
Precise anatomic positioning is mandatory for the potential chondroprotective effect of meniscal transplants.
During the past decades, the concept of meniscal replacement has become more common. 33 Allograft meniscal transplantation results in reduction of pain in the meniscectomized compartment and improvement of knee function in the majority of patients. The most important aim of meniscal replacement is the prevention of degenerative arthritis. Despite a lot of clinical follow-up studies that have been published since the first free meniscal transplantation in 1984, 33 clear evidence that meniscal replacement prevents the knee joint from postmeniscectomy degenerative arthritis is still missing. Different types of meniscus substitutes such as allografts, autografts (tendons, perichondral tissue, fat pad), biodegradable scaffolds, and prosthesis have been used in experimental and clinical studies.3,5,21,26,27,48,50,54 With regard to the graft material, to date, fresh-frozen allografts and cryopreserved allografts seem to provide the best a priori conditions for a possible prevention of degenerative arthritis. 42 Early experiences with meniscal transplantation already have given hints that fixation of the anterior and posterior horn insertions of the transplant at the wrong tibial location might be a cause for failure.24,25 Furthermore, congruence and correct size have been recognized as crucial outcome factors.10,18,25,48 A recently published biomechanical study demonstrated that meniscal transplants of a size + 10% of the original meniscus restore the contact mechanics close to normal, 10 yet exact positioning of the meniscal transplant is difficult. As pointed out in the literature, one possible reason for this is that the posterior horn might not be placed anatomically because the tibial eminence obscures the surgeon's view of the insertion site during the arthroscopic procedure. 45 A biomechanical study showed that nonanatomic placement significantly alters the load transmissions on the tibial plateau. 45 Furthermore, in a finite element model, the effect of geometric parameters of meniscal transplants on the contact behavior could be demonstrated. 18 To our knowledge, beside these in vitro studies, the influences of nonanatomic placement and incongruency of the meniscal transplants on the articular cartilage of the tibial head have not been investigated. The purpose of the present study is to evaluate the influence of nonanatomic positioning and incongruency of meniscal transplants on the tibial articular cartilage in an animal experiment.
Materials and Methods
Experimental Design
Ten female sheep (Ovies aries) with an average mass of 67.5 kg (range, 45–90 kg) were used. The study was approved by a local ethics committee according to the federal German guidelines. At the time of surgery, the sheep were between 2 and 2.5 y old. As in former animal studies, 34 the 10 animals were operated simultaneously on both knees. It could be demonstrated in a sheep experiment that there is no significant difference in lameness comparing total and hemi-meniscectomized knees at any day postoperatively. 47
The knees were divided into 3 groups (Table 1). Group I (n = 10) served as the control. In this group, a complete medial meniscectomy was performed at the left hindlimbs of the animals. In groups II and III, a medial meniscal transplantation with an autograft was performed. Thereby in group II, the meniscus was totally dissected from the knee joint. Immediately afterward, the resected meniscus was reinserted and refixated in defined nonanatomic position of the anterior and posterior attachment via bone tunnel sutures as an autograft (Figure 1).
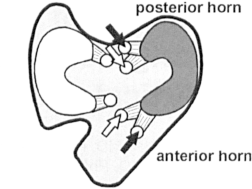
Schematic diagram of the nonanatomic position of the meniscal autograft in group II. White arrow, anatomic position; black arrow, nonanatomic position.
Distribution of Experimental and Control Groups
In group III, the medial meniscus that had been removed from the left knee joint was consequently used to replace the meniscus from the right knee as an incongruent autograft (Figure 2). This was performed immediately afterward. As in group II, fixation took place via bone tunnel sutures and refixation to the joint capsule. In this group, the original insertion sites of the meniscus at the anterior and posterior horn were used.
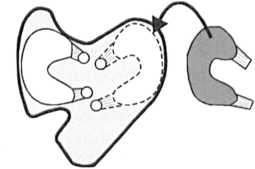
Schematic diagram of the incongruent meniscal transplantion in group III with the medial meniscus taken from the opposite knee.
The sheep were sacrificed after 6 months using an overdose (6 mL/50 kg body weight) of T61 Hoechst (0.2 g embutramid, 0.05 g mebezoniumjodid, 0.005 g tetracainhydrochlorid/1 mL). Next, the radiological, macroscopic, histological, and scanning electron microscopic (SEM) evaluation was performed by a blinded investigator.
Surgical Technique
The surgical procedure was performed with the animal under general anesthesia (Nembutal 600 mg intravenously and N2O/O2 3:1/Halothan 1–1, 5 Vol%). Before starting the surgical procedure, anterior-posterior view and lateral view radiographs were obtained of both legs. Then both hindlimbs were shaved, cleaned, and draped in sterile fields in a sterile operating theater. Antibiotic prophylaxis with a penicillin-streptomycin combination (Tardomycel 5–7.5 mL) was administered. All anesthesia was performed under veterinary control.
A medial parapatellar incision was used for arthrotomy. The medial collateral ligament was exposed. Its femoral insertion was detached with a 10 x 10 x 5 mm bone block. This allowed full access to the medial compartment of the knee and the meniscus. After the different surgical procedures in each group, the medial collateral ligament was reattached, and the bone block was fixed using a washer and a 6.5-mm cancellous AO-screw (Synthes, Switzerland) of 25 mm in length. The joint capsule, retinaculum, and subcutaneous tissue were closed with absorbable sutures (Vicryl 0 and 2–0; USP Ethicon, Norderstedt, Germany) and the skin with single stitches of nonabsorbable suture (Ethilon 2-0; Ethicon Inc, Somerville, NJ). This same surgical approach was used in all experimental and control groups (I-III).
In all groups (I-III) after the surgical approach, the medial meniscus was sharply dissected from the joint capsule, and from its insertional ligament at the anterior and posterior horn as well, using a scalpel. In group I, reattachment of the MCL and wound closure followed directly after meniscectomy as described.
In group II, the medial meniscus that had been removed was tagged with nonabsorbable sutures (Ethibond 2; Ethicon Inc) at the anterior and posterior horns. Nonanatomic insertions of the anterior and posterior horns were determined. The anterior attachment was placed 8 mm more ventrally and medially in a small groove, which is regularly found in the ovine knee joint. The insertion of the posterior horn was positioned 10 mm dorsally and medially of the original insertion (Figure 1). Bone tunnels of 2 mm in diameter were drilled from the ventral side of the tibia to the new anterior and posterior insertions of the meniscus with the help of an ACL drilling guide (Acufex; Smith & Nephew, Andover, Mass). The tag sutures were passed through the bone tunnels, and the meniscus was pulled into the medial joint space. After the tag sutures were passed through the tunnels they were knotted tightly together until the meniscal ligament came into contact with the bone tunnels. The meniscus was sutured to the capsule with 4 absorbable sutures (Vicryl 2-0; USP Ethicon, Norderstedt, Germany). Finally, the medial collateral ligament was reattached, and wound closure followed as described above.
In group III, the exact location of the meniscal insertions on the tibia plateau were subsequently marked with a sterile pen before removing the meniscus. Afterward, the medial meniscus of the opposite left leg, which had been removed before and stored under sterile conditions, was tagged with nonabsorbable sutures (Ethibond 2, Ethicon). Because both knees were operated on simultaneously, time between medial meniscectomy at the left hindlimb and reinsertion on the right hindlimb was less than 1 h. As described, 2 bone tunnels were drilled from the frontal side of the tibia, but in contrast to the former group (II), the bone tunnels were placed at the original insertions of the meniscus. The medial meniscal transplant of the opposite left knee had to be flipped over to serve as an incongruent medial transplant in the right knee. Consequently, the former femoral surface of the meniscus was located now on the tibia and vice versa (Figure 2). Fixation of the meniscus, reattachment of the medial collateral ligament, and wound closure was performed as mentioned.
The animals were allowed immediate free movement and weightbearing postoperatively and were not restricted in any way. The sheep were kept in sheds with 4 sheep per shed for the first 2 weeks. After the skin sutures were removed, the sheep were allowed to roam freely in a herd with sufficient space for running. Wound healing and gait were examined daily, pain medication (Temgesic 2 mL and Rimadyl 4.5-6 mL) and prophylactic antibiotics (5-7.5 mL penicillin-streptomycin combination) were given for 2 days postoperatively. All animal care was undertaken in accordance with the guidelines of the animal laboratory at our institution and under supervision of a veterinarian team.
Evaluation of the Specimen
Radiological Assessment.
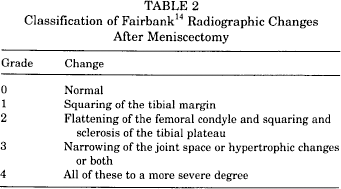
After sacrifice of the animals, non-weightbearing anterior-posterior and lateral view radiographs of the hindlimbs were taken. For this, the knees were manually held in a maximal extended position. The radiographs were assessed by a blinded observer according to the criteria described by Fairbank14,52 (Table 2) evaluating the degree of osteoarthritic changes after meniscectomy. Furthermore, joint space narrowing between the preoperative radiographs and radiographs after sacrifice (6 months postoperatively) was compared. Joint space reduction in percent was calculated using the preoperative and the postoperative joint space measurement in millimeters.
Classification of Fairbank 14 Radiographic Changes After Meniscectomy
Macroscopic Assessment.
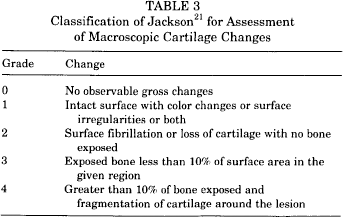
The joints were dissected with the femur separated from the tibia. The meniscus was left attached to the tibia plateau. Photographs were made perpendicular to the tibial plateau with and without the menisci in place. The morphologic evaluation of the cartilage changes on the medial tibial plateau was performed according to the classification of Jackson, 21 which differentiates between 5 grades of degenerative cartilage changes (grade 0 = no observable gross changes; grade 4 = greater than 10% of bone exposed) (Table 3). The photographs were reviewed by an investigator who was blinded to the surgical treatment.
Classification of Jackson 21 for Assessment of Macroscopic Cartilage Changes
Histological Assessment.
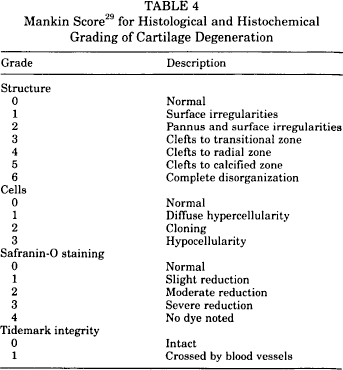
Three samples containing articular cartilage and subchondral bone of the medial tibial plateau were taken using a chisel to avoid heating artefacts from the oscillating saw in a standardized procedure. Each block measured approximately 3 x 3 x 15 mm. The tibial samples were taken from the anterior, middle, and posterior part of the tibial plateau (Figure 3). The blocks were fixed in 10% neutral buffered formaldehyde. Samples were decalcified using a chelating agent, embedded in paraffin, and cut in 5-um thick sections. The sections were stained with hematoxylin-eosin and with safranin O. Safranin O is a cationic dye that binds to the polyanions (chondroitin sulfate and keratine sulfate) of the cartilaginous ground substance in a stoichiometric fashion. Thus, the intensity of dye uptake reflects the concentration of proteoglycan in the tissue. 43 The cartilage sections were evaluated under a light microscope according to the histological and histochemical grading system of Mankin 29 (Table 4). As in the macroscopic evaluation, the histological sections were scored by an investigator who was blinded to surgical treatment. The mean value of the 3 samples of 1 knee was taken for evaluation.
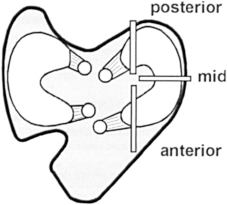
Schematic diagram of the tibial plateau from where the samples for the histological evaluation were taken.
Mankin Score 29 for Histological and Histochemical Grading of Cartilage Degeneration
Scanning Electron Microscopy (SEM)
The samples for the scanning electron microscopy were taken in the same size and region as the samples for the histological assessment (Figure 3). They were immersion-fixed immediately after removal in Karnovsky solution (3% formaldehyde, 3% glutaraldehyde-buffered 0.2M sodium cacodylate). They were rinsed in buffer, postfixed for 90 min in 2% osmium tetroxide solution, dehydrated in graded ethanols, and embedded in Epon. The blocks were cut into 1- to 2-μm thick sections and stained with an alkalinized toluidine blue solution. For enhancing contrast of the ultrathin sections, they were saturated with uranyl acetate followed by Reynold's aqueous lead citrate. The sections were examined with a Siemens 101 II electron microscope (Erlangen, Germany). The cartilage changes were graded according to a modified classification published by Hesse. 19 This classification differentiates between 5 degrees of cartilage degeneration taking changes at the superficial and deeper cartilage zones into account. As in the foregoing evaluation, the electron microscopy sections were examined by a blinded observer.
Differences between the treatment groups were statistically analyzed using the Mann-Whitney rank sum test for nonparametric variables SPSS (version 11.5; SPSS Science Inc, Chicago, Ill). Statistical significance was set at P ≤ .05.
Results
There were no visible intraoperative or early postoperative complications during the clinical follow-up of the animals. On dissection of the knee joints, there were no signs or other complications. Thus, all knees could be included in the evaluation. Also, all transplanted menisci were healed.
Radiological Results
Group II (nonanatomic insertion) had the highest degree of osteoarthritic changes (3.8 + 0.44; mean + standard deviation) (Figure 4). This group was followed by the meniscectomized knees (group I) with 3.5 + 0.53 points according to Fairbank's criteria. The least osteoarthritic changes were seen for the knees with the incongruent meniscal transplants in group III (2.6 + 0.89 points) (Figure 5). Statistical analysis demonstrated a significant difference between groups II and III (P < .05). Evaluation of joint space narrowing revealed a 19% reduction in group II with the nonanatomic position of the meniscal transplants, whereas in the meniscectomized knees (group I) and in the knees with the incongruent meniscal transplants (group III), a joint space narrowing of 7% or 6%, respectively, was found.
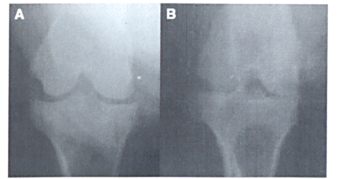
Radiographic example of a right knee preoperatively (A) and 6 months after transplantation of the meniscal autograft in a nonanatomic position (B).
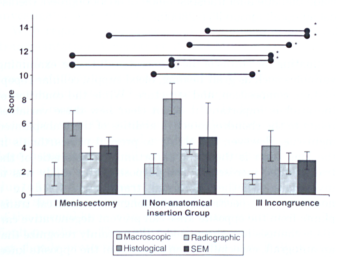
Mean score values (+ SD) of the histological, scanning electron microscopic (SEM), macroscopic, and radiographic cartilage evaluation considering their particular scoring system. *Indicates significant (P < .05).
Macroscopic Results
In group I with the total meniscectomized knees, the mean grading of the cartilage changes resulted in grade 1.73 + 0.99. Group II with nonanatomical insertion of the meniscal autograft revealed an average grade of 2.6 + 0.83—the highest degree of macroscopic cartilage changes (Figure 6). After meniscal transplantation with the incongruent autograft from the opposite knee (group HI), the cartilage changes were a mean of 1.27 + 0.45 (Figure 5). Even though the cartilage damage of the nonanatomically positioned meniscal autograft showed 2.6 + 0.83—the highest degree of cartilage damage in relation to the meniscectomized knees— the difference was not significant (P = .13). The cartilage situation between the meniscectomized knees and the knees with the incongruent meniscal transplants did not differ significantly either. Comparing the nonanatomically inserted meniscal autografts with the incongruent meniscal autografts, the incongruent ones had significantly less cartilage damage (P = .03).
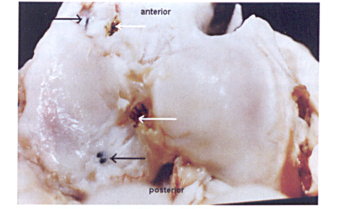
Example of macroscopic cartilage evaluation of a tibial plateau after nonanatomical insertion of the meniscal autograft in group II. White arrow, anatomic position; black arrow, nonanatomic position.
Histological Evaluation
The highest mean Mankin score was observed in the nonanatomically positioned autograft group (II) with 8.00 + 1.29 (Figure 7), followed by the meniscectomized group (I) with 5.97 + 1.05 (Figure 8), and the incongruent meniscal autograft group (III) with 4.07 + 1.26 points (Figure 5). In contrast to the macroscopic results, the comparison of the meniscectomized group (I) with meniscal autograft groups (II and III) revealed significantly less cartilage damage for the incongruent meniscal autograft group (P = .02) and a significantly inferior cartilage situation in the nonanatomically positioned meniscal autograft group (P = .01). In relation to the nonanatomically positioned meniscal autograft, the incongruent meniscal autografts also demonstrated significantly better results in the Mankin score (P = .01).

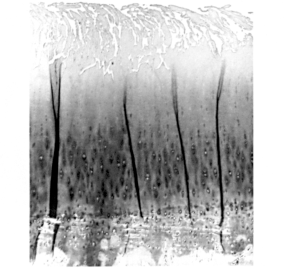
Histological example taken from group II with the nonanatomically inserted meniscal autografts. Deep clefts display severe degenerative changes. Magnification, 56x.
Histological example taken from the meniscectomized group. Magnification, 56x.
Scanning Electron Microscopy (SEM) Results
Corresponding to the radiographic, macroscopic, and histological assessment, group II with the nonanatomic position of the meniscal transplants proved with 4.80 + 2.98 points to have the highest degree of cartilage damage in the SE evaluation (Figure 5). Just as in the other measurements, group II was followed by the meniscectomized knees (group I) with 4.13 + 0.67, and the knees with the incongruent meniscal transplants (group III) with 2.87 + 0.73 points in the SEM assessment of the cartilage situation (Figure 9). Similarly to the histological cartilage evaluation, the results of the meniscectomized knees (group I) and the knees with the nonanatomic insertion of the meniscal allografts demonstrated a significantly inferior cartilage situation in relation to the knees with the incongruent meniscal transplants. The difference in cartilage damage between the meniscectomized and the nonanatomically positioned meniscal transplants was not significant.
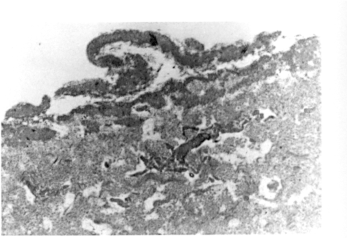
Scanning electron micrograph shows grade III cartilage damage after transplantation of an incongruent meniscal autograft (group III) (x28000).
Discussion
This study demonstrates in all applied evaluation methods steady succession of cartilage degeneration regarding the 3 experimental groups. The highest degree of cartilage damage or respective osteoarthritic changes was consistently found in group II with the nonanatomical insertion of the meniscal transplants, followed by group I with the meniscectomized knee. The lowest amount of cartilage changes was always found in group III with the incongruent meniscal transplants. Statistical analysis proved in all evaluation methods a significantly inferior cartilage situation for the nonanatomically inserted meniscal transplants compared with the incongruent meniscal transplants. The comparison of group II with nonanatomically inserted meniscal transplants with the meniscectomized knees (group I) displayed a significant increase in cartilage damage only in the histological evaluation. The incongruent meniscal transplant demonstrated in the histological, as well as in the SEM results, a significantly better cartilage situation in relation to the meniscectomized knees.
Previous studies using animal models to investigate meniscal allograft replacement have focused primarily on evaluating the status of the meniscal graft tissue, examining variables such as graft healing, blood supply, cellular repopulation, composition, and structure. ∥ While the condition of the graft is important, it is not clear how these variables relate to the chondroprotective abilities of the transplanted meniscus. However, the ability to prevent osteoarthritis in the long term is the most important characteristic of the transplanted meniscus. 12 The purpose of this study was to investigate whether meniscal transplants fixed in a nonanatomical position or as incongruent meniscal transplants from the opposite knee can prevent degenerative cartilage changes in a sheep model. We certainly recognize that an autograft, especially when taken from the opposite knee, would not be used clinically and constitutes a best-case scenario for meniscal transplantation. By using an autograft instead of an allograft, the effects of fixation were isolated from other confounding factors between donor meniscus and the original meniscus. These factors include reduced material properties due to graft-processing techniques.
References 4, 5, 7, 13, 21, 22, 27, 32, 33.
Meniscal allografts may be fresh, cryopreserved, fresh-frozen, or lyophilized. Lyophilized grafts have been found to undergo shrinkage, and knees with lyophilized meniscal allografts show degenerative changes comparable with meniscectomized knees in the long-term results. 57 Because autografts were used for this study, we were forced to perform the operations on both knees of the animals. In agreement with the experiences from other authors,34,47 the animals tolerated the operative procedures on both knees without any difficulties.
The relevance of using radiographs for the evaluation of degenerative cartilage or osteoarthritic changes after meniscal transplantation in animal studies is estimated differently in the literature. One of the arguments for not using radiographs is that weightbearing radiographs are required. Therefore, Edwards et al 11 constructed an animal study with a special jig to provide a constant compressive force and to standardize the radiographs. Yet it was demonstrated in an experimental study in rabbits that even with weightbearing radiographs, no correlation to the histological cartilage changes could be found. 31 Furthermore, with 6 months duration, the animal experiment is relatively short for expecting definitive radiological changes. But as far as a comparison with the literature is allowed corresponding to the results of the present study, none of the published animal studies found a significantly better radiological situation comparing meniscal transplanted knees with meniscectomized knees.16,35,40
Jackson et al 21 presented a standardized scheme for the macroscopic evaluation of meniscus and cartilage after meniscal transplantation. This classification is similar to the classification system of Outerbridge, 37 which is widely used clinically, and thus simplifies the transfer of the experimental results. When using photographs only, a visual evaluation of the cartilage is possible, whereas in clinical use the examiner can also palpate the lesion. We nonetheless accepted this limitation as a systematic circumstance to which the blinded investigator was subjected.
With regard to the macroscopic evaluation of meniscal transplantation, Arnoczky et al 5 and Mikic et al 32 reported some degree of cartilage protection after meniscal allograft transplantation in previous animal studies. These studies, however, did not grade or compare their observations with those of meniscectomized joints. 51 In the literature, differences between the meniscal transplantation groups and sham groups were found regarding the macroscopic cartilage assessment in all animal experiments.2,5,21,21,49,51,56 Some authors suspect that the extrusion of the menisci due to horn displacement is responsible for this. 2 The literature shows that the actual goal of restoring the conditions of the normal knee with a meniscal transplantation is difficult to achieve. The ability of the meniscal transplant to act chondroprotectively to some degree is well illustrated by the comparison with the meniscectomized knees.2,51 Precise positioning of the anterior and posterior horn seems to be mandatory for achieving an adequate pressure distribution by the meniscal transplant. Especially during arthroscopic implantation of meniscal allografts, the posterior horn might be placed in a nonanatomical position because the tibial eminence obscures the surgeon's view of the insertion of the posterior horn. In the present study, the sites of the nonanatomic placement, due to the length of the insertion ligaments of the ovine meniscus, allowed this malpositioning without stretching the body of the meniscus itself. A biomechanical study by Sekaran et al 45 clearly demonstrated that placement of the posterior horn in a nonanatomic medial location caused a significant increase in the normal maximum pressure over all flexion angles. This study recommends that the posterior horn tunnel of a meniscal transplant be placed within a tolerance tighter than 5 mm medial and 5 mm posterior to the anatomic location because nonanatomic placement significantly alters the contact pressure distribution. These findings are supported by the results of the present study demonstrating cartilage damage due to nonanatomic placement of the meniscal transplants comparable to meniscectomized knees.
Beside the problem of malpositioning, correct size matching is frequently quoted to be mandatory for a successful meniscal transplantation. It is speculated that a graft that is too small can be trapped beneath the femoral condyle and thus subjected to disproportionately high forces that predispose it to failure. Conversely, a large graft may have a loose fit around the femoral condyle, and therefore it can be mechanically ineffective. 30 Dienst et al 10 demonstrated in a biomechanical in vitro study that only a mismatch of less than 10% of the original meniscus might be acceptable. Several preoperative measuring techniques for correct size matching of the meniscal allografts have been introduced in the literature.8,17,20,38,46,53 In an anatomical study of meniscal allograft sizing, it could be shown that the meniscal dimensions can be predicted accurately from tibial plateau measurements. 30 The results of the present study support that geometric similarity is a very important factor for a successful result of meniscal transplantation.
The results of macroscopic evaluation of the incongruent meniscal transplants showed no significant improvement in the cartilage situation compared with the meniscectomized knees. These macroscopic findings are confirmed by a finite element analysis by Haut et al. 18 In this study, the sensitivity of the contact variables of the tibial plateau to the cross-sectional width and height of the lateral meniscus was determined. The results showed that contact variables are similarly sensitive to both the transverse and the cross-sectional parameters of the menisci. Additionally, the medial meniscus parameters have a greater effect on the contact variables than the lateral parameters. They found that a less than 0.5-mm change in the medial meniscal height and greater than 1-mm change in the lateral meniscal height could be tolerated before the relative difference in the contact variables exceeded 10% from those for the original geometry. This might explain the observation in the present study that the incongruent meniscal transplants revealed less cartilage damage than the meniscal transplants in the nonanatomic position, because by simply shifting or turning the transplants from the opposite knee, the height of the meniscal transplant had not been changed. Additionally, the position of the meniscal body was left unchanged. It might be suspected that this may also lead to fewer cartilage changes compared with the meniscectomized and nonanatomically positioned transplant group.
It is possible to detect cartilage degenerative changes by means of histological evaluation much earlier than is possible by macroscopic or radiological evaluation.31,55 Despite some difficulties associated with the Mankin score described in the literature,28,36 we decided to use it for the cartilage evaluation in the present study because the majority of published studies concerning the histological cartilage assessment after meniscal transplantation have predominantly also done so.1,9,12,23,35,41,51,56 Nevertheless, a direct comparison is still difficult because many variations of the Mankin score have been used. Corresponding to the macroscopic findings, most of the histological results in the literature demonstrated that the normal cartilage status of the knee cannot be restored by meniscal transplantation. There is only one exception in which a lateral meniscal transplantation was performed; the postoperative evaluation time was 4 months, which is relatively short. 23 In addition, there are some animal studies1,9 dealing with the histological cartilage evaluation after meniscal transplantation that show a chondroprotective effect, along with studies that did not even find a significant difference in comparison with meniscectomized knees12,35,51 (Table 5). The results of the present study revealed a significantly increased cartilage deterioration for the knees with the nonanatomically inserted medial meniscal transplants, whereas the incongruent medial meniscal transplanted knees showed a significantly better cartilage situation compared with the meniscectomized knees in the histological evaluation. This supports the opinion that an anatomic position is very important for the chondroprotective effect of a meniscal transplant.
Literature Review of the Histological Evaluation of Cartilage Degeneration After Meniscal Transplantation According to the Criteria of Mankin and Its Modification a
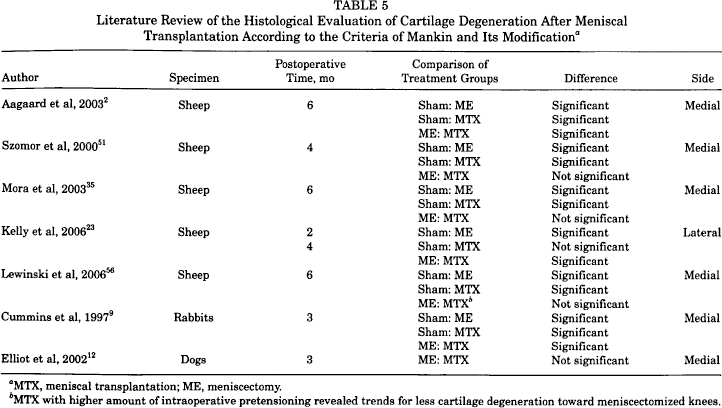
MTX, meniscal transplantation; ME, meniscectomy.
MTX with higher amount of intraoperative pretensioning revealed trends for less cartilage degeneration toward meniscectomized knees.
Compared with light microscopy, SEM is a relatively complex evaluation method that has been used only in a few experimental studies of meniscal replacement27,39 for the assessment of the meniscus substitute material itself. Cartilage evaluation with SEM after meniscal transplantation in clinical or experimental studies is rare. Contrary to our expectations, the cartilage evaluation by SEM seemed to be no more sensitive than the histological evaluation by light microscopy. We suspect a possible reason for this is the applied scoring system, which was mainly designed for very early degenerative changes, whereas the Mankin score allows a detailed evaluation of more severe degenerative changes.
In analyzing these results, we suggest that because of the nonanatomical insertion, the meniscal transplants no longer take up their load-bearing function. The study by Sekaran et al 45 has shown that a posterior and medial placement of the posterior horn caused the meniscal transplant to displace toward the periphery of the joint, causing the meniscus to become slack circumferentially. Inasmuch as the circumferential tensile modulus has been shown to be an important determinant of meniscal load sharing, 15 introducing circumferential slackness caused decreased load-sharing on this part of the meniscus. Furthermore, it is possible that due to its material properties, the nonanatomically inserted meniscal transplant acts as a kind of foreign body in the knee joint, which could explain the results of increased cartilage damage compared with the meniscectomized knees.
Even though the incongruent meniscal transplants with anatomical placements of the anterior and posterior horns demonstrated a significantly better cartilage situation than the meniscectomized and nonanatomic inserted meniscal transplanted knees, one has to be aware that a suture fixation cannot restore the complex structure and function of the meniscal attachment at the anterior and posterior horns. The natural attachment zones of the meniscus on the tibial plateau have uncalcified and calcified fibrocartilaginous zones. The border between the calcified fibrocartilaginous zones shows deep interdigitations increasing the contact area and the strength to resist shear and tensile forces.6,16,44 Gao et al 16 investigated the healing process of the anterior attachment of the medial meniscus during the first 12 wk in a rabbit model after sharp transection and refixation in a tibial bone tunnel. Normal insertion strength was not reestablished, and the failure load at tensile testing never reached more than 20% of a normal attachment. This can be supported by an ovine study investigating the influence of the intraoperative pretensioning on the meniscal transplant sutures, which confirmed that a certain intraoperative pretensioning on the tag sutures is necessary to achieve a chondroprotective effect of the meniscal transplants. 56
Conclusion
With the limitations of the present study in mind, it can be concluded that nonanatomic insertion of a meniscal transplant leads to even more severe cartilage damage than a complete meniscectomy. The histological results especially show that meniscal transplantation has a certain chondroprotective effect when the transplant is inserted in a precise anatomic position. The results from this animal study can be applied to clinical practice insofar as they suggest that accurate positioning of meniscal transplants has a major influence on the development of degenerative articular cartilage changes of the tibial plateau. However, the histological results especially demonstrate that meniscal transplantation has a possible chondroprotective effect when the transplant is inserted in a precise anatomic position.