
Abstract
Background:
When overhead-throwing athletes suffer from a rotator cuff tear, their ability to perform sporting activities is significantly impaired.
Hypothesis:
Arthroscopic rotator cuff repair allows amateur overhead-throwing athletes to return to their preoperative level of overhead-throwing sports.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Twenty-one overhead-throwing athletes (14 male and 7 female; average age, 58.9 years, range, 46–69 years) were reviewed for clinical outcome with the Constant Score and structural integrity of the repair on magnetic resonance imaging. The average follow-up was 25.7 months (24–29 months). Athletes were asked to retrospectively assess their sporting activity for pain, strength, endurance, and range of motion before onset of symptoms, preoperatively and at follow-up. They also were asked to evaluate their overall performance as a percentage of their original performance (0% to 100%). Retear rates and Constant Scores were compared with those of 32 patients who were not overhead-throwing athletes and who were operated on during the same time span.
Results:
Patients significantly improved their Constant Score from 54.9 to 84.2 (P < .001). Sporting activity was not significantly influenced by repair integrity; the retear rate was 23.8% (5/21). There was no significant difference for retear rate (25%; 8/32) or clinical outcome (Constant Score 84.5, P = .993) compared with patients who were not involved in overhead-throwing sports or any sports. All patients returned to their overhead-throwing sport an average of 6.3 months (3–12 months) after the surgery. Participation (2.1 per week) and duration (2.3 hours) of overhead-throwing activity postoperatively were not significantly lower than before the Patient was injured (2.2 per week, P = .290; and 2.4 hours, P = .285). Patients estimated their overall activity level to be 91.9% of their original, noninjured condition, which was significantly improved from the preoperative condition of 34.8% (P < .001).
Conclusion:
Arthroscopic rotator cuff repair led to good clinical results in this group of overhead-throwing athletes. Patients were able to return to overhead-throwing sports, most of them at the same preoperative level.
The rotator cuff is an important structure for the overhead-throwing athlete because it functions as the primary dynamic stabilizer of the shoulder and is put under continuous stress during throwing and other overhead-activity. The literature regarding rotator cuff injury and overhead-throwing athletes is focused on young professional athletes, mostly baseball players. In these cases repetitive microtrauma is considered to be the cause of rotator cuff injury. This repetitive throwing motion leads to posterosuperior impingement of the rotator cuff against the glenoid, which in turn can lead to articular-sided partial tears of the rotator cuff with accompanying lesions of the biceps such as superior labral anterior to posterior (SLAP) or Pulley lesions.8,18 These articular-side partial rotator cuff tears are considered typical for overhead-throwing athletes. Treatment options regarding the rotator cuff include arthroscopic repair if the tear consists of more than 50% of the tendon or simple debridement if it is less than 50%. A full-thickness tear is much less common in professional overhead-throwing athletes. When it occurs, however, this is often a career-threatening injury, as a recent report on professional baseball players showed. 10 Young professional athletes are not the only group of athletes most shoulder surgeons will treat for rotator cuff injury. Many patients involved in overhead-throwing sports will be active middle-aged patients involved in recreational or amateur overhead-throwing sports. These rotator cuff tears are often degenerative with underlying primary impingement. However, these patients are passionate about their sport and demand a successful return to activity.
Even for nonathletes, whether currently used arthroscopic rotator cuff repair techniques provide adequate repair strength is debated. 4 Although patient satisfaction is not based on the integrity of the repair, recent reports have shown that tendon integrity has a significant influence on abduction strength. 2 This could be significant, especially for the overhead-throwing athlete. To our knowledge, no study has addressed whether currently used arthroscopic rotator cuff repair methods are capable of restoring the ability to participate in overhead-throwing sports. We hypothesize that arthroscopic rotator cuff repair of isolated supraspinatus tears allows patients to return to their preinjury levels of overhead-throwing sports.
Materials and Methods
Patient Population
Patients for this study were selected from a group of 53 consecutive patients who received an arthroscopic repair of an isolated supraspinatus tear between 2000 and 2001. Exclusion criteria for this study were previous operations, tears extending to the infraspinatus or subscapularis tendon, adhesive capsulitis, or signs of infection. Patients were informed of the nature of the investigation and gave written consent for participation in this study. This group was prospectively followed for clinical outcome and repair integrity using MRI with a minimum follow-up of 24 months. The MRI results of these patients were published recently. 9
At the follow-up examination, patients who engaged in regular overhead-throwing activity were identified and retrospectively interviewed specifically regarding their sporting activity. The group of patients who did not perform any sporting activity or who performed sporting activities that do not require the use of the involved shoulder were excluded. Twenty-one of the 53 patients (39.6%) were included in the overhead-throwing athlete group; the other 32 became the non-overhead-throwing athlete control group. None of the identified patients were professional athletes. Their activity level was therefore rated either as amateur athlete if they were involved in regular competitive league or tournament play or as recreational athlete if they were not.
Clinical outcome was assessed using the Constant Score, which measures pain, activities of daily living, range of motion, and abduction strength. Abduction strength was measured using an Isobex dynamometer (Cursor AG, Bern, Switzerland). All patients were examined in the same open low-field MRI unit (0.2 T FA ESAOTE E-scan XQ, Esaote S.p.A, Genova, Italy) at our clinic to evaluate repair integrity at the time of follow-up. Regular MRI scans were obtained of the involved shoulder; no intra-articular gadolinium was used for this study. A retear was diagnosed if a signal consistent with fluid traversed the complete thickness of the supraspinatus tendon on at least 1 sagittal T2-weighted sequence according to established criteria. 12
Operative Technique and Postoperative Rehabilitation
Patients were operated in a standardized fashion by 1 of the 2 senior surgeons. While the patient was in a beach-chair position, a diagnostic arthroscopy of the glenohumeral joint was performed through a more superolateral posterior portal to evaluate the supraspinatus tear from the articular side and identify and address any labral, biceps, or other intra-articular lesions. The arthroscope was then moved to the subacromial space, and a thorough bursectomy followed by an acromioplasty without resection of the coracoacromial ligament was performed before the repair. The tear was then identified and prepared from the bursal side. For the repair, an additional posterolateral portal was established to complement the anterolateral portal already established for the acromioplasty. The supraspinatus tendon was released if necessary and the footprint was prepared with an acromionizer. If the tear shape required additional side-to-side sutures, these were placed and tied first. The tear was then reduced to the prepared footprint, and refixation was performed using bioabsorbable suture anchors preloaded with two No. 2 nonabsorbable braided polyester sutures (Biocorkscrew, FA Arthrex, Naples, Fla). For the repair, the modified Mason-Allen technique combining a mattress and a simple stitch was used to achieve a tension-free repair of the supraspinatus. 14
Postoperative rehabilitation protocol was identical for all patients. The patients were immobilized in an abduction pillow holding the arm in approximately 20° of abduction and 30° of internal rotation for 3 weeks. The pillow was gradually discontinued after 3 weeks. During the first 6 weeks, physiotherapy consisted of passive range of motion exercises for the shoulder. Range of motion limits were continuously increased from 60° of abduction, 60° of flexion, and 10° of external rotation in week 1 to 90° of abduction, 145° of flexion, and 45° of external rotation in week 6. Free passive range of motion was allowed at week 7, and isometric strengthening exercises were begun at week 9. Intensity of these exercises was increased to eccentric strengthening and weight training in week 12. Sport-specific exercises were begun after week 12, whereas return to overhead-throwing sports was advised no sooner than week 21.
Evaluation of Sporting Activity
For the retrospective evaluation, patients were asked to assess their sporting activity at 3 defined time points. The first time point was the preinjury level, when the patient was able to perform the sporting activity at the best of his or her ability without shoulder pain. The second time point was set before surgery, when the shoulder was painful. The third time point was the time of follow-up. At all 3 time points, the average number of times the sporting activity was performed during a week and the average amount of time spent were assessed. The patients were asked to evaluate 4 parameters subjectively at the different time points on scale of 0 to 10 points: Pain, strength, endurance, range of motion.
Finally, they were asked to evaluate their overall performance as a percentage of their original performance (0% to 100%).
Statistical Analysis
Statistical analysis was performed using the statistical software SPSS version 13.0 (SPSS Inc, Chicago, Ill). Level of significance was set at .05. Preoperative and postoperative nonparametric data from both groups were analyzed using the Wilcoxon signed rank test. Comparisons between the two groups were performed using the Mann-Whitney U test.
Results
For this study, we identified 21 patients who participated in overhead-throwing sports on a regular basis from a group of 53 patients prospectively followed up for clinical outcome and tendon integrity after arthroscopic supraspinatus tendon repair. The average age of the 21 overhead-throwing athletes was 58.9 years (range, 46–68 years) at the time of surgery; the group consisted of 14 men and 7 women. The average follow-up of this study was 25.7 months with a minimum of 24 months (range, 24–29 months). No postoperative complications were reported. Intraoperative findings are summarized in Table 1.
Intraoperative Findings a
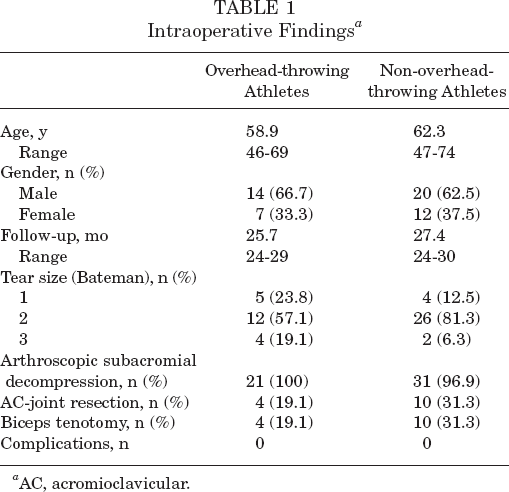
AC, acromioclavicular.
Analysis of the clinical results showed that, overall, patients were able to significantly improve all parameters of the Constant Score (Figure 1). In this respect, the results did not differ from the clinical results of the 32 patients who did not participate in overhead-throwing sports (Figure 2). Retear rate in the overhead-throwing athletes was 23.8% (5/21), which was also not different from the nonathletes (25%; 8/32). Of the 5 patients suffering from a retear 2 had a grade 1 retraction and 3 had a grade 2 retraction on the follow up MRI according to the Patte classification (13). The 3 patients who showed a grade 2 retraction according to the Patte 13 classification also had a lower Constant Score (74.7 points; P = .044). For these 3 patients, sporting activity level was 70%, which was not a statistically significant difference (P = .105). The 2 patients with a grade 1 retraction did not show inferior clinical results (83.9 points; P = .673) or lower activity levels (100%; P = .315) compared to the group with an intact repair.
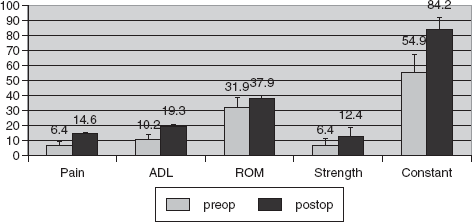
Preoperative and postoperative constant score of overhead-throwing athletes. ADL, activities of daily living; ROM, range of motion.
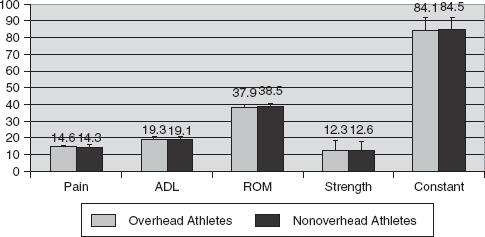
Comparison of clinical outcome between overhead-throwing athletes and non-overhead-throwing athletes. ADL, activities of daily living; ROM, range of motion.
The sports participation level was considered as amateur in 9 patients (42.9%) and as recreational in 12 patients (57.1%). At final follow-up, all patients had successfully returned to their sporting activities, which are listed in Table 2. The patients did so after an average of 6.3 months (range, 3–12 months) after the surgery. When the frequency and duration of the sporting activity were compared, there was a statistically significant decrease in frequency and duration from the healthy condition to the preoperative condition when the rotator cuff tear was symptomatic (P < .001 and P < .001). At final follow-up, no significant difference could be found compared with the original healthy condition (P = .290 and P = .285) (Figure 3).
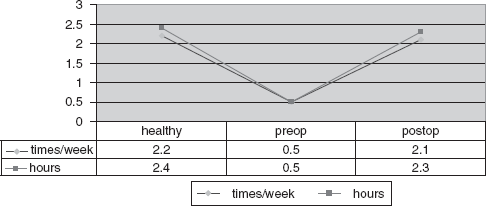
Frequency and amount of time for sporting activity.
Sporting Activities of the Study Population (N = 21)
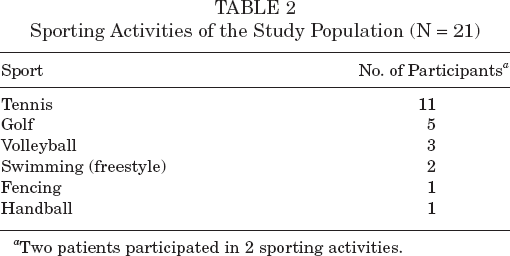
Two patients participated in 2 sporting activities.
Patients estimated their overall activity level at the time of follow-up to be 91.9% of the original healthy condition, which was significantly improved from the preoperative condition of 34.8% (P < .001). The 4 parameters of pain, strength, endurance, and range of motion were overall significantly improved from the preoperative state at final follow-up (Figure 4). Thirteen patients (61.9%) were able to reach 100% of their original activity level, whereas 8 patients were not able to return at 100%. These patients had problems in 1 or more of the evaluated parameters. Pain was a problem in 3 patients, strength was an issue in 5 patients, endurance was a problem in 4 patients, and range of motion was a problem in 4 patients.
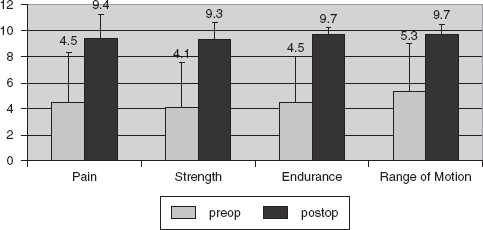
Comparison of preoperative and postoperative subjective sporting ability.
As stated above, 5 patients (23.8%) suffered a retear as revealed by MRI at the time of follow-up. The difference in the sporting activity from the rest of the group was not statistically significant; however, the 2 patients with the worst results from the study group regarding sporting activity both suffered a retear. These 2 patients, who were both tennis players, estimated their activity level at 50% and 60% of the original activity level. Both patients were otherwise pain free and therefore reluctant to undergo revision surgery, which was discussed as an option at the time of follow-up. The other 3 patients suffering from a retear all had subjectively recovered to 100% of their original activity in golf, swimming, and volleyball.
Four patients did not follow our rehabilitation protocol and returned to overhead-throwing sports before week 21. These patients had a significantly lower constant score of 76.8 points compared with 85.9 points for the rest of the group, who followed the rehabilitation protocol (P = .039). However, only 1 patient suffered a retear (25%), which means the retear rate was not significantly increased. Also, sporting activity was not rated significantly lower for patients returning early (98.75% vs 90.29% in the compliant group, P = .383).
Because all patients were amateur or recreational athletes, we looked at a possible influence of the patient's occupation. Seven patients (33.3%) were manual workers. There were no significant differences in the Constant Score, which was 87.5 points compared with 82.4 points for patients not involved in manual work (P = .156). Overall activity level was 94.3% for the manual workers compared with 90.7% for the non-manual workers (P = .608).
Analysis of gender differences showed that women estimated their overall activity level to be significantly higher (98.6% vs 88.6%) than male athletes (P = .007). When we analyzed the single parameters, women did worse regarding pain. However, they did better regarding endurance and range of motion (Figure 5).
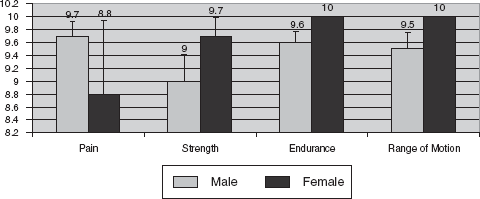
Gender differences in subjective sporting activity.
Patients fared better if the dominant arm was involved. Overall activity level was significantly better for the dominant arm at 95.0% versus 85.7% for the nondominant arm (P = .008). This difference was also significant for every single parameter evaluated (Figure 6).
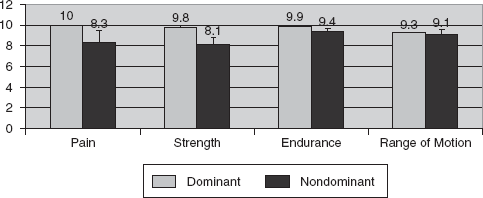
Differences between dominant and nondominant arm in subjective sporting ability.
Discussion
There is a strong contrast between the recreational and the professional athlete in the literature regarding treatment of complete rotator cuff tears. For the young professional overhead-throwing athlete, a complete tear of the rotator cuff is rare. The few reports of complete tears in professional athletes involve a traumatic event in a contact sports situation. Goldberg et al 6 reported on 6 elite rugby players suffering from a large rotator cuff tear from a traumatic shoulder dislocation. The investigators performed a 2-stage open operation, treating the rotator cuff tear first and then conducting an open stabilization procedure about 10 weeks later. All patients described the outcome as successful and were able to return to their sport. Return to sports has been far more difficult for professional overhead-throwing athletes. Tibone et al 16 followed 45 athletes after open rotator cuff repair for either partial-thickness (n = 30) or full-thickness rotator cuff tears (n = 15). After an average follow-up of 42 months, 25 patients (56%) had returned to their sport at their original competitive level without significant pain. The authors concluded that rotator cuff repair with anterior acromioplasty does not guarantee a return to the original competitive level of sports. In a recent retrospective review, Mazoue and Andrews 10 reported on 16 professional baseball players treated with an open rotator cuff repair from 1995 to 2003, which underlines how rare a complete tear is in this patient group. Twelve of these baseball players were pitchers, and only 1 was able to return at a high competitive level for more than 6 months; 5 of those pitchers never played a professional game after surgery. The authors concluded that it is very difficult to return to baseball, especially pitching, after rotator cuff tear.
High-level athletes who experience rotator cuff tear have a dramatically inferior prognosis for returning to sports compared with middle-aged recreational athletes. This is reflected in the few studies on this subject that can be found in the literature. Sonnery-Cottet et al 15 looked at results for 51 middle-aged (average age 51 years) amateur tennis players with open rotator cuff repair (n = 42) or arthroscopic debridement with or without biceps tenotomy. Their return rate to tennis was 80% (n = 40) after an average of 9.8 months after surgery. No difference was found in the ability to return to tennis between the open repair and the debridement group. However, the authors did not conclude that debridement was equivalent to open repair. This is reflected to some extent in our findings that patients who had suffered a retear successfully returned to their sporting activities. Bigliani et al 1 showed that in active tennis players with an average age of 58 years, only 1 of 23 (4%) had an unsatisfactory result after open acromioplasty and rotator cuff repair and was not able to return to tennis.
Similarly good results were found by Vives et al 17 for a group of 29 amateur golfers undergoing open or mini-open rotator cuff repair at an average age of 60 years. Only 3 patients (10%) did not return to golf; 26 of 29 were playing golf without loss of handicap or driving distance.
To our knowledge, there are no reports documenting tendon integrity and return to sports after arthroscopic rotator cuff repair. Rotator cuff repair is on the verge of transitioning from open and mini-open to all-arthroscopic techniques. 19 Although the clinical results available seem to be equal to the results of open and mini-open repair, concerns have been raised about repair stability and long-term integrity. 4 For a patient planning to return to an overhead-throwing sport after surgery, this is certainly a major issue. As a result, surgeons might tend to use open repair techniques in overhead-throwing athletes until biomechanically stronger arthroscopic repair techniques such as double-row repair prove their clinical and structural superiority. After switching to all-arthroscopic repairs, we have gradually begun to treat all our patients arthroscopically, regardless of involvement in sports. At 2 years postoperatively, all of our patients were able to return to their respective sporting activities but some did so at lower activity levels. Two patients, both of whom suffered a retear, were not satisfied with their postoperative level of play. The retear rate that we found for our arthroscopic repairs compares well with the rates reported in the literature for open and arthroscopic repairs of isolated supraspinatus tears.2,3,5,7,11
A specific weakness of our study is that the retrospective collection of sports participation information may be subject to recall error. In addition, our subjects were a rather inhomogeneous group of athletes from 6 different sports. Including golf in the mix of overhead-throwing sports is debatable, because some do not consider it an overhead-throwing activity. However, there is no doubt that golfing puts stress on a shoulder, and it is a very popular sport for players of the age we studied. Therefore, we believed it appropriate to include the results of our golfers in this study.
Our conclusion from this study was that arthroscopic repair of isolated supraspinatus tears led to good clinical results in this group of recreational and amateur overhead-throwing athletes. All patients were able to return to overhead-throwing sports, most of them at their preoperative level.