
Abstract
Background: Transtendinous repair is a well-known technique for the arthroscopic management of partial rotator cuff tear. However, there are not a lot of clinical follow-up studies in the literature reporting data on this approach, and, moreover, potential factors responsible to influence the outcomes have not been investigated.
Purpose: To evaluate clinical outcomes after arthroscopic transtendinous repair and to identify predictive factors of residual shoulder symptoms.
Study Design: Case series; Level of evidence, 4.
Methods: Fifty-four patients with a mean age of 56.7 ± 8.8 years (range, 31-71 years) who had undergone an arthroscopic transtendon repair for a painful articular-sided rotator cuff tear with a minimum of 2 years of follow-up were contacted. Clinical outcomes using a patient-based questionnaire, the Constant score, University of California at Los Angeles score, Simple Shoulder Test, and visual analog scale were evaluated. The influence of patient age, presence or absence of a trauma responsible for the cuff tear, presence of associated shoulder lesions, millimeters of exposed footprint, and millimeters of torn tendon retraction on the outcomes were assessed.
Results: The mean cuff tear exposure footprint was 5.2 mm, and the mean retraction of the torn part of the tendon was 8 mm. Only one patient reported dissatisfaction with surgery because of persistence of pain during overhead activities. After arthroscopic repair, University of California at Los Angeles, Constant, and Simple Shoulder Test scores were significantly improved from 14.1, 45.3, and 9.8 to 32.9, 90.6, and 0.8, respectively (P < .001). Twenty-two patients (41%) reported occasional shoulder discomfort at the extremes of range of motion (particularly at extremes of abduction and internal rotation) occurring during some daily living and sports activities. The best multivariate model showed that residual shoulder discomfort is strongly linked with a partial thickness supraspinatus tendon avulsion-type articular-sided rotator cuff lesion consisting of a large tendon retraction and/or a relatively small exposure footprint area in an older patient in the absence of a specific trauma (P < .001).
Conclusion: Arthroscopic transtendon partial articular supraspinatus tendon avulsion-type rotator cuff repair was a reliable procedure that resulted in a good outcome in terms of pain relief and shoulder scores in 98% of the 54 patients. Better results could be expected in patients with less tendon retraction, a larger footprint exposure, of younger age, and with a clinical history of trauma.
Keywords
Since the original description of partial rotator cuff tears, considerable attention has been given to their diagnosis and management. The pathogenesis of these lesions includes intrinsic degeneration, extrinsic impingement, trauma, microtrauma, or a combination. 31 Partial rotator cuff tears may occur on the bursal side, within the tendon, or on the articular side, depending on the anatomical and biomechanical situation. Articular-side partial cuff tears are 2 to 3 times more common than bursal-sided lesions,4,11,17 especially in throwing athletes, and articular surface tears have shown a high percentage of intratendinous extension. 3
With the advent of magnetic resonance imaging (MRI) and arthroscopy, articular partial-thickness cuff tears have become better understood. Ellmann 8 classified partial cuff tears based on location and graded these lesions with measurements of both the depth and the area of the defect. In an effort to simplify lesion description and facilitate communication and, thereby, decision-making, Snyder et al 29 proposed a more comprehensive system that allows a systematic classification of the intraoperative findings, assigning a letter for each location and a number for grade.
Millstein and Snyder 22 described the partial articular supraspinatus tendon avulsion and coined the acronym PASTA lesion to indicate this particular partial cuff tear. However, at present there is no widely accepted classification system and treatment paradigm for partial-thickness articular-side rotator cuff tears. Recently, some authors have outlined the importance of evaluation of the rotator cuff footprint to better assess the depth of the partial cuff tear defect.6,27 In practice, the depth of the partial tear can be judged by the amount of exposed “footprint,” allowing the surgeon to estimate the severity of the tear and to choose the most logical treatment. 27
Some authors have recommended rotator cuff repair for high-grade partial articular rotator cuff tears. Good or excellent results have been reported with treating partial-thickness tears by completing them to full-thickness tears and then repairing the entire tendon.3,11,13,14,16,24,34,35
An alternative surgical approach was suggested by Snyder. 28 He proposed an arthroscopic transtendon technique for treating significant partial articular-side rotator cuff tears with the intention of restoring the torn surface to its native footprint area on the tuberosity, while preserving the remaining normal attachment of the tendon fibers on the bursal side. To date, there are few studies in the literature reporting data on this approach.15,18,30 To our knowledge, no studies report the effect of patient-related factors on patient outcomes. The purpose of the present study is to evaluate the clinical outcome in a series of patients with painful partial articular cuff tears treated with the arthroscopic transtendinous repair and to attempt to identify factors to predict residual shoulder symptoms, thereby improving patient selection and clinical outcome. Our hypothesis is that this repair technique is a reliable procedure that can be expected to improve symptoms in patients suffering from partial articular cuff tears.
Materials and Methods
Retrospective database review was performed on all patients treated with arthroscopic transtendinous cuff repair in the period between 2004 and December 2005. A total of 70 consecutive patients were identified. Of these patients, 54 (77%) were successfully contacted and were able to return for clinical follow-up. Sixteen patients could not be contacted or were unable to return for assessment. Eleven patients were lost because of address and phone number changes, and 5 patients refused to participate in this study. For each of the 54 remaining patients, data related to clinical history, preoperative medical evaluation, and intraoperative findings, including type of cuff tear described according to the Snyder classification 22 –particularly, we considered A2 as a failure of some rotator cuff fibers, usually <2 cm; and A3 as a more severe rotator cuff injury involving the whole articular surface of the rotator cuff tendon, usually <3 cm—grade of tendon retraction (expressed as a distance in millimeters between the anatomical point of tendon insertion on the humeral head and the edge of the cuff tear calculated using a 5-mm tip of probe), and grade of cuff tear exposure footprint (millimeters of thickness [depth] of the tear), were retrieved from the medical record. Particularly, the footprint exposure was evaluated after debridement of the cuff tendon remnants by using the known width of 3.5-, 4.5-, or 5.5-mm full-radius shavers, compared with the size of the footprint exposure (Figure 1).
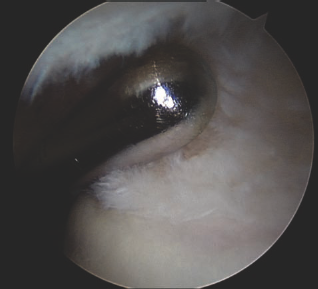
Intra-articular arthroscopic view of a right shoulder showing the measurement of a footprint exposure using a 3.5-mm tip of a full radius shaver. In this case a 4-mm footprint exposure was calculated.
Of the 54 study patients, there were 28 men and 26 women with a mean age of 56.7 ± 8.8 years (range, 31–71 years). Forty-four cases involved the right shoulder, and 10 cases were left shoulders. The injured shoulder was the dominant side in all but 2 cases.
Before surgery, all patients had pain aggravated by overhead activities. Night pain was present in 43 (80%) patients. Twenty-one patients were involved in overhead sports (14 tennis, 7 basketball), 11 patients had a history of minor trauma (a fall in 9, motor vehicle accident in 2), 7 patients had an overuse injury from heavy manual labor, and the remaining 15 patients had an insidious onset of symptoms without any history of trauma.
All patients underwent an unsuccessful minimum 4-month course of conservative treatment consisting of activity modification, anti-inflammatory medication, and a physical therapy and exercise regimen before undergoing surgery.
Preoperative and postoperative evaluation consisted of patient-based questionnaire and physical examination performed by an independent, experienced physician. Clinical assessment consisted of the measurement of glenohumeral range of motion (ROM) using a goniometer, and muscle strength testing using the Lafayette Manual Muscle Test System (Lafayette Instrument Company, Lafayette, Indiana). The Constant rating score as originally proposed by Constant and Murley, 2 University of California at Los Angeles (UCLA) score, and Simple Shoulder Test (SST) as reported by Matsen et al 20 were assessed. Pain was recorded using the visual analog scale (VAS); a score of 0 indicated no pain, and 10 points indicated the worst possible pain.
All patients underwent preoperative radiographs (anterior-posterior, axillary, and arch view) and MRI evaluation. The MRI studies revealed a partial-thickness tear of the rotator cuff at the articular side in all patients.
Cuff tears were repaired with an arthroscopic transtendon (PASTA) repair as described by Snyder. 28 Surgical procedures were performed by the senior author with the patient in a lateral decubitus position using a single titanium suture anchor (Fastin; DePuy-Mitek, Norwood, Massachusetts) loaded with two No. 2 Ethibond or Orthocord sutures (Fastin; DePuy-Mitek). The anchor was placed percutaneously through the remaining tendon into the bone of the decorticated rotator cuff footprint. A spinal needle loaded with a No. 1 monofilament absorbable suture (PDS; Ethicon, Norwood, Massachusetts) was introduced percutaneously lateral to the edge of the acromion. It was passed through the bursal side of the remaining cuff and through a healthy portion of the articular tendon. The suture was used to “shuttle” the 2 anchored sutures through the edge of the partial cuff tear. The sutures were retrieved and tied in the subacromial space (Figure 2). In all cases included in this study, one anchor was used to perform the repair.

Intra-articular arthroscopic view of a right shoulder from a posterior portal showing the repair of rotator cuff tear with a good restoration of the cuff footprint.
Postoperative Care
In the operating room, the operated arm was placed in an UltraSling brace (DJ Ortho, Carlsbad, California) with 0° of external rotation and 15° of abduction and worn for 4 weeks. All patients followed a standard postoperative rehabilitation protocol supervised by one of the authors. After one week, supervised gentle physical therapy consisting of passive pendulum and gradual passive range of motion (PROM) and trunk and scapular exercises was begun. After 6 to 8 weeks, scapular stabilizer strengthening exercises using isometric contractions and resistance bands were started, and at the same time the PROM recovery was gently performed with land and water therapy. After 12 weeks, a gentle strengthening of the cuff was begun, limiting active exercise in abduction to 30° to 60° to avoid stressing the cuff repair. Full exercise force was allowed after 4 months. Initial progress required no pain with internal and external rotation before active abduction exercises were begun. Sports activities were allowed at 5 to 6 months after surgery. Patients were reviewed at a mean follow-up of 2.7 ± 0.8 years (range, 2-3.8 years).
Data Analysis
All statistical analyses were performed by a biostatistician using S-Plus version 7.0, Enterprise Developer (Insightful Corporation, Seattle, Washington). Student t tests or Wilcoxon tests were used to test differences between preoperative and postoperative values of ROM, VAS, UCLA, SST, and Constant scores. A significant difference of results was considered when the corresponding P value was below the standard threshold of .05.
A stepwise, multivariate, logistic regression analysis based on the Aikake information criterion was used to find a correlation between the outcome measures (residual shoulder symptoms referred by the patients) and the following covariates: age, presence of trauma in the clinical history, presence of associated shoulder lesions, millimeters of exposed footprint (depth of tear), and millimeters of tendon retraction as measured during surgical procedures and reported on the database.
Results
No intraoperative complications occurred in this group of patients.
According to the Snyder classification system, 29 13 tears were graded as A2, 22 as A3, and the remaining 19 as A4 lesions. The cuff tear exposed a portion of the bony footprint varying between 4 mm and 7 mm (mean, 5.2 mm). Retraction of the torn portion of the tendon was found in all cases, ranging from 5 mm to 20 mm (mean, 8 mm).
Eighteen patients had associated shoulder lesions, including 12 cases with long head biceps (LHB) tendon lesions (5 dislocations, 5 wear, 2 avulsions), 3 cases with tearing of the superior margin of the subscapularis tendon, and 3 cases with a type II superior labral anterior posterior (SLAP) lesion. In these patients, associated surgical procedures were performed at the time of cuff repair, including 12 cases of a LHB tenotomy, 3 cases of a suture of the upper margin of the subscapularis, and 2 cases of SLAP repair.
The level of pain improved significantly in all patients at follow-up. However, one patient was unsatisfied with surgery because of persistence of pain during overhead activities. This patient refused further evaluation, including ultrasound, MRI, or physical therapy. The VAS score decreased from a mean preoperative value of 5.7 points (range, 4–10) to a mean value of 1.3 points (range, 0–5).
At final follow-up, we observed a statistically significant improvement of UCLA, Constant, and SST scores and ROM. Specifically, UCLA rating scores improved from a mean preoperative value of 14.1 (range, 7–20) to a postoperative value of 32.9 (range, 22–35). The initial Constant score was 45.3 (range, 15–67) and improved to 90.6 (range, 40–100). The SST score (referring to pain or limitation in activities of daily living) improved from a mean of 9.8 (range, 8–12) before arthroscopic repair to 0.8 (range, 0–5) after repair.
Table 1 summarizes preoperative and final follow-up values of ROM and shoulder scores.
Preoperative and Final Follow-up Score Expressed in Mean ± Standard Deviation (N = 54) a
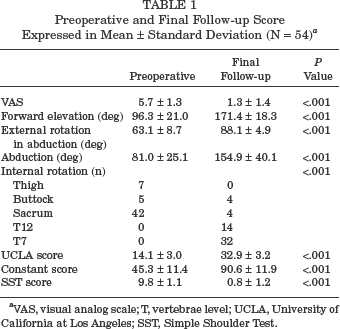
VAS, visual analog scale; T, vertebrae level; UCLA, University of California at Los Angeles; SST, Simple Shoulder Test.
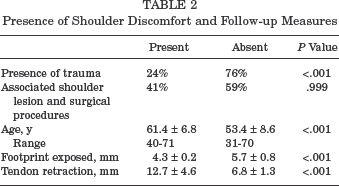
At follow-up, we identified 22 patients (41%) with residual complaints of occasional shoulder discomfort at the extremes of ROM (particularly abduction and internal rotation) occurring during some daily living and sports activities. Although no patient reported pain at rest, the analysis of data shows that the group of patients with occasional shoulder discomfort scored lower on all of the outcome scores than the other patients. However, the difference of scores between the 2 groups was not significant. Table 2 summarizes the covariates the authors considered at final follow-up separated by the presence or absence of reported shoulder discomfort.
Presence of Shoulder Discomfort and Follow-up Measures
The best multivariate model found to predict the presence or absence of shoulder discomfort was the millimeters of exposed bony footprint (depth of tear) and millimeters of tendon retraction Therefore, a high probability of shoulder discomfort is most often found in cases with a large tendon retraction or in cases with a small cuff tear exposure footprint area.
Given the results displayed in Table 2, the age factor was also incorporated into the multivariate model. In such a situation, the best model found takes into account the age of the patient, presence or absence of trauma, and millimeters of tendon retraction as factors influencing the presence of shoulder discomfort at follow-up. This result is coherent with the previous model, because a small millimeter of footprint exposure is correlated with a higher age (P < .001) and the absence of trauma in clinical history (P < .001).
Discussion
In this study we reviewed a group of 54 patients who underwent an arthroscopic transtendon repair for partial-thickness articular-side rotator cuff tears. None of these patients showed any concomitant bursal-side cuff injury.
Patients were evaluated after a minimum of 2 years, and all but 1 was satisfied with surgery. In 18 patients (33%), we found associated shoulder lesions that were treated during the same surgical procedure.
Partial-thickness rotator cuff tears represent a very interesting topic of discussion in the literature, particularly related to pathogenesis, classification, and management.
The pathogenesis of these lesions includes intrinsic factors such as age-related degenerative changes, extrinsic factors such as subacromial impingement, trauma, and microtrauma resulting in an overload of the articular side of the tendon, or a combination of all these causes.1,5,10,14,21,31,32 In our series, 15 patients (28%) reported an insidious onset of symptoms without any history of trauma, while in the other 39 patients (72%), a history of trauma or repetitive microtrauma was identified as a probable cause of the tear. It was not possible to accurately determine the potential influence of intrinsic cuff degeneration or specific anatomic changes that may play a role in causing a partial articular cuff tear. On the other hand, Millstein and Snyder 22 stated that an isolated trauma or repetitive microtrauma can result in a partial cuff lesion consisting of an avulsion and retraction of the articular surface of the cuff; they termed this lesion a PASTA lesion. Previously, Ellman 8 noted that in cases of partial-thickness tears, the most inferior articular surface fibers demonstrate the greatest degree of retraction. Therefore, grading of partial articular tears should include quantifying the exposed bone at the tendon footprint. 27 This is a relatively new concept,6,15,27 and because not all articular partial cuff tears are alike, it is reasonable to assume that different types of surgical management should be proposed. A direct comparison of the results with the studies reporting treatment of partial articular cuff tendon tears is very difficult.
Mixed results have been reported in the literature following simple debridement of partial-thickness cuff tears.9,21,23,26,33 Arthroscopic debridement combined with subacromial decompression also led to variable results.5,10,12,16,25,34 However, it seems that the cause of poor results is related to failure to address concomitant shoulder diseases and to debride higher grade partial cuff tears without surgical repair.
Concerns about residual cuff integrity and potential tear progression prompted recommendations for repair of extensive partial rotator cuff tears.8,14,34 The meaning of an extensive tear is not standardized in the literature because a reproducible classification system for partial articular cuff tears is lacking. Furthermore, the normal footprint thickness can be variable.15,27
In our study, patients with an avulsion of footprint equal to or greater than 4.0 mm underwent a cuff repair.
In 1999, Weber 34 reported the results from a series of 2 groups of patients with a deep partial rotator cuff tear involving ≥50% of the thickness of the rotator cuff treated with arthroscopic debridement and acromioplasty or with mini-open repair. He showed a significantly worse outcome in patients treated with arthroscopic debridement alone and recommended rotator cuff repair in patients with tears ≥50% of the thickness of the rotator cuff. Fukuda et al 12 reported satisfactory results in 94% of patients with partial tears treated with open acromioplasty and cuff repair. Wright and Cofield 35 also reported good results in patients with partial tears treated with open repair. Recently, Deutsch, 7 who prospectively evaluated clinical outcome following arthroscopic repair of partial-thickness tears, reported satisfactory results in 98% of the patients.
In the past years, different arthroscopic techniques for repair of partial cuff tears have been reported. Lyons et al, 19 attempting to avoid further progression in selected partial articular cuff tears, proposed a debridement of the greater tuberosity adjacent to the tear and a side-to-side stitch passed through the supraspinatus and subscapularis tendon. This technique placed the debrided tendon against the humeral bone bed, but no clinical results have been published. Snyder 28 first, and later Lo and Burkhart, 18 proposed a transtendon arthroscopic repair. The purpose of this technique is to avoid removing normal, healthy, residual bursal-sided cuff tissue to complete the tear and repair only the deeper portion of the cuff to the greater tuberosity. In this manner, the medial aspect of the footprint is restored while preserving the intact lateral tendon. This reestablishment of the normal footprint of the rotator cuff potentially minimizes any length-tension mismatch of the repaired cuff. 18 Although during some maneuvers performed in this surgery, such as passage of bone punch and inserting the anchors, the intact cuff could be damaged, no intraoperative complications were reported in our series, and in the final analysis, we obtained a good repair in all cases. Clinical outcomes reported in our study, as in others, 15 show a good reliability of this surgical technique.
One of the questionable aspects of this study can be related to the grade of lesion treated. The consensus in the literature seems to be that a partial lesion deeper than 6 mm (50%) should be repaired. In our study, patients with an exposure of 4.0 mm of footprint also underwent a rotator cuff repair. Looking at Snyder's classification, 29 13 patients (24%) with an A2 lesion were included in our series. These indications seem to be different from those of the other studies, and it could appear that some patients included in our series were overtreated. However, as mentioned earlier, it is difficult to compare these findings because there is no reproducible classification system for partial articular cuff tear, and determining the grade of tendon involvement can be difficult at the time of arthroscopy. Moreover, the footprint thickness can be different among individuals, and 4 mm of exposure can represent also the 50% of the footprint in some smaller patients. 15
An interesting finding of our study that has not been previously reported was the presence of a shoulder discomfort in 22 patients during activities involving extreme internal rotation and abduction. We found this discomfort in patients having only a small area of footprint exposure or with a large degree of tendon retraction and degenerative tears, especially in the older age group. In light of these results, even though these patients were generally satisfied with their surgical result, the presence of tendon retraction, particularly in older patients with a no traumatic onset of shoulder symptoms, leads us to assume this surgical technique may not be the preferred treatment. It is possible that a partial cuff tear with significant retraction of the articular layer undergoes more traction on the original footprint zone and causes some discomfort. Furthermore in these cases, the bursal layer of the cuff may be bunched up after transtendon repair and cause residual shoulder discomfort. It may be preferable in these cases to complete the cuff tear and repair the tendon in a more medial position to avoid any residual discomfort. The only patient unsatisfied with surgery in our series was older than 50 years and had a large tendon retraction.
However, a control group in which the lesion was completed and the tendon reattached in a more medial position is lacking in this study, so it is not possible to make a definitive conclusion.
The same concern is applicable to the millimeters of footprint exposure. The analysis of our results shows that shoulder discomfort was found also in patients with a small footprint area exposure. Transtendon cuff repair was performed in patients having only 4 mm of footprint exposure. We suppose that in these cases the tendon may have undergone additional traction when repaired on the original footprint, independently from the grade of retraction. However, it is difficult for the surgeon to is establish the depth of cuff for each individual. In fact, the studies on the footprint have shown that it is variable; 4 mm of footprint exposure can correspond to just 50% of exposure in some individuals. We did observe that in cases of small footprint exposure, the surgeon will sometimes pass the sutures through the intact rotator cuff cable, thereby advancing it to the bony footprint. It is possible that this nonanatomical placement could cause high stress in this zone and be responsible for the shoulder discomfort.
One obvious weakness of this study is the absence of a control group treated in a different way; it was a retrospective study, and 23% of patients were lost at follow-up. An additional weakness was the lack of MRI imaging at follow-up to evaluate the integrity of the repair. This might confuse the results, as the improvement in some cases (18 patients) might be due to concurrent procedures performed.
A positive aspect of the study is that data from all treated patients were carefully collected, and preoperative, postoperative, and numerous validated shoulder scores were carefully used to assess the results. In addition, all patients were operated on by a single surgeon and were evaluated preoperatively and during follow-up by an independent doctor at an average follow-up of 2.7 years. Additionally, the multivariate analysis of data has shown that the associated surgical procedures performed in this series of patients do not have any influence on the clinical results.
In summary, the surgical technique of arthroscopic transtendon repair of PASTA-type cuff tears is a reliable procedure that can be expected to produce a good outcome with significant pain relief and improved shoulder scores in 98% of the patients. The data conclude that better results will be achieved in patients who have small tendon retraction, large footprint exposure, younger age, and a traumatic onset of shoulder symptoms.