
Abstract
Background: Femoral nerve blockade has been purported to be an effective regional anesthetic in patients undergoing various procedures to lower extremities.
Hypothesis: Femoral nerve blockade will provide improved postoperative pain control over a local anesthetic in the knee joint alone in patients undergoing endoscopic patellar tendon anterior cruciate ligament reconstruction.
Study Design: Randomized, controlled trial; Level of evidence, 1.
Methods: Fifty-six adult patients undergoing an endoscopic patellar tendon anterior cruciate ligament reconstruction under general anesthesia were prospectively randomized to receive either a bupivacaine femoral nerve blockade (block) or a saline placebo injection (control). Both groups received local bupivacaine injection and intravenous ketorolac at wound closure. Outcomes included postoperative pain measured on a validated visual analog scale at postoperative intervals for 72 hours, intraoperative and postoperative narcotic consumption, admission rates, hospital charges, patient satisfaction, and complications related to the femoral nerve block.
Results: There were 31 block patients and 25 control patients. No significant differences between groups for postoperative pain scores, intraoperative or postoperative narcotic consumption, readiness for discharge, duration of hospitalization, admission rates, hospital charges, or patient satisfaction were observed. There were no complications related to the femoral nerve block.
Conclusion: A preemptive femoral nerve blockade, although safe, does not provide significant clinical benefit in this patient population to justify its routine use.
Regional nerve blockade has emerged as an effective method of anesthesia for patients undergoing certain orthopaedic procedures to the upper and lower extremities. When a regional nerve block is administered before the surgical procedure, it is referred to as a preemptive anesthetic. It is theorized that preemptive anesthesia can decrease intraoperative as well as postoperative narcotic requirements by reducing the number of afferent pain signals transmitted by nociceptive fibers.7,14,35,61 Femoral nerve blockade (FNB) has been used primarily for operative procedures of the lower extremities. ‖ Reliable anesthesia over the anterior thigh, knee, and anteromedial leg is provided, while motor function to the lower extremity is preserved. Previous studies have shown that an FNB (with 27 and without ¶ local anesthetic injection) provides extended postoperative pain control when administered to patients undergoing knee ligament reconstruction20,21,38,51,55,56 knee arthroscopy,5,27 and total knee arthroplasty.2,31 It has yet to be shown conclusively if a preemptive FNB is clinically beneficial for patients undergoing patellar tendon anterior cruciate ligament (ACL) reconstruction. A double-blinded, randomized trial by Frost et al 25 comparing FNB and placebo injection in patients undergoing hamstring ACL reconstruction under general anesthesia showed no clinically significant benefit of the block over intra-articular bupivacaine alone. Studies supporting the use of FNB in this patient population have unfortunately suffered from significant design problems, including lack of randomization,21,38,59 an absence of control groups,21,38 inconsistent timing of the block, 21 and a deficiency of meaningful outcome measures.21,45,48,51,56
It is our hypothesis, based on clinical experience, that a preemptive FNB will lead to an objective improvement in pain control, reduce postoperative narcotic use and hospital admissions, and improve patient satisfaction in patients undergoing patellar tendon ACL reconstruction. Therefore, the purpose of this study is to evaluate FNB as a supplement to general anesthesia in patients undergoing isolated patellar tendon ACL reconstruction measuring a variety of clinical and nonclinical patient outcomes.
Materials and Methods
Study Design
This study, which was approved by our university's Investigational Review Board, was a double-blinded, randomized, placebo-controlled trial in patients undergoing an endoscopic patellar tendon ACL reconstruction. Consent to participate in the study was obtained by 1 of 3 fellowship-trained sports medicine surgeons during preoperative consultation in the office.
Patients were randomized to receive a preemptive bupivacaine FNB (block) or a subcutaneous saline placebo injection (control). In addition, all patients (block and control) received a general anesthetic as well as a local anesthetic injection intra-articularly into the knee joint as well as subcutaneously in and around each portal incision and graft harvest site at the end of surgery. Randomization occurred immediately before surgery when the anesthesiologist working in the preoperative holding area selected the next consecutively numbered sealed study envelope containing the preassigned study group (allocated using computer-generated random numbers). The anesthesiologist was not blinded to the group assignment and administered the FNB or saline placebo injection in the preoperative holding area immediately before surgery. This anesthesiologist was not involved with the patient's care in the operating room; however, the surgeons and patients were blinded to group assignment. All procedures were initiated before 2 o'clock to avoid the confounding variable of time of day on discharge decisions.
Study Population
The study population included patients 18 years of age and older undergoing endoscopic ACL reconstruction with a patellar tendon autograft under general anesthesia during a 16-month period. Patients were excluded from the study if they had had prior ipsilateral knee surgery or contralateral ACL reconstruction, had a drug allergy to bupivacaine, were unwilling to participate in the randomization process, had a history of narcotic abuse or a metabolic disease known to affect anesthetic or narcotic metabolism, for example, diabetes mellitus or chronic liver disease, or were undergoing a concurrent major operation, that is, other ligament reconstruction, on the involved extremity. The most common causes for exclusion were patients’ unwillingness to undergo the randomization process and fill out the evaluation forms necessitated by the study. As ACL tears and meniscal or chondral injuries are commonly associated, patients requiring concomitant meniscal surgery, that is, meniscectomy or repair, or minor chondral procedures, that is, chondroplasty, were included in the study.
Injection Technique
Both lower extremities of each patient were covered with thigh-high antiembolism stockings in the preoperative holding area. A barrier drape was placed above the patient's waist to obscure his or her observation of the injection. The groin region of the involved extremity was prepared with betadine and a sterile field established. Patients were told by the anesthesiologist that they would feel a needle stick or pressure in the groin. They were also instructed to report any “electrical” or “pins and needle” sensations in the thigh or leg indicating intraneural injection. Questions from the patients of a general nature were answered by the anesthesiologist, but no other information regarding the type of injection or anticipated sensation, for example, distribution of the femoral nerve, was given. A paravascular injection technique with nerve stimulation was used in the block group. Thirty milliliters of 0.5% bupivacaine with 1:200 000 epinephrine was injected with a 22-gauge needle inserted lateral to the femoral arterial pulse. A nerve stimulator connected to the injecting needle was used to elicit a strong contraction of the vastus medialis, vastus intermedius, and vastus lateralis at 0.3 mA in those patients receiving the block. Patients in the control group were administered a subcutaneous injection of 2 mL of normal saline at a similar location though nerve stimulation was not attempted to avoid the risk of nerve injury. Patients in both groups were asked to contract their quadriceps muscle after the injection, although no prompting was given by the anesthesiologist as to the significance of their ability or inability to do so. Identical dressings were applied over the injection site of both groups after the injection. The operating surgeons were not present in the preoperative holding area during the injection; therefore, the presence of certain pieces of equipment, that is, nerve stimulator, was not relevant to surgeon blinding.
Intraoperative Management
A certified nurse anesthetist or board-certified anesthesiologist blinded to the nature of the injection (block vs placebo) administered a standard intraoperative anesthetic regimen on all patients. Lidocaine (1 mg/kg), propofol (2 mg/kg), and fentanyl (2 g/kg) were used for induction. Unless contraindicated, a laryngeal mask airway (LMA) was inserted for airway management. An endotracheal tube was used in those cases that an LMA was contraindicated. In this situation, rocuronium (0.6 mg/kg) was added to the above medications. Anesthesia was maintained with nitrous oxide (50%) in oxygen with sevoflurane titrated to keep the blood pressure to within 20% of baseline. After the induction of anesthesia, only morphine sulfate was used for pain control. Meperidine was substituted for those patients allergic to morphine. Narcotic administration was based on the patients’ response to painful stimuli, for example, tachycardia or elevated blood pressure, during the procedure. The narcotic pain medication was then titrated to achieve a respiratory rate of 10 to 15 breaths per minute. Shivering was treated with warmers and hot blankets rather than with meperidine.
The ACL reconstruction was performed with a central-third bone-patellar tendon-bone autograft using a 1-incision (endoscopic) technique. A midline incision was used for graft harvest and placement of the tibial tunnel. Both metal and bioabsorbable interference screws were used for graft fixation. Repairable meniscal tears were fixed with either inside-out sutures or meniscal fixators at the discretion of the surgeon. Irreparable tears were treated with partial meniscectomy. A tourniquet was used by all 3 surgeons, but the duration of tourniquet use, for example, throughout the entire procedure or only during and after graft harvest, was at the discretion of the operating surgeon. Each patient was given ketorolac (60 mg) intravenously after the tibial interference screw had been inserted (beginning of wound closure). All patients also received a 20-mL injection of 0.5% bupivacaine equally distributed both intra-articularly (10 mL) and at the wound sites (portals and graft harvest; 10 mL) at the completion of wound closure. Neither intra-articular drains nor continuous passive motion (CPM) devices were used. A Cryo-Cuff (Aircast, Summit, New Jersey) and postoperative hinged knee brace were placed on the operated limb at the conclusion of the procedure.
Postoperative Management
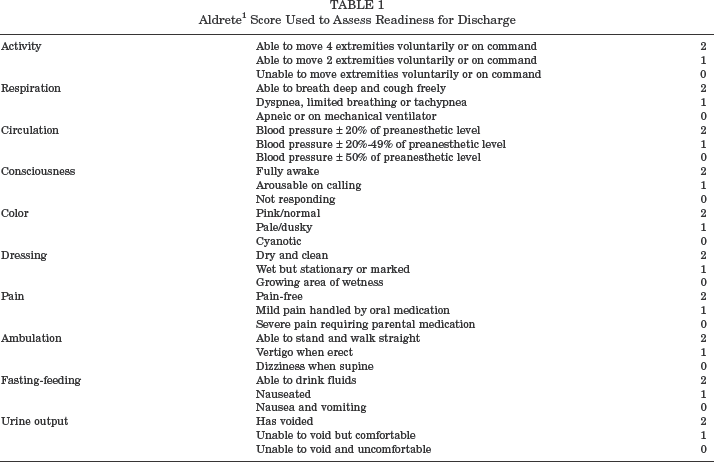
Nurses in the recovery room and same-day surgery unit assessed each patient's readiness for discharge every 30 minutes with the Aldrete score 1 (Table 1). Patients were discharged if they achieved a score of at least 18 and were able to urinate and ambulate with the assistance of crutches. Full weightbearing was allowed immediately upon discharge. If the patient did not meet the discharge criteria, then he or she was admitted as an inpatient. Special note was made of those patients admitted for non–pain-related conditions, for example, nausea or lack of transportation. All outpatients received 40 tablets of a hydrocodone/acetaminophen preparation (5 mg hydrocodone/650 mg acetaminophen) postoperatively with a prescribed dosage of 1 to 2 tablets every 4 to 6 hours as needed for pain. Oxycodone/acetaminophen (5 mg oxycodone/650 mg acetaminophen) was substituted for those patients allergic to hydrocodone. Propoxyphene/acetaminophen (100 mg propoxyphene/650 mg acetaminophen) was given to those patients intolerant of stronger narcotics. Those patients requiring stronger pain medication necessitating admission were prescribed a patient-controlled analgesia (PCA) pump to administer the same narcotic (morphine or meperidine) used during the procedure. The total amount of narcotic medication was recorded by the floor nurses. Use of nonnarcotic analgesics such as ibuprofen and acetaminophen was allowed if the patient's pain did not warrant narcotic medication.
Aldrete 1 Score Used to Assess Readiness for Discharge
Each patient was given a chart by his or her nurse at the time of discharge—either from the outpatient recovery unit or from the inpatient ward—to record the number of narcotic and nonnarcotic tablets consumed hourly for the first 72 hours postoperatively. Equipotent doses of all narcotic medications were calculated at the conclusion of the study.
Outcome Measures
Pain intensity was determined with a standardized 10-cm (0 = no pain, 10 = extreme pain) visual analog scale (VAS) preoperatively and at 2, 4, 8, 12, 24, and 72 hours postoperatively. The VAS has been previously validated as a reliable indicator of pain. 51 Pain intensity at the 4-hour time period was used as the primary outcome measure. Secondary outcome measures were the milligram amount of preoperative fentanyl (in micrograms), intraoperative narcotics used (in milligrams of morphine sulfate equivalents), the number of oral narcotic and nonnarcotic pain pills used postoperatively, duration of hospitalization, overall hospital charges, patient satisfaction, and complications related to the injection. Patient satisfaction was calculated as the mean response to 2 questions, each scored on a 5-point Likert scale. The questions were “Would you be willing to receive the same treatment again for pain in a similar surgery?” and “Would you recommend the treatment for a friend or family member having the same surgery?” (1 = definitely would not receive again/definitely would not recommend; 5 = definitely would receive again/definitely would recommend).
Statistical Analysis
Descriptive statistics included the means and standard deviations (SD) for continuous variables and percentages for categorical variables. We used the Wilcoxon rank sum test to compare continuous variables and the chi-square or Fisher exact test to compare proportions. Two-tailed tests (P < .05) were used throughout to determine statistical significance. Pain patterns between groups based on the VAS were compared using a polynomial regression analysis during the 72-hour time period. A post hoc power analysis using pain intensity on the VAS at the 4-hour postoperative period indicated an adequate sample size (based on preliminary pilot data only due to the lack of historical data) to maintain a significance level of 5% with at least 80% power to detect a 1–SD difference. Statistical analysis was performed with SAS software (SAS Institute, Cary, North Carolina).
Results
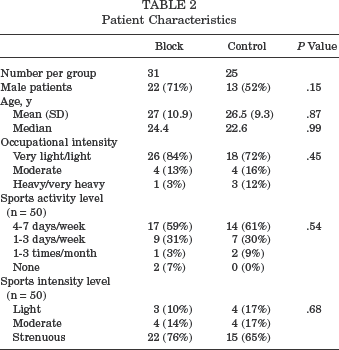
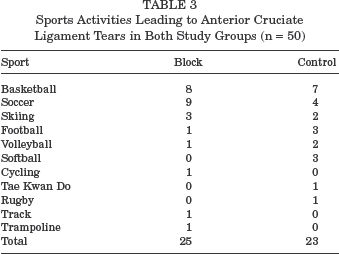
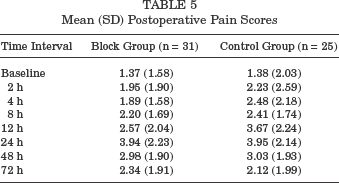
Of the 56 study patients, 31 were randomized to receive the femoral nerve blockade (block patients), and 25 were randomized to receive the placebo injection (control patients). Mean age of the patient population was 27 years. There were no significant differences between patients in the 2 groups at baseline (Table 2). All patients were classified as physical status I or II according the American Society of Anesthesiology classification and did not differ in age, occupational intensity, sports activity level, sports intensity level, or baseline pain scores (block group: 1.37 cm, SD, 1.58 cm; control group: 1.38 cm, SD, 2.02 cm; P = .98). The ACL tear occurred during sports activities in 26 (84%) of the block group and in 24 (96%) of the control group (P = .21). A breakdown of activities leading to the ACL tear is listed in Table 3. Mean duration of injury was 5.0 months (SD, 1.6) in the block group and 8.3 months (SD, 2.4) in the control group (P = .24).
Patient Characteristics
Sports Activities Leading to Anterior Cruciate Ligament Tears in Both Study Groups (n = 50)
There were no differences between groups in the number of concurrent procedures (Table 4). The mean duration of surgery was considered as the time between when the patient entered the operating room and when he or she entered the recovery room. This took into consideration patient positioning, preparing and draping, the actual operating time, the time to put on the dressing and brace, and the time to wake the patient and transport him or her to the recovery room. This averaged 257 minutes but differed among surgeons (surgeon A: 280, SD, 39 minutes; surgeon B: 250, SD, 28 minutes; surgeon C: 238, SD, 38 minutes; P = .0012). This difference was thought to be due to the increased number of meniscal repairs performed by surgeon A compared with surgeons B and C.
Concurrent Operative Procedures a
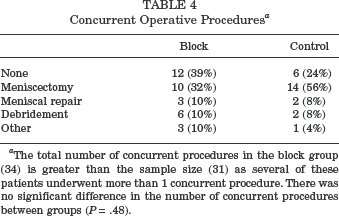
The total number of concurrent procedures in the block group (34) is greater than the sample size (31) as several of these patients underwent more than 1 concurrent procedure. There was no significant difference in the number of concurrent procedures between groups (P = .48).
Postoperative Pain
Mean postoperative pain scores for both groups are shown in Table 5. There was no difference in mean 4-hour pain scores (block group: 1.89, control group: 2.48; P = .5). The lowest pain scores were measured at 4 hours in the block group and at 2 hours in the control group; the highest scores were at 24 hours in both groups. Polynomial regression analysis of pain patterns between groups is shown in Figure 1. During the 72-hour postoperative period, there was no significant difference in postoperative pain scores between groups.
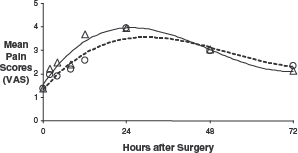
Polynomial regression of visual analog score (VAS) and time. Individual data points are plotted (Δ, control group; O, block group). Polynomial regression equations of the control group (solid line) and block group (dashed line) are shown. Control group: Y = 4E – 0.5× 3 - 0.0058× 2 + 0.2164× + 1.5516, R 2 = 0.9045 (P = .0165) Block group: Y = 2E – 0.5× 3 – 0.004× 2 + 0.1716× + 1.3375, R 2 = 0.8923 (P = .021)
Mean (SD) Postoperative Pain Scores
Postoperative pain medication usage is shown in Table 6. The mean number of pain pills used postoperatively (narcotic and nonnarcotic) was lowest on the day of surgery and highest on postoperative day 3 and did not differ between groups. The mean number of narcotic pain pills used from the day of surgery until postoperative day 3 in the block group and control group was hydrocodone/acetaminophen: 12.85, SD 10.9, and 15.08, SD 8.8 (P = .26); oxycodone/acetaminophen: 0.94, SD 2.7, and 1.0, SD 3.1 (P = .92); and propoxyphene/acetaminophen: 0.53, SD 2.0, and 0.0, SD 0 (P = .37), respectively.
Postoperative Analgesic Use a
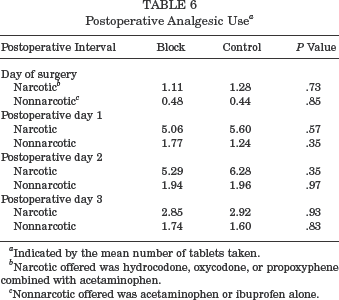
Indicated by the mean number of tablets taken.
Narcotic offered was hydrocodone, oxycodone, or propoxyphene combined with acetaminophen.
Nonnarcotic offered was acetaminophen or ibuprofen alone.
Secondary Outcomes
There was no significant difference in the amount of fentanyl given preoperatively between groups (block group: 143 μg; control group: 148 μg; P = .49). There was also no significant difference in the mean milligram amount of intraoperative morphine sulfate equivalents given between groups (block group: 9.84 ± 5.3 mg; control group: 10.88 ± 6.8 mg; P = .16).
The mean duration of hospitalization postoperatively was 13.2 hours (SD, 7.7) in the block group and 12.8 hours (SD, 8.3) in the control group (P = .9). There was also no significant difference between groups in the number of hours from the start of surgery until readiness for discharge by the Aldrete criteria (Table 7). There were 8 (26%) overnight admissions in the block group and 11 (44%) in the control group (P = .78). Nausea was the most common reason for admission of the block group, whereas pain was the most common reason for admission of the control group. Other reasons for admission were lack of transportation and the distance from the patient's home that he or she did not feel comfortable driving after surgery. Although patient satisfaction scores were higher in the block group (4.57, SD 0.75, vs 4.16, SD 0.99; P = .09), and hospital charges were lower ($9,991.60, SD $1,115.60, vs $9,452.87, SD $1,984.10; P = .23), these differences were not statistically significant (Table 7). None of the secondary outcome parameters differed as a function of the operating surgeon.
Secondary Outcome Measures
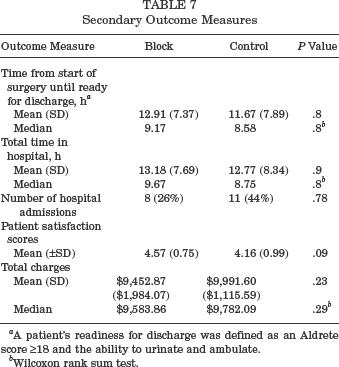
A patient's readiness for discharge was defined as an Aldrete score ≥18 and the ability to urinate and ambulate.
Wilcoxon rank sum test.
There were no neurological complications related to the block or placebo injection, nor were there any signs of systemic toxicity related to the injection of bupivacaine at any time point. Although several patients expressed temporary anxiety related to the injection, none complained of significant pain at the injection site.
Discussion
An important component of patient satisfaction after any surgical procedure is the method of pain management. The goal of this study was to rigorously assess the effectiveness of an FNB in patients undergoing endoscopic patellar tendon ACL reconstruction. The most important point to emerge from this study was that the addition of an FNB administered as a single preoperative injection provided no significant clinical benefit over postoperative injection of local anesthetic alone (and intravenous ketorolac) in this patient population. Specifically, we found no difference between patients who received an FNB in addition to local anesthetic and those without the FNB in pain during the 72-hour postoperative period, intraoperative or postoperative narcotic use, or patient satisfaction scores.
Arthroscopic ACL reconstruction has become accepted as an outpatient procedure due to the lower costs, low complication rates, and high patient satisfaction rates associated withoutpatient surgery in general.25,33,36,46,53 Pain after ACL surgery typically is most severe in the first 2 postoperative days,8,41 but effective postoperative pain management enables early knee motion and progressive reestablishment of normal joint function. An ideal anesthetic for outpatient ACL surgery should be technically simple to administer, have a rapid onset of action, be highly effective, have few or no side effects, and be relatively inexpensive.
There is conflicting evidence about the effectiveness of an FNB for pain reduction after knee surgery. Recent studies suggest that FNB is effective in reducing postoperative pain after knee arthroscopy,5,11,12,27 total knee arthroplasty,2,22,54,58 and ACL reconstruction # due to the innervation pattern of the knee joint. Previously published studies have documented a decrease in postoperative narcotic requirements and improved pain control when an isolated FNB is administered in addition to general anesthesia either before or after an ACL reconstruction or repair. ** However, the majority of these studies have been nonrandomized, retrospective analyses without a control group. Frost et al 25 assessed the efficacy of an intraoperative FNB (at the end of the procedure) compared with placebo injection in those patients undergoing a hamstring ACL reconstruction. These authors found no significant clinical difference between groups except a reduction in a single VAS pain score on the night of surgery. As a result, they concluded that an FNB was not beneficial in this patient cohort and did not recommend its routine use. Similarly, Mehdi et al 44 reported that a postoperative FNB offered no advantage over intra-articular local anesthetic combined with oral analgesia after patellar tendon ACL reconstruction. Our findings were in agreement with these prior studies.
Preemptive analgesia is an antinociceptive treatment that prevents the establishment of central sensitization, which amplifies postoperative pain.35,61 However, the degree of benefit of preemptive analgesia on pain after surgery has been debated.28,35,61 Tissue damage from surgery typically produces 2 phases of sensory input. The first is associated directly with the tissue-damaging stimulus, whereas the second results from the inflammatory reaction to the damaged tissue. It is controversial which stimulus is most relevant to the production of postoperative pain and, therefore, when a block is more effective—before or after surgery. 61 We failed to demonstrate a clinically beneficial effect of our method of preemptive analgesia. One possible reason is the difference between the duration of the preemptive analgesia and the duration of peripheral inflammation that stimulated the dorsal horn neurons with nociceptive input.7,35 Only continuous blockade of a peripheral nerve will prevent any sensitization of either the peripheral terminal or dorsal horn bodies to further inflammation or nociceptive input associated with the surgical trauma. While a single injection is the most frequently used method of administering an FNB to patients undergoing knee surgery, an intermittent 38 or continuous-infusion FNB, 55 or “3-in-1 block”10,11,22,39,40,60 (regional blockade of the femoral, lateral femoral cutaneous, and obturator nerves), may have reduced pain to a greater degree in our study population. However, in comparison with single-injection FNB, these other methods are technically more difficult and costly to perform, require extra equipment in the form of an indwelling catheter, which increases the risk for infection, 18 and are not as common as the method we chose to study.
Local side effects associated with an FNB include vascular puncture,38,40 intraneural injection, femoral nerve palsy,6,24,32,37,38 dermatitis at the site of injection,21,38 and the toxic systemic effects of the anesthetic agent. The incidence of neurological injury after peripheral nerve blocks ranges between 0.5 of 10 000 and 4.8 of 10 000, 3 but there have been sporadic reports of femoral nerve palsy after blockade after the injection of a “safe” dose based on body weight calculations.6,24,32,37,38 Patients in whom the inguinal landmarks are difficult to identify, for example, the morbidly obese or those having previous surgery in the inguinal region, or those patients with anatomical variants are most at risk for the inadvertent puncture of either the femoral artery, vein, or nerve. We attempted to minimize the risk of iatrogenic neurovascular injury by using a nerve stimulator and by ensuring that nerve stimulation ceased at a low level of current. 2 Fortunately, none of the patients in the block group exhibited any signs of temporary or permanent local or peripheral neurologic injury.
The systemic side effects of bupivacaine for local or regional anesthesia involve primarily the central nervous system (anxiety, dizziness, blurred vision, tremors, and seizures) and the cardiovascular system (cardiac depression and dysrhythemias). Rarely, these agents may lead to signs of local and systemic hypersensitivity. 21 More severe central nervous system and cardiovascular side effects are usually associated with higher plasma concentrations possibly related to accidental intravenous or arterial administration, unusually rapid uptake from the site of administration, decreased metabolic degradation, or excessive administration. 21 No patient in our study showed any sign or symptom of local or systemic toxicity from the bupivacaine injection.
Study Strengths
We sought to assess the efficacy of femoral nerve blockade in a randomized, double-blinded, placebo-controlled trial. Strengths of our methods include the randomized design and the use of a sham procedure to blind the patients, surgeons, and the treating anesthesiologist/anesthetist to the study group assignment. This was critical, as the primary outcome of this study was the participant's subjective assessment of pain. Control patients in this study received “usual care” for patients undergoing ACL reconstruction–intra-articular local anesthetic and an intravenous nonsteroidal anti-inflammatory drug (ketorolac), pain management that has been shown to improve pain relief after arthroscopic knee surgery and total knee arthroplasty.9,15,23,34,43,47,49 This increases the relevance of our findings to patients undergoing this procedure and may explain why we found no benefit to an FNB in contrast to other investigators who found an FNB to be beneficial over placebo for a similar procedure. To minimize the effect of procedural factors and practical considerations on duration of hospitalization, we used accepted, comprehensive discharge criteria to objectively assess each patient's readiness for discharge in addition to actual length of stay. The timing of postoperative discharge after any surgical procedure is affected by several patient and procedural factors, which are difficult to quantify separately. 21 Patient factors include their degree of pain and nausea, their ability to ambulate with crutches, and their mental acceptance of early discharge. 21 Postoperative pain, nausea, and vomiting can have a significant effect on the recovery process and on patient satisfaction with his or her care after outpatient surgery. 13 Interestingly, nausea was the most common reason for admission in the block group, whereas pain was the most common reason in the control group. Nevertheless, there was no significant difference in admission rates or pain satisfaction scores between groups despite these findings. Procedural factors such as the availability of an anesthesiologist to discharge the patient from the outpatient recovery room may have also influenced the duration of hospitalization.
Study Limitations
There are several limitations to our study. This was a single-site study, and our findings may not generalize to other settings. However, the FNBs were administered by 3 different board-certified anesthesiologists and the surgeries performed by 3 different surgeons. Therefore, our findings are likely not anesthesiologist- or surgeon-specific. The 3 anesthesiologists were experienced in administering these blocks; therefore, the possibility that the block group did not do significantly better solely because of ineffective blocks seems unlikely. All FNBs were performed with the patients awake in the preoperative holding area with the use of a nerve stimulator—both factors accepted as being the ideal standard by which to perform this type of regional block. A second potential limitation was our avoidance of nerve stimulation in the control group as a means to limit the risk of iatrogenic nerve injury. Because the control patients were blinded to the expected sensation of a muscle twitch associated with femoral nerve stimulation, and because they were physically prohibited from observing the method of injection, the absence of a deep injection with nerve stimulation (for ethical reasons) should not have been a source of bias. Third, we relied on self-reported data for outcome assessment. Although patients were blinded to their treatment group and all were trained to use the same standardized measurement protocol, patients’ responses and measurement intervals were not objectively confirmed or monitored. However, we do not believe that outcome measurements by patients differed systematically. Unfortunately, feasibility concerns precluded the accurate measurement of total costs, and we relied instead on hospital charges. We are unable to quantify the positive effect of the ketorolac injection on pain control as it was given as an adjunct to all patients. Finally, our sample was relatively small; thus our failure to demonstrate any benefit may be due to inadequate power. A lack of historical literature on which to base a power analysis a priori to assess secondary outcome measures such as narcotic and nonnarcotic use, reasons for hospital admission, patient satisfaction, and hospital charges limited us to a post hoc power analysis of the primary outcome measure—pain scores at the 4-hour postoperative intervals. A post hoc analysis of these secondary outcome measures indicated that nearly 1000 patients would be required in each group to show statistical differences with adequate power. The fact that we found no evidence of benefit in these multiple secondary outcomes suggests that any clinical benefit to an FNB over local anesthetic alone is minimal.
Conclusion
The results of this randomized, double-blinded, placebo-controlled trial have shown that a preemptive femoral nerve block, though safe, does not provide significant clinical improvement over local bupivacaine and intravenous ketorolac to justify its routine use in patients undergoing endoscopic patellar tendon ACL reconstruction.