
Abstract
Background:
There is little scientific evidence available regarding the pathologic basis for chronic groin injury in athletes, a known difficult clinical problem.
Hypothesis:
Histological analysis of the superior pubic ramus in athletes with diagnosed chronic groin injury may reveal the nature of the pathologic process.
Study Design:
Case series; Level of evidence, 4.
Methods:
Ten athletes with a diagnosis of chronic groin injury by clinical criteria (at least 6 weeks of pain) and magnetic resonance imaging criteria (unequivocal increase in T2 signal intensity) underwent bone biopsy of the superior pubic ramus. The biopsy site was located in the parasymphyseal region in the area of increased magnetic resonance image signal intensity. Histologic analysis of the specimens was then undertaken.
Results:
Evidence of new woven bone was seen in all biopsy specimens. Signs of old bony injury were seen in 8 of the 10 specimens. There was no evidence of inflammation or osteonecrosis.
Conclusion:
Histologic analysis of bone biopsy specimens taken from the parasymphyseal pubic bone region with magnetic resonance imaging T2-weighted increased signal intensity of athletes diagnosed by clinical and magnetic resonance imaging criteria as having chronic groin injury demonstrates new woven bone formation. This is consistent with the athlete having a bone stress injury that may contribute significantly to athletic groin pain.
Keywords
Sports-related chronic groin pain is a difficult clinical problem, with many different causes being proposed.7,10 Recent studies20,21 have implicated a pubic bone stress injury of the superior pubic ramus as a common diagnostic entity in elite-level Australian Rules football players. These studies associated the finding of MRI-detected increased signal intensity of the parasymphyseal bone region with the clinical features of groin injury.20,21 The conclusion drawn was that this increased signal intensity was consistent with pubic bone marrow edema, a nonspecific finding associated with bony stress injuries.2,4 Other authors have also demonstrated similar MRI findings in symptomatic athletes with chronic groin pain, but not all have come to the same conclusion with respect to diagnosing pubic bone stress injury.3,5,11,15,17
No published study exists, however, which correlates the finding of increased T2-weighted signal intensity of the pubic bone on MRI with histologic findings, and therefore it is not clear that bone marrow edema is responsible for the finding seen commonly on MRI. Furthermore, there are few studies that describe the histologic appearance of the common MRI finding of increased T2-weighted signal intensity with any disease or disorder. The notable exceptions to this are found in histologic studies of bony tumors, bone marrow edema syndrome of the hip, 13 and bone bruises of the knee region. 14
Accordingly, the aim of this study was to biopsy the parasymphyseal region of the superior pubic ramus of athletes with clinical symptoms and signs of chronic groin injury in the area where an unequivocal increase in signal intensity on pubic bone MRI scans was detected. It was considered that subsequent histologic analysis may give an indication as to the nature of the pathologic process.
Methods
A study was performed on athletes, all of whom were male Australian Rules football players with a diagnosis of athletic chronic groin injury using clinical and MRI criteria. Clinical criteria included the presence of at least 6 weeks of groin pain, located in the adductor and/or pubic bone region and present during and/or after sporting activity. Clinical signs included pubic symphysis and superior pubic ramus tenderness, as well as positive pubic symphysis stress test results. 21 Additionally, the athlete needed to be significantly impaired by the injury, causing him to cease playing and/or training. Magnetic resonance imaging criteria were used to substantiate the diagnosis of chronic groin injury. These criteria included an unequivocal asymmetrical increase in MRI signal intensity of the parasymphyseal region of the superior pubic ramus on the predominant painful side of the injury. Thus our diagnostic criteria were consistent with the athlete having a pubic bone stress injury.19,21
With respect to the MRI, all athletes underwent T1-weighted spin-echo and fat-saturation T2-weighted fast or turbo spin-echo sequences in planes axial and coronal to the body of the pubis. T1-weighted spin-echo images were acquired with the following parameters: repetition time, 440 to 688 milliseconds; echo time, 20 milliseconds; slice thickness, 4 mm; gap, 10%; field of view, 20 cm; matrix size, 256 × 512; and acquisitions, 1 to 2. Fat-saturation T2-weighted images used the following parameters: repetition time, 4000 to 6002 milliseconds; echo time, 66 to 112 milliseconds; slice thickness, 4 mm; gap, 10%; field of view, 20 cm; matrix size, 224 to 240 × 256; and acquisitions, 2 to 3. T2-weighted fat-suppression images were subjectively graded for the intensity of bone marrow signal (normal = 0, subtle/equivocal = 1, moderate = 2, and severe = 3) by an experienced musculoskeletal radiologist (J.P.S.). We considered the bone marrow signal unequivocal when its change in intensity was graded 2 or 3.
After diagnosis, the athletes subsequently had 3 months’ rest, during which they were not permitted to undertake athletic weightbearing activity. The athletes then attempted a return to activity. Those athletes who failed to return to activity due to recurrence of pain were considered for enrollment in the study. A repeat MRI scan (same protocol as before) of the pubic bone region was then performed to confirm continuing asymmetrical increase in bone signal intensity. A signed informed consent form was then obtained before undertaking the procedure. The procedure consisted of a bone drilling to the pubic bone in the parasymphyseal region as a day-surgical procedure. Bone biopsies (core samples) (Figure 1) were taken from the predominantly painful side of the superior pubic ramus area with unequivocal MRI signal intensity increase. Athletes who had equal pain on both sides had bone biopsies on both affected sides. The bone was drilled from the superior aspect of the superior pubic ramus to the inferior aspect of the superior pubic ramus using radiographic guidance. The core sample was then removed. This procedure was repeated so that each participant had 2 samples taken from the same predominantly affected side. Subsequently, we closely monitored athletes for short- and long-term complications to establish whether the procedure could be undertaken safely in this pubic bone location.
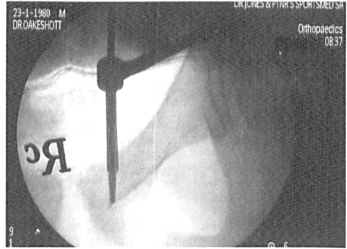
Core biopsy of bone. Entrance was from the superior part of the parasymphyseal region of the superior pubic ramus, with the drill extending to the inferior part of the superior pubic ramus.
The specimens were analyzed from the superior aspect of the superior pubic ramus to the distal extent of the biopsy specimen (inferior part of the superior pubic ramus). Bone biopsy specimens underwent histologic analysis by 2 independent clinical pathologists (L.H. and N.L.F.). The specimens were fixed in 10% neutral buffered formalin, decalcified, and stained with hematoxylin and eosin (H&E); trichrome stains were used if necessary to highlight connective tissue, and Perl's stain was performed to help identify granules of hemosiderin pigment. The sections were studied with ordinary brightfield microscopy and also with crossed polars to help identify and distinguish between woven bone and lamellar bone. Institutional ethical approval was obtained to analyze and report the findings from the collected biopsy specimens. The rationale for this procedure to be performed in this pilot study was to perform a core decompression of the pubic bone in a manner similar to that used for osteonecrosis of the femoral head. We were attempting to increase blood flow to the region and thereby hasten bone recovery. Thus the procedure was performed for considered therapeutic reasons and conformed to the declaration of Helsinki.
After the procedure, athletes were rested from weightbearing athletic activity for a further 6 weeks and a gradual reintroduction of activity was instituted.
The bone biopsy specimens were examined for the presence of the following features: (1) new woven bone (micro-callus), (2) edema, (3) inflammatory cells, (4) osteonecrosis, and (5) evidence of chronic bone injury, such as hemosiderin, chondroid callus, and/or desmoid-like areas.
Follow-up was performed by the surgeon (R.D.O.) at 2 and 6 weeks after the procedure. Rehabilitation and return to activity was supervised by the sports physician (G.M.V.) over the subsequent 9 months, principally by direct consultation. Parameters assessed at follow-up included (1) complications of procedure (eg, pain, swelling, genitourinary symptoms), (2) ongoing symptoms and/or resolution of symptoms, (3) ability to return to sport, (4) timing of return to sport, (5) assessment at end of subsequent playing season for number of games played and presence or absence of ongoing symptoms.
Results
Ten athletes provided informed consent and underwent pubic bone drilling for a biopsy specimen of bone. Two athletes had both sides drilled, whereas the remaining 8 had a single side drilled. All athletes fulfilled the clinical and MRI criteria for chronic groin injury outlined in the Methods section. Tables 1 and 2 detail symptom duration, biopsy, and MRI results.
Biopsy Results From the 10 Participants a
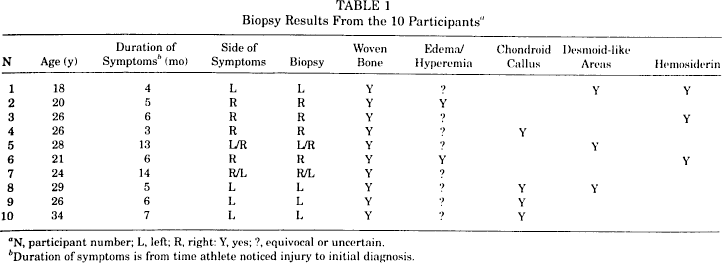
N, participant number; L, left; R, right: Y, yes; ?, equivocal or uncertain.
Duration of symptoms is from time athlete noticed injury to initial diagnosis.
MRI Results From the 10 Participants a
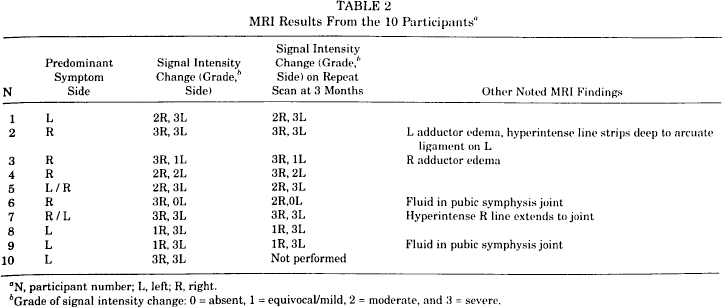
N, participant number; L, left; R, right.
Grade of signal intensity change: 0 = absent, 1 = equivocal/mild, 2 = moderate, and 3 = severe.
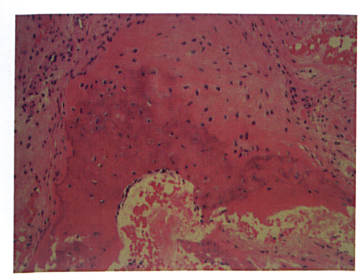
The bone biopsy specimens of all 10 participants demonstrated new woven bone. The new woven bone did not appear to represent simple bone remodeling of existing bony trabeculae such as normally follows homeostatic osteoclastic activity. In these cases, the process of new woven bone was considered to represent a repair process. It was also considered that the new woven bone from specimens was nonlocalized and was present throughout the entire specimen from the superior aspect of the superior pubic ramus to the inferior aspect of the superior pubic ramus. Stellate fibroblasts, neovascularization, and plump osteoblasts were seen in the woven bone specimens (Figures 2 through 7).
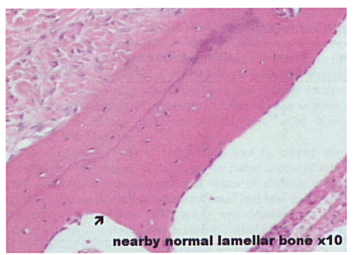
Normal bone seen on H&E section. Magnification ×10.
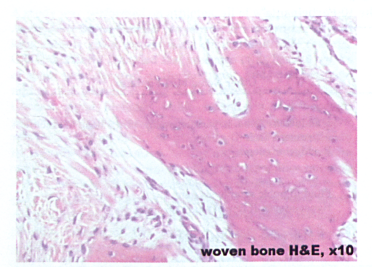
Woven bone seen on H&E section. Magnification ×10.
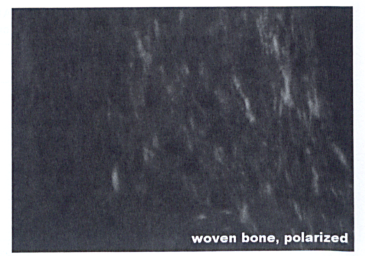
Woven bone seen on polarized light demonstrating a disorganized pattern. Magnification ×10.
Neovascularization on H&E section. Magnification ×10.
Stellate fibroblasts on H&E section. Magnification ×20.
Plump osteoblasts consistent with woven bone formation on H&E section. Magnification ×20.
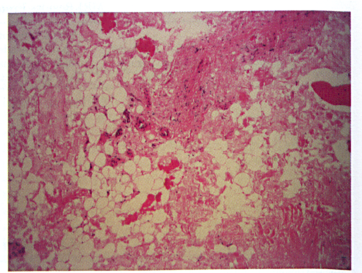
Edema/hyperemia was only considered to be unequivocally present in 2 specimens. There was no evidence of inflammatory cells or osteonecrosis on any of the biopsy specimens. Chronic bony injury was represented by the presence of chondroid callus, desmoid-like areas, and/or hemosiderin deposition and was present in 8 of the 10 biopsy specimens (Figures 8 and 9).
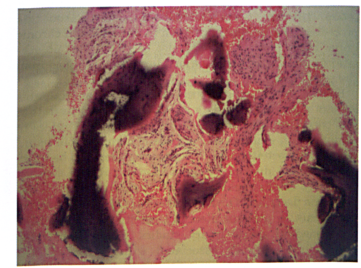
Desmoid-like fibroblasts and chondroid callus. Magnification ×10.
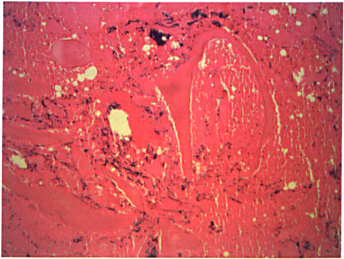
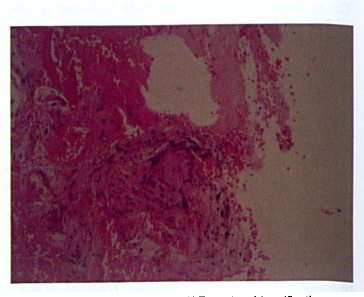
Chronic bone changes. Hemosiderin deposition identified with Perl's stain. Magnification ×10.
At follow-up, we found that 8 athletes played in the subsequent football playing season whereas 2 did not play due to continuing groin problems. Of those who played, 5 were symptom-free at the beginning of the subsequent playing season (approximately 12 weeks after the procedure), whereas 3 had continuing symptoms. Of those who played by the end of the subsequent playing season (9 months after the procedure), 6 athletes were symptom-free whereas 2 had continuing groin symptoms. No complications, surgical or otherwise, were noted in any athletes.
Discussion
The major finding of our study was the observation that increased T2-weighted signal intensity demonstrated on MRI is associated with new woven bone and with plump osteoblasts, neovascularization, and stellate fibroblasts. Thus our findings are consistent with the athlete having a bony stress response as the pathologic cause, at least in part, of activity-related chronic groin pain.
Edema was seen conclusively in 2 specimens. It must be stated that edema is demonstrated on the MRI scans and cannot be reliably determined from histologic sections. As an explanation of this, bone marrow edema is considered to be interstitial and therefore difficult to detect when considering the nature of these specimens.
Importantly, there was no evidence of osteonecrosis, infection, or inflammation. It is also not surprising that in many cases, there were histologic findings consistent with old bony injury, as all participants had at least 6 months of symptoms before acquisition of the biopsy specimen. New bony remodeling with any bone injury can continue for many months, even after clinical recovery has ensued, and hence the finding of new woven bone coexisting with old bony changes is consistent with the proposed pathologic process.
Limited information exists in the published literature with respect to the histologic findings of increased T2-weighted signal intensity on MRI. A finding similar to our study has been seen in specimens taken from core decompression from studies of the bone marrow edema syndrome of the hip with the demonstration of new bone formation. 13 However, to our knowledge, no previous study has taken bone biopsy specimens in athletes with chronic groin pain, who are considered to have a different etiologic process for their condition, and in this respect our study can be considered unique.
Woven bone has been demonstrated to form in an animal model as a response to fatigue loading. By exposing the ulna bone of laboratory rats to a single bout of in vivo fatigue, authors were able to demonstrate woven bone formation 16 and increased periosteal vascularity 12 as a response to this stimulus. Furthermore, the woven bone formation was demonstrated to occur as a dose-dependent response to the damaging mechanical loading of the bone 18 and is considered to be formed to restore the whole-bone strength and to enhance resistance to further damage that can be caused by continuing repetitive loading. 13 These studies give us some basis for the hypothesis that woven bone formation can occur as a consequence of repetitive loading as seen in our athletes. However the actual inciting events for the parasymphyseal pubic bone woven bone formation and increased T2-weighted signal intensity on MRI in this study are not as clear. Potential explanations include primary bone stress (repetitive loading) injury, insertional adductor enthesopathy, and pubic symphysis joint disruption. This study does not conclusively demonstrate any single cause as responsible for the entity of pubic bone stress injury as it is possible that new woven bone formation, along with signs of old bony injury, may be seen in all of these proposed causes. To our knowledge, no study of the histologic findings of enthesopathies has been presented and therefore we cannot compare our findings to any other study.
On the basis of the evidence presented in this study, we consider a primary bone stress injury as being the most likely entity to be responsible for the described clinical and histologic findings as opposed to other possible explanations. We have deduced this from the following observations: (1) the nature of how the biopsy specimens were taken, with the biopsy bone entrance being from the superior part of the superior pubic ramus that was not associated with any particular muscle-tendon insertion, in particular the adductor tendon region (Figure 1); (2) the extensiveness of the MRI signal intensity changes being seen throughout the anterior-posterior and superior-inferior extent of the superior pubic ramus and not localized to any particular area of muscle/tendon attachment (Figure 10); and (3) the widespread nonlocalized new woven bone (it was present in most cases in the entire biopsy core) seen in the biopsy specimens.

Coronal T2 MRI scan demonstrating extensive parasymphyseal pubic bone marrow edema.
Pelvic biomechanical studies lend support to this view of the superior pubic ramus being prone to stress injury. It is considered that, with weightbearing, the superior pubic rami and the pubic symphysis act as a compression strut, linking the femur to the posterior pelvic structures and spine, 1 with the centers of rotation (screw axes) being near the pubic symphysis. 9 Thus the parasymphyseal bony area is the region of the anterior pelvis considered most vulnerable to the stressors of athletic activity.
The original rationale for this procedure to be performed in this pilot study was to perform a core decompression of the pubic bone in a manner similar to that used for osteonecrosis of the femoral head. 8 We were attempting to increase blood flow to the region and thereby hasten bone recovery. It was apparent from the limited number of biopsy specimens that there was no evidence of osteonecrosis as the underlying pathologic process. When comparing the clinical results from this study to a study in which pubic bone stress injury was diagnosed and treated nonoperatively, 21 it is apparent that the clinical results obtained from this group of athletes treated with a pubic bone core decompression were similar to the nonoperatively treated group. Therefore, it is difficult to be enthusiastic about this procedure as a therapeutic option in athletes with chronic groin injury. However, it may also be stated that no athletes demonstrated short- or long-term complications from the procedure.
Finally, we believe that the nosology of osteitis pubis should be discussed. It is a relatively common term that has been used in sports medicine and generally refers to athletes with a nonspecific episode of chronic groin pain. 6 Historically, osteitis pubis has been considered to be infective in origin due to a complication of urologic surgery. Similarly, osteitis pubis as an obstetric complication has also been described. Obviously these are unlikely causes of groin pain in athletes. Recently, osteitis pubis has been mentioned in sports injury studies that demonstrated chronic groin injury associated with increased MRI parasymphyseal signal intensity.11,20 If possible, it would be better if specific diagnoses could be used to describe sports-related chronic groin injury rather than osteitis pubis, which has differing meanings in medicine.
Conclusion
Histologic analysis of bone biopsy specimens taken from the parasymphyseal pubic bone region of athletes diagnosed by clinical and MRI criteria as having chronic groin injury demonstrates new woven bone formation. This is consistent with the athlete having a bone stress injury as the probable cause of the athletic groin pain. This is the major finding from our study. Additionally, the common MRI finding of increased signal intensity in the context of athletic overuse is most probably due to the formation of new woven bone formation with associated plump osteoblasts, neovascularization, and stellate fibroblasts. There was no evidence of osteonecrosis or inflammation detected in this study.