
Abstract
Background: New devices for graft fixation in anterior cruciate ligament reconstruction are released to clinical use without clinical follow-up data.
Hypothesis: There is similar clinical outcome after either cross-pin or absorbable interference screw fixation in anterior cruciate ligament reconstruction with hamstring tendons.
Study Design: Randomized controlled clinical trial; Level of evidence, 1.
Methods: A total of 120 patients were randomized into 4 different groups (30 each) for anterior cruciate ligament reconstruction with hamstring tendons: femoral Rigidfix cross-pin and Intrafix tibial expansion sheath with a tapered expansion screw; Rigidfix femoral and BioScrew interference screw tibial fixation, BioScrew femoral and Intrafix tibial fixation; or BioScrew fixation into both tunnels. The evaluation methods were clinical examination, knee scores, and instrumented laxity measurements.
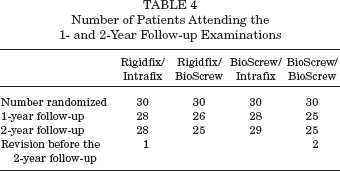
Results: Ten patients were completely lost to follow-up and 3 revisions were done before the 2-year follow-up, leaving 107 of 120 (89%) patients for analysis. No statistically significant differences between the groups were seen 2 years postoperatively, and all but 2 patients in the Rigidfix/Intrafix and Rigidfix/BioScrew groups, respectively, were classified into International Knee Documentation Committee A or B categories. A revision reconstruction was performed before the 2-year follow-up in 2 cases after a high-energy injury caused a rerupture (1 in Rigidfix/Intrafix and 1 in BioScrew/BioScrew groups). In addition, there were 4 nontraumatic failures revised before the 2-year follow-up (2 in Rigidfix/Intrafix and 1 each in Rigidfix/BioScrew and BioScrew/BioScrew).
Conclusion: There were no statistically or clinically relevant differences in the results 2 years postoperatively, and all 4 techniques improved patient performance.
Keywords
Bone-patellar tendon-bone graft (BPTB, central third) and hamstring tendons have been used as free autografts to replace a torn anterior cruciate ligament (ACL) with increasing use of hamstring tendon grafts13,17 because of less postoperative morbidity, anterior knee pain and trauma, and versatility of the fixation methods.7,36 It has been shown that a 4-stranded hamstring tendon graft is stronger graft material than BPTB graft, 19 but the weakest points in hamstring tendon ACL reconstruction are not the graft itself but the fixation sites, and, particularly during the early postoperative period, the stability of the fixation of a hamstring graft to the bone tunnel is considered to be the primary factor in limiting rehabilitation.9,21 Therefore the graft fixation to bone should be strong enough to avoid failure, stiff enough to restore load-displacement response, and secure enough to resist slippage under cyclic loading. 16 It should allow early rehabilitation and hold the graft in place until histological transition to calcified fibrocartilage has occurred at the bone-tendon interface. 13
There are numerous ways to fix the graft into the bone tunnels, of which an interference fixation with a screw made of metal or of bioabsorbable material has been mostly used.15,28,30 Follow-up studies of hamstring tendon reconstruction have documented tunnel enlargement. In a prospective study comparing metal and bioabsorbable screw fixation, there were significantly larger radiographically visible drill holes on both the tibial and femoral sides in the Poly-L-Lactide (PLLA) group compared with the metal group at 6 and 24 months, but clinical examination at 2 years revealed no major differences between the groups. 28
Although prospective studies have shown that interference screw fixation in BPTB and hamstring tendon graft fixation give statistically equal results in terms of laxity and knee scores,15,30 alternative soft tissue graft fixation techniques have been sought. The graft can be suspended outside the femoral tunnel by a metal plate, “EndoButton,” 5 or transfixed with cross-pins,12,34,41 and some clinical experience of these techniques has been presented. †
References 2–4, 12, 18, 20, 29, 32, 35, 40.
Less innovation has been made regarding tibial fixation, and variations of the interference principle have prevailed. The interference screw can be introduced either eccentrically 8 or concentrically between the graft limbs. Transfixation by cross-pins can be used here also. 3 A novel approach has been the Intrafix (DePuy Mitek, Raynham, Massachusetts) device in which a sheath made of plastic or absorbable material is expanded with a screw. Biomechanical studies have been done with contradicting results.6,10,13,25
The ACL graft fixation devices can be made of metal, plastic, or, increasingly, of bioabsorbable material. The advantage of biomaterials is that there is no need to remove the fixation devices, and revision surgery might be easier if the implants have been absorbed. The most optimal fixation method has not yet been defined, the solutions are new, and the follow-up of clinical materials has been short. Therefore, scientifically valid, randomized, controlled, prospective (RCT) studies are needed.
The purpose of this study was to prospectively compare hamstring tendon ACL reconstruction when the fixation method was randomized into 4 groups using Rigidfix cross-pin (DePuy Mitek) in the femur and Intrafix expansion sheath and a tapered expansion screw in the tibia compared to conventional interference screw fixation technique (BioScrew; Linvatec, Largo, Florida) and to report the results 1 and 2 years after surgery.
We hypothesize that all 4 techniques provide equal results in restoring knee stability.
Materials and Methods
To fix the graft and as the basis for the randomization, we chose the following 3 devices. For femoral fixation we used 2 Rigidfix bioabsorbable rods (PLLA). The diameter of the rod is 3.3 mm and the length is 42 mm. Tibial fixation was done with a nonabsorbable Intrafix device, which consists of an expansion sheath made from high-density polyethylene and a tapered expansion screw molded from Delrin (DePuy Mitek). Finally, for femoral and/or tibial fixation BioScrew, a bioabsorbable interference screw made of L-lactic acid, was used.
In group I, femoral Rigidfix cross-pins and a tibial expansion sheath and a tapered expansion screw (Intrafix, n = 30) were used. In group II, femoral Rigidfix and tibial interference screw fixation (BioScrew, n = 30) were used. In group III, femoral BioScrew and tibial Intrafix fixation (n = 30) were employed. And in group IV, BioScrew fixation into both tunnels (n = 30) was done.
The diagnosis of an ACL tear was made by clinical examination, by magnetic resonance imaging (MRI) examination when needed, and confirmed at arthroscopy. According to the study protocol, the inclusion criteria were fresh or chronic (less than 5 years old) unilateral ACL tears in female or male patients with an age range of 18 to 50 years. Additional injuries could be an uncomplicated meniscal lesion and minor chondral damage.
To exclude a case the interval between the injury and surgery needed to exceed 5 years or be a revision procedure. Concomitant grade II to III collateral or posterior cruciate ligament tears and peripherally detached meniscal tears to be repaired as well as severe Outerbridge 3 to 4 chondral damage and arthrosis of the knee also excluded the case.
Randomization was done by sealed, numbered envelopes that contained information of the treatment group, and the patients as well as physiotherapists were blinded to the method used. Numbers were generated by a computer program using block randomization to ensure equal distribution of patients into each group. The envelope containing information of the treatment allocation was not opened until arthroscopy had confirmed the diagnosis after graft harvesting was completed. Two surgeons (both authors) performed the reconstructions. The ethical committee of the University Hospital District approved the study, and the patients gave their informed consent to participate.
Surgical Technique
After diagnostic arthroscopy and minor menisci procedures were completed, the hamstring tendons (STG) were harvested through a short vertical incision located medial to the tibial tuberosity. The Linvatec graft harvester was used. The grafts with a diameter from 7 mm to 10 mm were individually prepared for the specific fixation method determined by the randomization group.
The drill tunnels were aimed into the posterior fourth quadrant of the femoral condyle in the sagittal plane and into 10:30-o'clock position in the right and 1:30-o'clock position in the left knee in the frontal plane. In the tibia, sagittally, the second quadrant anterior to posterior was targeted with the drill guide intra-articularly positioned at the ACL footprint.
The graft in Rigidfix fixation was constructed according to the manufacturer's instructions with whipstitches of No. 1 Vicryl (Ethicon Inc, Johnson & Johnson, Somerville, New Jersey) to join the doubled limbs of the semitendinosus and gracilis tendons together. Drill guides were used, and the depth of the transtibially drilled femoral tunnel was 30 mm to 40 mm. With the Rigidfix instrumentation, 2 transverse drill tunnels were drilled to receive the fixation devices. After the graft was passed into the drill tunnel by pulling it with No. 2 Vicryl loop left in the graft end, 2 Rigidfix implants were tapped through the drill guide sleeves transfixing the graft and advanced to the bone medial to the drill tunnel.
For the Intrafix tibial fixation, No. 1 absorbable whipstitch in the graft ends was used, and the graft was spread into 4 quadrants between the sleeve and the drill tunnel. After cycling of the knee 10 to 15 times, the graft was tightened, and the expansion sleeve and the screw were introduced concentrically by which the 4 limbs of the graft could be compressed between the bone tunnel and the device. Three sizes of the screw were used: if the graft size was less than or equal to 8 mm, the 6 mm to 8 mm screw was used (7–9 mm screw if the bone quality was suboptimal), and if the graft was larger than 8 mm, the 8 mm to 10 mm screw was used. In the BioScrew fixation, the femoral drill tunnel was done with the “outside-in” technique using the rear-entry guide (Linvatec). A tight whipstitch with No. 1 Vicryl was used to join the graft limbs together to form a single bundle. The bioabsorbable interference screw of 30 mm length and diameter equal to the graft and tunnel was inserted eccentrically, compressing the graft against the bone tunnel wall. The fixation was reinforced with a resorbable button in 25 cases by which the whipstitch sutures were secured outside the femoral and/or tibial tunnel. If the graft ends protruded from the tibial tunnel entrance, the screw fixation was supplemented with a staple (Richards; Smith & Nephew, Memphis, Tennessee). Before the tibial fixation, the knee was cycled 10 to 15 times through the range of motion in all 4 groups. The graft was then tightened to 40-N force with the Mitek tensioning device (Intrafix fixation), and in the BioScrew fixation a manual estimate of 40 N was done. The knee was held in 30° of flexion, and the distal ends of the graft were secured according to the group specified.
Rehabilitation
Postoperatively no knee braces were used, and the knees were immediately mobilized in the same way in all groups. During the 2 postoperative weeks partial weightbearing with crutches was recommended and thereafter full weightbearing was allowed as tolerated. Active quadriceps activity was delayed until 3 to 4 weeks postoperatively. The physiotherapist used closed kinetic chain muscle rehabilitation principles in guiding the patients. Return to sports activity was allowed gradually 6 to 12 months postoperatively and after 1 year without restrictions.
Preoperative and Postoperative Evaluation
Tegner activity level was used to define the actual physical performance (0–10) and for subjective evaluation Lysholm knee scores (0–100) were recorded preoperatively 38 as well as “patellofemoral scores” (KPS 0–100, Table 1). 27 Information for the IKDC was gathered (2000 IKDC KNEE EXAMINATION) and the subjective IKDC score was calculated. 23
Median Tegner Activity Level, Lysholm, IKDC, and Patellofemoral Scores (KPS) Preinjury (I) and Preoperatively (II) in ACL Reconstruction in the 4 Randomization Groups a
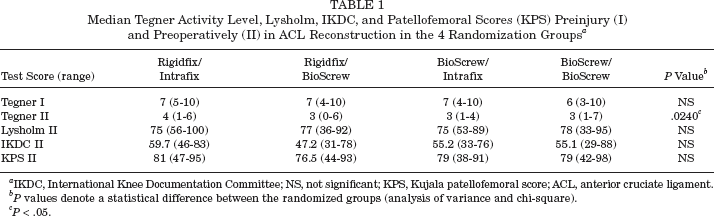
IKDC, International Knee Documentation Committee; NS, not significant; KPS, Kujala patellofemoral score; ACL, anterior cruciate ligament.
P values denote a statistical difference between the randomized groups (analysis of variance and chi-square).
P < .05.
On clinical examination the Lachman test was graded negative (– with hard end point; side-to-side difference <3 mm), slightly positive (+; side-to-side difference 3–5 mm), or clearly positive (++; side-to-side difference >5 mm). Correspondingly, in the pivot-shift test the grading was negative (–), glide (+), or clearly positive (++).
In addition to clinical examination, anteroposterior knee laxity (side-to-side difference with 35-pound and manual maximum force; KT-2000 arthrometer, MEDmetric Corporation, San Diego, California) and isokinetic peak muscle torques of the knee extensors and flexors at 60 deg/s and 180 deg/s (Lido MultiJoint II, West Sacramento, California) were measured. These examinations were repeated at 1 and 2 years postoperatively. The clinical examinations were done by both authors, the KT-2000 arthrometer and isokinetic measurements were done by a physiotherapist, and the knee scores were completed by the patients themselves.
Statistical Analysis
Statistical analysis was performed using the BMDP statistical package (Statistical Solutions Ltd, Cork, Ireland). The parametric data between the 4 groups were evaluated with analysis of variance. The nonparametric data were evaluated with chi-square (between the groups) and with McNemar's or sign test (comparison over time within a group). The minimum level of significance was P =.05. One of our main outcome measurements was the Lysholm score. With a difference of 10 points, a clinically significant difference between the treatment groups would be acknowledged. When type I error (α) was set at 0.05 and power (β error, power 1-β) at 80%, sufficient total sample size would be 54 for 2 treatment groups. Therefore, 120 cases were allocated equally into 4 treatment groups.
Results
A total of 120 patients with a fresh or chronic ACL injury were operated on with hamstring tendon reconstruction. With regard to the fixation method, they were randomized into 4 treatment groups as described above. The first patient was randomized in August 2001 and the last in August 2004. Baseline characteristics (gender, age, additional injuries, and time from injury to operation) were similar in all groups preoperatively, although there was a higher preoperative Tegner activity level in the Rigidfix/Intrafix group and among the BioScrew/Intrafix and BioScrew/BioScrew groups (Tables 1 and 2). The isokinetic flexion torque percentage at 180 deg/s was better than in the remaining 2 other groups (Appendix available online at http://ajs.sagepub.com/supplemental/). Otherwise there were no differences between the study groups preoperatively regarding the Lysholm or KPS scores or IKDC classification (Tables 1 and 3).
Demographic Variables in ACL Reconstruction in 4 Randomization Groups a
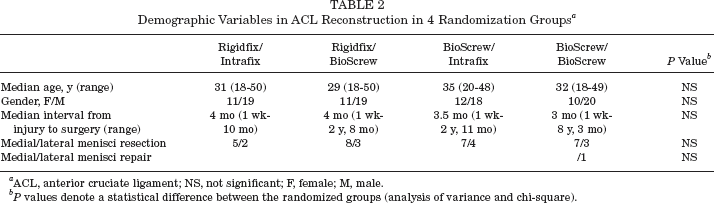
ACL, anterior cruciate ligament; NS, not significant; F, female; M, male.
P values denote a statistical difference between the randomized groups (analysis of variance and chi-square).
IKDC Classification Without Subjective Evaluation Preoperatively and 1 and 2 Years Postoperatively in ACL Reconstruction With the 4 Randomization Groups a
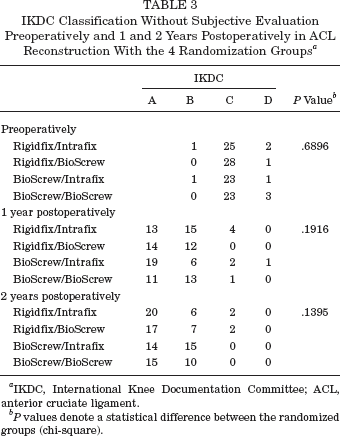
IKDC, International Knee Documentation Committee; ACL, anterior cruciate ligament.
P values denote a statistical difference between the randomized groups (chi-square).
There were altogether 4 violations to the study protocol. One randomization was misread to group III when it should have been group II. Therefore analysis of the results was done according to the intention to treat principle 22 keeping the patient in the intended treatment group. The data were also analyzed according to the actual fixation method. Against the study protocol in one case, a contralateral ACL injury was also noted 6 months after surgery (group III). Side-to-side laxity difference measurements were omitted concerning this case. In one case a detached lateral meniscus was repaired (group IV). Finally, a patient belonging to group IV had injured her knee 8 years previously.
Ten patients were completely lost to follow-up, and 3 had undergone a revision ACL surgery before the 2-year follow-up, leaving 107 of 120 (89%) patients for analysis (Table 4). The reason for revision was a new injury disrupting the graft in 2 cases (1 in Rigidfix/Intrafix group and 1 in BioScrew/BioScrew group) and 1 for a graft failure (BioScrew/BioScrew). At the 2-year follow-up, 3 obvious failures were noted by ++ pivot-shift or Lachman tests (2 in the Rigidfix/Intrafix and 1 in the Rigidfix/BioScrew groups).
Number of Patients Attending the 1- and 2-Year Follow-up Examinations
Range of Motion
There was no difference between the groups with respect to range of motion (ROM) at the 1- or 2-year follow-ups. One year postoperatively there were altogether 8 patients (Table 5) with 1° to 5° of extension deficit. The ROM was from 147° to 152° in the 4 groups (Table 5). By the 2-year follow-up the ROM had improved, without statistical significance, with a range from 151° to 154° in the 4 groups (Table 5). Two years postoperatively there were altogether 6 patients with an extension deficit of 1° to 5°.
Range of Motion (ROM) 1 and 2 Years Postoperatively in ACL Reconstruction With the 4 Randomization Groups
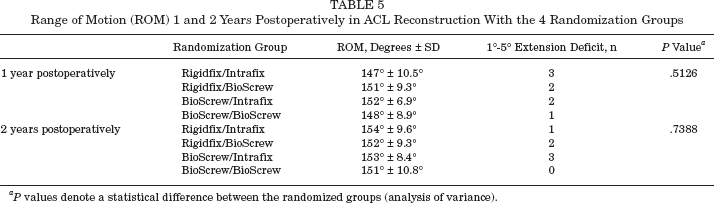
P values denote a statistical difference between the randomized groups (analysis of variance).
Stability
There were no statistically significant differences between the groups with respect to clinical stability evaluation either preoperatively or at the 1- or 2-year follow-up examination (Table 6). There was an almost statistically significant difference (P = .0506) between the groups at 2 years because 2 of the 3 failures occurred in the Rigidfix/Intrafix group. The mean preoperative manual maximum KT-2000 arthrometer side-to-side laxity difference diminished from 4.4 mm to 1.4 mm by 2-year follow-up in the Rigidfix/Intrafix group. The corresponding values in the Rigidfix/BioScrew group were from 4.7 mm to 2.2 mm, in the BioScrew/Intrafix group from 5.3 mm to 2.7 mm, and in the BioScrew/BioScrew group from 4.9 mm to 2.2 mm. No statistically significant differences between the groups were found preoperatively or in the 1- and 2-year laxity measurements (Table 7).
Clinical Stability Evaluation 1 and 2 Years Postoperatively in ACL Reconstruction in the 4 Randomization Groups
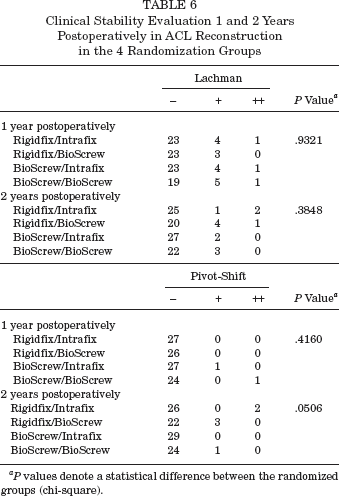
P values denote a statistical difference between the randomized groups (chi-square).
Anterior-Posterior Laxity Side-to-Side Difference (in mm) Measured With the KT-2000 Arthrometer Device Using 35 Pounds and Manual Maximum Forces (Injured–Control Knee, Mean ± SD) Preoperatively as Well as 1 and 2 Years Postoperatively in ACL Reconstruction With the 4 Randomization Groups a
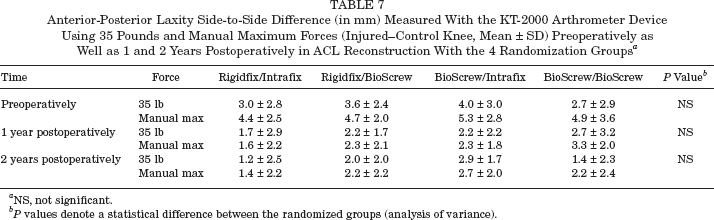
NS, not significant.
P values denote a statistical difference between the randomized groups (analysis of variance).
Knee Scores
There were no differences between the groups in the 1- or 2-year follow-up examinations with respect to Tegner activity level, Lysholm knee score, IKDC score, or the Kujala patellofemoral score (KPS) (Table 8).
Tegner Activity Level, Lysholm, and KPS Scores 1 and 2 Years Postoperatively in ACL Reconstruction With the 4 Randomization Groups a
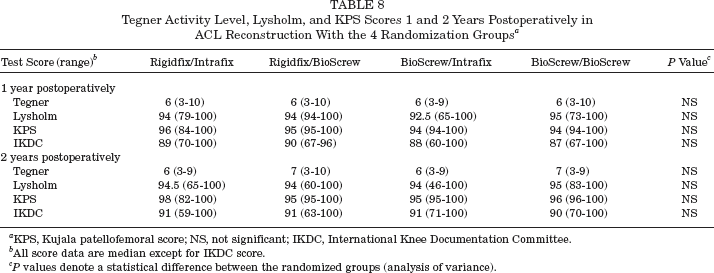
KPS, Kujala patellofemoral score; NS, not significant; IKDC, International Knee Documentation Committee.
All score data are median except for IKDC score.
P values denote a statistical difference between the randomized groups (analysis of variance).
IKDC Classification
There were no differences between the groups in the preoperative IKDC classification. For the most acute cases (<2 months) the preoperative IKDC classification was not done (Table 3). There were no differences between the groups at the 1- or 2-year follow-up (Table 3). At the 2-year follow-up all but 2 cases in the Rigidfix/Intrafix and Rigidfix/BioScrew groups were classified to IKDC A or B categories (Table 3).
Isokinetic Peak Muscle Torque
There was a statistically significant difference between the groups regarding the isokinetic peak muscle torque preoperatively (percentage control–injured extremity). In the BioScrew/Intrafix and in the BioScrew/BioScrew a higher 180 deg/s flexion torque was observed (P = .0316). This tendency remained throughout the follow-up in both 60 deg/s and 180 deg/s flexion torque measurements (see online Appendix at http://ajs.sagepub.com/supplemental/).
Complications and Additional Procedures
There was one perioperative technical complication when posterior blowout of the femoral graft tunnel occurred in a Rigidfix/Intrafix case and the graft was secured with staple fixation. A broken screw guide wire was noted in the postoperative radiograph, and it was removed arthroscopically the next day (BioScrew/Intrafix group). In one case (BioScrew/BioScrew group) a hematoma in the harvest site was evacuated the first postoperative day. These complications did not affect the outcome. Two infections were noted, of which one was a deep infection requiring washout arthroscopies and antibiotic treatment with eventual healing and a stable knee (BioScrew/BioScrew group). The other one was an infection at the tibial entry site in a patient belonging to the BioScrew/Intrafix group. After operative debridement and eventual healing, the knee became slightly unstable with 1+ Lachman, negative pivot-shift, and 6 mm side-to-side difference in KT-2000 arthrometer manual maximum laxity tests. In one case, a deep-vein thrombosis was diagnosed with uneventful recovery after thrombolytic treatment (BioScrew/Intrafix group).
In addition to the 3 revision ACL reconstructions, there was surgery in 7 cases during the 2-year follow-up period. One Intrafix device was removed (extrusion) and in another case a broken BioScrew tip was removed from the knee joint. Two medial meniscus resections were performed after new injury. Two arthroscopies showed a femoral condyle lesion (treated with microfracture) in one and a partial peripheral medial meniscal detachment in the other. In one case knee arthroscopy was done twice, a Cyclops lesion was found in both procedures, and in addition a bucket-handle medial meniscus tear the second time as well. No injury had been present at the time of ACL surgery. The total number of additional procedures was 11 in 10 cases with no correlation to the randomization groups. The cases with complications and additional procedures were grouped together and analyzed against the rest of the material. No significant difference was noted in the clinical stability examination at 2 years. The 2-year KT-2000 arthrometer mean manual maximum laxity side-to-side difference was 2.4 mm in the additional procedure group and 1.8 mm in the rest (P = .4359). The corresponding median values for Tegner activity level were 7 in both groups (P = .7916); 92.5 and 94, respectively, for median Lysholm score (P = .0925); 92 and 90.8, respectively, for median IKDC score (P = .9281); and 97 and 96, respectively, for KPS (P = .0622).
Discussion
There are numerous biomechanical studies in which graft fixation techniques are compared with one or several different methods. ‡ In an intra-articular model with ovine soft tissue grafts after 6 weeks, the biomechanical characteristics of grafts that were fixed with cross-pins were superior to those of grafts after interference screw fixation. 42 In a human ex vivo knee biomechanical study, transcondylar screw fixation of the patellar tendon autograft into the femoral tunnel performed mechanically as well as interference screw fixation. 11 In porcine femora, the interference screw and the Rigidfix fixation demonstrated inferior fixation biomechanics compared with Bio-Transfix (Arthrex, Naples, Florida) and EndoButton techniques. 1 Biomechanical test results of hamstring grafts in bovine knees with a suspension screw were found to be better than those of the interference screw. 39 Among 9 different types of femoral fixation in porcine knees, the transcondylar devices offered the best structural properties for femoral fixation of doubled hamstring graft in ACL reconstruction. 31 Dargel et al 14 showed the importance of graft preparation in the Rigidfix technique. If no stitching of the looped-over portion of the quadrupled graft was done, the ultimate failure loads were lower compared to the grafts that were prepared properly with whipstitching.
References 1,8, 10, 11, 13,24,25,31,42.
Caborn et al 10 compared bioabsorbable interference screw and Intrafix fixation in human tibiae and quadrupled hamstring tendon grafts. They found that displacement at failure was greater for the Intrafix device. Krupp and colleagues' 26 biomechanical study compared the fixation of quadrupled semitendinosus and gracilis (STG) allografts in standard drilled tunnels prepared in low apparent bone mineral density (BMD) cadaveric tibiae using either an Intrafix device with primary intra-tunnel fixation in a region of predominantly cancellous trabecular bone, or a CentraLoc (Arthrotek, Warsaw, Indiana) device with primary extra tunnel fixation in a region of predominantly cortical bone. The CentraLoc group displayed superior load at failure and survived more loading cycles than the Intrafix group. Coleridge and Amis, 13 using calf tibiae and 4-strand tendon grafts fixed with the Intrafix and 4 different devices, reported there was no significant difference in graft construct elongation under cyclic loads, and all devices performed well under cyclic loads that represented normal walking activity but the ultimate strengths differed. Kousa et al 25 compared 6 different tibial graft fixations finding that the Intrafix provided clearly superior strength in the fixation of hamstring tendon grafts to the tibial drill hole. In a bovine model, CentraLoc and bioabsorbable interference screws provided superior resistance to cyclic loading compared with the Intrafix device. 6
According to biomechanical test results, the new fixation methods (Rigidfix and Intrafix) have not differed from other fixation methods and their performance has met the requirements of the loads supposed to occur in daily activities.24,25,33 Clinical follow-up results after cross-pin femoral fixation (TransFix) have been presented, and the short-term results were good. 12 TransFix cross-pin femoral fixation has been compared with interference screw fixation in a randomized setting, and no significant differences have been found.20,35 Rose et al 35 disproved their hypothesis that the transfixation technique leads to less laxity and therefore to a better clinical outcome when compared with the use of bioresorbable interference screws. They found no significant differences in the knee laxity testing using the Rolimeter (Aircast, Vista, California) device between both groups and over time within these groups. Ninety percent of all patients had functionally normal or near normal IKDC knee ligament ratings almost equally distributed in both groups within the IKDC subgroups. Musil et al 32 compared BPTB graft with the hamstring tendon Rigidfix fixation and reported no differences in the results. A randomized study comparing the Rigidfix with resorbable screw fixation in hamstring tendon ACL reconstruction has been reported but so far no detailed report has appeared. 37
In the present study new fixation techniques, absorbable cross-pins and an expansion sheath and screw, were compared with standard absorbable interference screw fixation. Not only did the authors want to explore whether these 2 proximal and distal fixation methods might have a different outcome, they also wanted to determine if such outcomes were related to either proximal or distal fixation. That is why the randomization was done into 4 groups mixing the femoral Rigidfix and tibial Intrafix fixations with interference screw fixation. According to the results no statistically significant differences between the 4 fixation methods were observed. There was an almost significant difference (P = .0506) between the groups 2 years postoperatively because there emerged 2 cases with ++ pivot-shift in the Rigidfix/Intrafix group and 3 cases with + pivot-shift in the Rigidfix/BioScrew group. These were obvious failures or graft elongations resulting from either loosening in the point of fixation or graft necrosis. This might imply that the Rigidfix fixation is not as good as interference screw fixation on the femoral side. On the other hand, there was no difference between the groups with respect to the various knee scores (Lysholm, Tegner, KPS, IKDC), and a significant improvement in function was achieved by the reconstruction.
There are some limitations in our study. Four study groups are difficult to handle, as can be noted in violations to the study protocol. Statistical analysis became difficult to interpret, and there was little room for missing cases from the follow-up. The addition of back-up fixations in some of the interference screw fixation cases might have skewed the results and certainly were an addition to the existing 4 study groups.
Conclusion
There was no statistically or clinically relevant difference in the results 1 or 2 years postoperatively, and all 4 techniques improved patient function. It is important to evaluate the performance of the new fixation methods in prospective randomized studies comparing them with standard methods. According to the results of this study, it can be said that the Rigidfix and Intrafix fixation methods compare well with interference screw fixation in ACL reconstruction with hamstring tendons.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.