
Abstract
Background: Physical examination maneuvers for patellar instability are often inaccurate.
Hypothesis: The “moving patellar apprehension test” is a sensitive and specific physical examination technique for the diagnosis of patellar instability.
Study Design: Cohort study (diagnosis); Level of evidence, 3.
Methods: The moving patellar apprehension test was performed in an office setting preoperatively and compared with the ability to dislocate the patella when examined under anesthesia in 51 patients. The examination begins with the knee held in full extension and the patella is manually translated laterally with the thumb. The knee is then flexed to 90° and then brought back to full extension while the lateral force on the patella is maintained. For the second half of the test, the knee is started in full extension, brought to 90° of flexion, and then back to full extension while the index finger is used to translate the patella medially. For a positive test in part 1, the patient orally expresses apprehension and may activate his or her quadriceps in response to apprehension. In part 2, the patient experiences no apprehension and allows free flexion and extension of the knee.
Results: When compared with the ability to dislocate the patella under anesthesia, the moving patellar apprehension test was found to have a sensitivity of 100%, a specificity of 88.4%, a positive predictive value of 89.2%, a negative predictive value of 100%, and an accuracy of 94.1%.
Conclusion: The moving patellar apprehension test is an accurate physical examination technique that, when performed and interpreted correctly, is highly sensitive and specific for patellar instability.
This incidence of patellar dislocation is 29 per 100 000 in adolescent age groups, 15 and recurrence rates with nonoperative treatment have been reported from 15% to 44%.7,15,21,25 Furthermore, an even larger 55% will not be able to return to sports with nonoperative treatment. 4 The mechanism of patellar instability is attributed to several anatomical factors, including abnormal osseous anatomy of the trochlea and patella,9,41 overall abnormal mechanical alignment of the lower extremity, 29 and deficient static and dynamic medial soft tissue stabilizers. §
References 5, 8, 11, 17, 19, 20, 22, 30, 44.
A history of instability is usually associated with a traumatic weightbearing or twisting event followed by the onset of acute pain. Often, patients do not report a frank dislocation or subluxation event, even when specifically questioned if they sensed their patella move out of position. For patients with recurrent instability, examination features that are most consistent with patellar instability are tenderness over the medial facet of the patella, tenderness over the medial patellofemoral ligament (MPFL) attachment onto the medial femoral epicondyle, and the patellar apprehension sign. Detection of patellar apprehension is not consistent, however. Sallay et al 40 found that only 39% (9 of 23) of patients who sustained a patellar dislocation had a positive apprehension sign. Garth et al17,18 also described difficulty in detecting MPFL deficiency in patients with patellar instability and attributed it to secondary restraints blocking the detection of injury to the primary restraint of the MPFL.
Accurate physical examination to detect patellar instability is especially important because radiologic studies may be insensitive in the nonacute setting. Radiographs and computed tomographic (CT) scans are static evaluations that do not visualize a frankly dislocated patella except in the rare occasion where the patella is unreduced. 19 Magnetic resonance imaging (MRI) has been advocated as a method of detecting features of patellar instability such as MPFL disruption in the acutely injured knee1,40 in which signal changes associated with bleeding, edema, and frank disruption can be observed. Tanner et al 42 found that MRI detection of chronic laxity of the MPFL, in the absence of bleeding or edema, has been disappointing, however.
To help achieve greater diagnostic accuracy for patellar instability, a new physical examination test has been developed that functionally mimics an actual dislocation or instability episode and therefore has potential for more diagnostic capacity and accuracy. The moving patellar apprehension test (MPAT) flexes and extends the knee joint with stress applied to the patella, which is similar to accurate examination maneuvers used in other joints to detect symptomatic instability.16,27,36,37
This study examines the use of MPAT and discusses the principles supporting its development. The hypothesis is that the MPAT will be sensitive, specific, and accurate in diagnosing patellar instability.
Materials and Methods
Approval of the Institutional Review Board from our institution was obtained. The senior author began using the MPAT as a routine patellofemoral examination maneuver in January 2003. To study the MPAT, patients who had both a possible diagnosis of patellar instability and a knee examination under anesthesia were selected. Charts during the period of January 2003 to January 2007 underwent an initial screening selecting those patients who underwent knee surgery. Those charts that passed the initial screening were then screened for the possibility of patellar instability, which was based on a documented preoperative history reporting symptoms of knee instability or giving way, anterior knee pain, or effusions. Therefore, patients were considered for inclusion in the study if they had undergone surgery that allowed an examination under anesthesia and then selected for inclusion if they had preoperative documentation that suggested a possibility of patellar instability. Retrospective chart review was performed, and the status of the MPAT performed preoperatively and the examination under anesthesia was recorded.
All patient histories obtained by the senior orthopaedic surgeon were documented in the chart and included the presence or absence of anterior knee pain, episodes of instability, and descriptions of knee swelling. All patients had documentation of a positive or a negative MPAT. As part of the surgical procedure, all patients received a complete examination under anesthesia, including an attempt to manually dislocate the patella laterally. The intraoperative ability to manually dislocate the patella was used as the gold standard against which the results of the MPAT were compared. Knee MRI reports were also reviewed for the presence or absence of the MPFL and/or medial retinacular injury.
Moving Patellar Apprehension Test
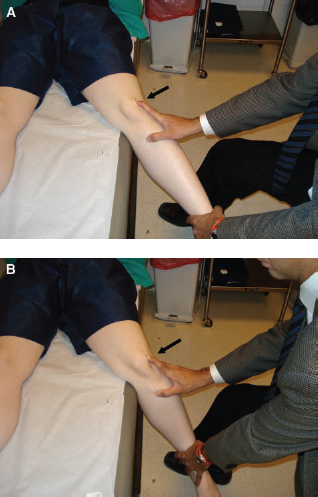
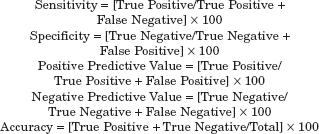
The MPAT is a modification of the patellar apprehension test.26,39 It is performed with the patient lying supine and relaxed with the ankle held off the examination table. The examination begins with the knee held in full extension while the patella is translated laterally with the examiner's thumb as far as possible (Figure 1). The knee is then flexed to 90° and brought back to full extension while the lateral force on the patella is maintained. During the second part of the test, the knee is started in full extension, brought to 90° of flexion, and then back to full extension while the index finger of the examiner is used to translate the patella medially as far as possible (Figure 2). To be considered a positive test in part 1, the patient orally expresses apprehension and may activate his or her quadriceps in an attempt to stop flexion and/or dynamically reposition the patella. In part 2 of a positive examination, the patient experiences no apprehension and allows free flexion and extension of the knee. For the MPAT to be considered positive, both parts 1 and 2 must be positive.

The moving patellar apprehension test examination technique. A, The knee is positioned in full extension, and the patella is translated laterally with the examiner's thumb. B, The knee is then moved into flexion and apprehension or quadriceps contraction is noted (arrow indicates direction of force applied to the patella).
A, The knee is positioned in full extension, and the index finger is used to translate the patella medially. B, The knee is then moved into flexion, and elimination of apprehension and quadriceps contraction is noted (arrow indicates direction of force applied to the patella).
Intraoperative Examination under Anesthesia
All patients with a preoperative diagnosis of patellar instability underwent a trial of nonoperative treatment with activity modification and formal physical therapy. Patients who continued to have symptoms despite nonoperative treatment were indicated for surgery. After general or regional anesthesia was established, the senior surgeon attempted lateral dislocation of the patella similar to part one of the MPAT. The knee was held in extension and the thumb applied lateral translation to the patella. The knee was then flexed and the patella was observed for frank dislocation. If the patella dislocated, the knee was then extended to allow reduction.
Statistical Procedures
All data were analyzed using SPSS 14.0 software (SPSS Inc, Chicago, Illinois). The descriptive statistics were calculated as follows:
Results
A total of 51 patients met the inclusion criteria and there were 27 (52.9%) female and 24 (47.1%) male patients with a mean age of 24.2 ± 10.3 years. The left knee was treated in 31 (60.8%) patients and the right knee in 20 (39.2%) patients. On the basis of intraoperative examination under anesthesia and operative findings, the treating surgeon classified 25 (49.0%) patients as having lateral patellar instability, 11 (21.6%) were diagnosed with osteochondral injuries and/or intra-articular loose body and/or plica, 7 (13.7%) with meniscal tears, 5 (9.8%) with patellar chondromalacia, 2 (3.9%) with combined ACL and meniscal injuries, and 1 (2%) patient with an ACL tear and an osteochondral injury.
Of the 51 patients included in the study, 49 patients had MRIs before surgery. Of the 49 with MRIs, 31 of them reported having a subluxation or a traumatic episode within the 3 months before the MRI, and these patients were considered to have an MRI during the acute postinjury period. Eighteen had the episode(s) earlier than 3 months before the preoperative assessment and were considered to have an MRI during the chronic period.
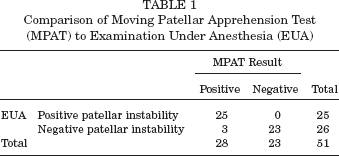
The MPAT performed during the clinic office visit was positive in all 25 (100%) patients operated on who had a frank patellar dislocation when examined under anesthesia. Three patients who did not demonstrate instability under anesthesia had a positive preoperative MPAT (false positives). Twenty-three patients had a negative MPAT, and all of these patients had inability to dislocate their patella under anesthesia (true negatives). There were no false-negative results. They all underwent knee surgery with management of knee injuries other than patellar instability. When compared with the physical examination under anesthesia, the MPAT was found to have a sensitivity of 100% (25 of 25) and a specificity of 88.4% (of 26 patients with stable patella, 23 had negative MPAT) (Table 1). The positive predictive value for the MPAT was 89.2%, with 25 of 28 positive MPATs actually having patellar instability. The negative predictive value for the test was 100%; all negative MPATs were in patients who did not have patellar instability. The accuracy of the MPAT was 94.1%.
Comparison of Moving Patellar Apprehension Test (MPAT) to Examination Under Anesthesia (EUA)
The results of the MRI were also compared with the ability to dislocate the patella. Two patients did not have preoperative MRI scans because of patient refusal. For the other 25 patients with ability to dislocate their patella under anesthesia, MRI reports were as follows: 10 patients had injury to the medial retinaculum and or medial patellofemoral ligament. These patients were all in a time period within 3 months of their last episode of instability. The other 13 patients with MRIs and ability to dislocate under anesthesia had no report of injury to the medial retinaculum or medial patellofemoral ligament. These patients all had their MRI after a 3-month time period from an episode of instability.
Discussion
Good outcomes have been reported after appropriate treatment for patellar instability, which varies from nonoperative rehabilitation, 28 trochleaplasty,10,43 osteotomies, and soft tissue and or MPFL reconstructions,12,14,34,35 but the first step for a good result lies in an accurate and prompt preoperative diagnosis. 38 Patellar instability has not proven easy to diagnose in many studies. Plain radiographs and CT scans have poor sensitivity for chronic patellar instability, although they are useful for surgical planning as well as evaluation of concomitant injuries.25,30 Accuracy of the MRI has been reported to be higher during acute episodes of patellar instability,19,33,40,42 but for some authors it still remains disappointing for chronic instability, which is consistent with our results.6,25,30,42,45 Because of these imaging limitations, physical examination is crucial for the diagnosis and treatment decision in these patients.22,23,38
The patellar apprehension sign was first described in 1936 as a clinical test producing a sense of apprehension in the patient on direct lateral displacement of the patella. 13 The exact examination maneuver was further detailed in 1968 as a test for patellar instability and described as “with the quadriceps relaxed, the knee in 30° of static flexion, a direct lateral force is placed on the patella. When positive, the patient expresses apprehension and begins to resist the lateral force by straightening the knee and relocating the patella.” 22 A recent investigation of the patellar apprehension sign showed a poor sensitivity of only 39% in patients with a history of dislocation while 87% had an MPFL tear at surgery. 40 Tanner et al 42 reported a further modification of the patellar apprehension sign and recommended testing the flexed knee at 30° and directing an oblique lateral force in line with the fibers of the vastus medialis obliquus while the quadriceps remained relaxed. They proposed that this better isolated the primary soft tissue restraints to lateral patellar instability and improved the accuracy of the test. 42 While these tests are performed at 30° of knee flexion, it is accepted that lateral patellar instability is most pronounced within the range of 0° to 30° of knee flexion. 2 Bruce Reider 39 in 1999 described a version of the patellar apprehension test equivalent to the first part of the MPAT, which moves the knee into flexion with lateral force applied to the patella. A positive test manifests with verbal anxiety or involuntary quadriceps contraction.
The MPAT was created based on the proposed mechanism of lateral patellar instability. In full knee extension, the patella is in its most unstable position and soft tissues and alignment are most responsible for the patella's stability. 2 As flexion begins, the patella must engage the trochlea and then stability is shared by the soft tissues, overall alignment, and the bone geometry of the trochlea and patella. For a knee without patellar instability, as the knee flexes the patella is guided into the trochlea by the MPFL and other medial soft tissue stabilizers. 2 The patella subluxates most easily at 20° of knee flexion, and the MPFL seems to resist lateral patellar subluxation greatest when the knee is toward full extension. 3 For patients with symptomatic instability, while the knee is flexing combined with an eccentric quadriceps force, the patella engages the trochlea in a lateral position and then dislocates or subluxates as the knee continues to flex.
For the patient with patellar instability who is being evaluated with the MPAT, as the knee flexes during the first part of the test, the patella engages the trochlea in a lateral position and mimics a patellar dislocation episode, therefore reproducing the symptoms associated with a dislocation. The MPAT also actively assesses the MPFL since the MPFL is responsible for guiding the patella properly into the trochlea as the knee moves from full extension into flexion. 2 In the second part of the test, with medial force on the patella as the knee is flexed, the symptoms of impending dislocation are eliminated because the patella engages the trochlea in a normal fashion. The manual translation of the patella reproduces the function of the deficient and/or incompetent MPFL. The MPAT is a combination of apprehension in part 1 and the reduction of the apprehension in part 2. This dynamic, provocative test is similar in concept to the pivot-shift test for ACL insufficiency in the knee, 16 the release test for anterior shoulder instability, 37 and the moving valgus stress test for valgus instability of the elbow. 36
In this study, 25 patients had apprehension during part 1 and all 25 showed reduction in apprehension during part 2. Although this would seem to indicate that part 2 of the examination may be unnecessary, we believe that the second part of the examination offers further confirmation of a positive result and may help resolve what may be “equivocal” examination maneuvers in part 1. The present study has demonstrated for the MPAT 100% sensitivity, 88.4% specificity, and overall accuracy of 94.1%, which are superior to previous reports using the patellar apprehension sign.31,40,46 The traditional patellar apprehension test requires forcing the patella laterally while the knee is positioned at 30° of flexion. This requires the patella to translate over the lateral trochlea rather than engage the trochlea in a lateral position and may be responsible for the poorer sensitivity and specificity of this test.
Several limitations of this study must be considered. First, we used intraoperative patellar dislocation as the gold standard by which to analyze the MPAT. Therefore, we cannot analyze patients with patellar instability who did not undergo surgery, such as those who responded to physical therapy and nonoperative treatment. The strict inclusion criteria were designed to include patients with possibility of patellar instability in whom the MPAT was performed and who also had an intraoperative examination under anesthesia (EUA) for comparison. The criteria allowed evaluation of the MPAT for diagnoses other than patellar instability. This facilitated proper calculation of sensitivity, specificity, negative and positive predictive values, and accuracy. In addition, patients with patellar subluxations (no frank dislocations) were excluded. This was implemented since a frank dislocation under anesthesia was chosen as a gold standard for diagnosing patellar instability to analyze the MPAT. Patients with symptomatic patellar instability but without frank dislocation under anesthesia do not have the gold standard to compare the MPAT and therefore were excluded. Thus, statements on the ability for the MPAT to diagnose injury in patients with patellar subluxation cannot be made based on this study. An alternative to using patellar dislocation when examined under anesthesia as a gold standard for analysis is to use MRI and then include those patients who did not have surgery; however, the accuracy of MRI is not high enough. This study also employed a single examiner at a single time point, so intra- and interobserver reliability is not assessed. Another source of potential bias is that the preoperative result of the MPAT was used to assist the diagnosis of patellar instability and influenced the decision to recommend surgery. Therefore, the possibility of false-negative results of the MPAT may have existed, and those patients, by not having surgery, are not captured in the data. This, however, is a problem recognized in many studies that evaluate examination maneuvers.24,32,36 Lastly, the study does not directly compare the standard patellar apprehension test to the MPAT. To have both tests performed on individual patients would have resulted in a sequence-order bias. If the MPAT is performed first and the patient is subject to a patellar apprehension episode, their sensation is heightened and a subsequent test of simple patellar apprehension may be positive when it otherwise would have been negative if the MPAT had not been performed.
Conclusion
The moving patellar apprehension test is a highly sensitive, specific, and an overall accurate physical examination test that can be performed in an office setting to diagnose patellar instability.