
Abstract
Background: This study was undertaken to prospectively analyze, at a mean 11-year follow-up, the clinical and radiographic outcomes in patients undergoing the authors’ intra-articular anterior cruciate ligament reconstructive procedure with extraarticular augmentation, and to compare these data with those at 5-year follow-up.
Purpose: The clinical and radiographic outcomes in patients undergoing anterior cruciate ligament reconstruction were analyzed at a mean 11-year follow-up.
Study Design: Case series; Level of evidence, 4.
Methods: The authors studied 54 of 60 consecutive high-level sports patients who underwent their anterior cruciate ligament reconstruction technique between 1993 and 1995. The surgical technique uses the hamstring tendons with intact tibial insertions for intra-articular double-stranded reconstruction plus an extra-articular plasty (augmentation) performed with the remnant part of the tendons. Clinical and radiographic evaluations were performed.
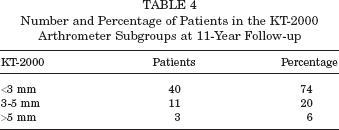
Results: After 11 years, the International Knee Documentation Committee score demonstrated good or excellent results (A and B) in 90.7% of patients. Ligament arthrometry using the KT-2000 arthrometer demonstrated that only 2 patients had >5 mm manual maximum side-to-side difference in laxity. The mean Tegner activity score was 4.5, while the mean Lysholm score was 97.3 and the mean subjective score was 90.0%. Radiographic evaluation demonstrated progressive joint narrowing only for the 20 patients having concomitant medial meniscal surgery.
Conclusion: The original technique demonstrates highly satisfactory results. Factors negatively affecting the outcomes are meniscectomy and laxity. In this series, anterior cruciate ligament reconstruction with lateral plasty shows maintenance of knee stability at long-term follow-up. Knee osteoarthritis after anterior cruciate ligament reconstruction with extra-articular tenodesis does not appear to be greater than after anterior cruciate ligament reconstructions without extra-articular augmentation as reported in historical controls.
Keywords
In the literature, there is no clear evidence that anterior cruciate ligament (ACL) reconstruction is capable of preventing osteoarthritis. Moreover, many variables have been shown to influence the onset of late degenerative joint disease and the final clinical result of ACL reconstruction. Meniscectomy has been shown to increase osteoarthritis and laxity of the knee when ACL reconstruction has been performed.3,15,25,54,55,57,65 Range of motion limitations could also have a detrimental effect on clinical outcome at long-term follow-up and may also be responsible for premature osteoarthritis.43,46,54 Time from injury to surgery is another factor that may influence the final result, due to the stretching of peripheral structures that serve as a secondary restraint over time in addition to increasing the risk of meniscal injury.25,35 A decreased activity level has also been shown to affect some of the outcome values of ACL reconstruction at long-term follow-up. 11
Recently, a more anatomic ACL reconstruction has been advocated to increase the rotational control of the knee after ACL injury to improve clinical outcomes and reduce the rate of arthritis. 69 In vitro tests17,18,48 and a few clinical studies23,38 have shown better results for double-bundle ACL reconstruction. The concept is that this technique should be able to better restore knee kinematics and thus improve knee function; potentially reduce the number of failures; and postpone, delay, or prevent degenerative joint disease. Anatomic reconstruction with double-bundle ACL reconstruction is not a new concept, nor is attempting to better control rotational laxity. Extra-articular augmentation was proposed as a means to control rotational instability in ACL-deficient knees. In theory, extra-articular plasty, due to its peripheral location of the lever arm, was thought to be twice as effective in controlling rotation. 41 In vitro biomechanical analysis of extra-articular plasty demonstrated a reduction of rotation with decreased force in the ACL graft of up to 43%. 13 In the last 20 years, several studies evaluated the efficacy of extra-articular plasty with conflicting results.6,24,28,40,41,47,59
However, clinical studies have not clarified the efficacy and the role of extra-articular augmentation with ACL reconstruction. Roth et al, 47 O'Brien et al, 41 and Strum et al 59 did not show any improvement in clinical outcomes when adding extra-articular augmentation to intra-articular ACL reconstruction and, in fact, they found an increased morbidity using the lateral procedure. On the contrary, Lerat et al 28 and Noyes and Barber 40 found significant improvement in objective knee laxity when adding the extra-articular procedure to a single-bundle ACL reconstruction. The potential downsides to using an extra-articular augmentation with an intra-articular ACL reconstruction include the increased risk of surgical morbidity and the potential risk of increased stress on the lateral compartment that may result in late degenerative changes. Thus the potential risks, combined with difficulty in determining the exact role of extra-articular augmentation in ACL reconstruction, have progressively led to an abandonment of extra-articular augmentation, especially in North America.
There are few published studies with long-term follow-up of combined intra- and extra-articular ACL reconstruction, and most of those used the patellar tendon as the intra-articular graft.2,28 In the last 2 decades, the use of hamstring tendons has become more popular due to the relatively low complication rate as compared with the bone–patellar tendon–bone graft.14,43,44,46,50,52 Further, few studies have reported the long-term results of ACL reconstruction using hamstring tendons as the graft source, and those studies report satisfactory results.21,37,43,49
In 1993, we developed a unique surgical procedure that utilizes the hamstring tendons with intact tibial insertion distally for an intra-articular ACL reconstruction and extra-articular augmentation performed with the remnant part of the hamstring graft. 34 The combination of intra-and extra-articular procedures was developed to address knee laxity, both anteroposterior and rotational; improve graft strength properties; and improve outcomes.
The aim of this study was to prospectively evaluate our intra-articular ACL reconstructive procedure with extra-articular augmentation at minimum 10-year follow-up, to identify the variables that could affect the clinical results, assess the rotational laxity, and evaluate the onset of osteoarthritis in this procedure, comparing these data with those at 5-year follow-up. 36
Materials and Methods
Patient Selection
Between 1993 and 1995, we enrolled 60 consecutive patients (45 male, 15 female), who underwent an ACL reconstruction technique using a hamstring tendon graft intra-articularly with extra-articular augmentation developed by the senior author (MM), in a prospective study. The inclusion criteria for this study were (1) age between 15 and 50 years, (2) normal contralateral knee with no history of trauma or surgery, (3) no osteochondral lesion larger than 3 cm2, and (4) activity being equivalent to participating in cutting sports at a competitive or amateur level. At midterm follow-up (mean 6.4 years), 50 patients were available for evaluation, whereas for this long-term follow-up (mean 11 years) we were able to locate 4 more patients, totaling 54 patients (90% follow-up). Forty-two patients were male and 12 were female. Thirty-one right knees were involved and 23 left knees. Twenty-six patients were treated for acute injuries (less than 3 weeks after injury), while 28 were treated for chronic injuries.
Ethics
The Ethics Committee of Rizzoli Orthopaedic Institute approved our prospective study.
Surgical Technique
All procedures were performed by the senior author, using the surgical technique described previously. 34 The graft used was the semitendinosus and gracilis tendons, sutured together as a double-stranded graft. The tibial insertion was left intact. The tendons were passed through the tibial tunnel and “over the top” of the femur. Ten cycles of knee flexion-extension were performed for graft pretensioning. A groove was made with an osteotome on the lateral aspect of the lateral condyle of the femur to freshen the bone to enhance healing of the graft to the femur while aiding in graft stabilization. The knee was flexed to 90° with external tibial rotation and a posterior drawer applied, and the tendons were then fixed to the cortical bone of the femur using 2 bone staples. The remaining part of the graft was then passed deep to the iliotibial band and fixed with a single staple onto Gerdy's tubercle as extra-articular plasty with the knee flexed to 90° (Figure 1).
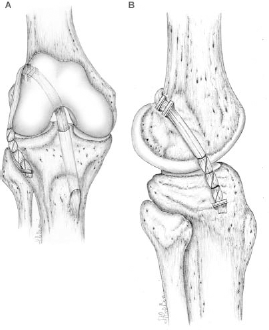
Anterior cruciate ligament reconstruction with hamstring tendons plus extra-articular plasty. A, anteroposterior view; B, lateral view.
Postoperative Protocol
All patients underwent the same postoperative rehabilitation protocol. A brace was not used postoperatively. Range of motion, quadriceps muscle active exercises, straight-leg raises, and prone hamstring muscle-stretching exercises were all begun the day after surgery. Functional muscle stimulation was used 2 hours, 3 times daily, for 4 weeks. Patients were allowed partial weightbearing during the first 2 weeks. Further, patients were allowed full passive extension and active flexion through the range of 0° to 120° from the third postoperative day. At the third week postoperatively, full weightbearing was allowed. Stationary biking, active knee extension with weights, and 1-quarter squats were introduced 4 weeks after surgery. All exercises were performed under the guidance of a physical therapist in a standard fashion that ensured patient compliance with the rehabilitation program.
Proprioceptive exercises were introduced at 4 weeks, running at 2 months, and sports activities after 4 months. Patients were allowed to return to full sports activities when there was no muscle atrophy of the operated leg, or less than 1 cm of atrophy as compared with the contralateral leg, and the one-legged hop was more than 90% of the contralateral leg. These measurements and the decision to return to sports were made by the surgeon and the physical therapist.
Assessment
All patients were assessed preoperatively, then at 5 years and at 11 years after surgery, using the International Knee Documentation Committee (IKDC) evaluation form 22 and the Lysholm knee score. 33 Additionally, resumption of sports at the preinjury level was evaluated by the Tegner score, 61 as well as documentation of the time to resume sport. Clinical evaluation included the Lachman maneuver, the anterior drawer, the pivot shift, and varus-valgus laxity. Instrumented knee laxity was evaluated with the KT-2000 knee ligament arthrometer (MEDmetric Corp, San Diego, California) by measuring side-to-side displacement differences on passive test, manual maximum test, and quadriceps active test. For all patients, standard flexion weightbearing posteroanterior and 30° flexion lateral radiographs were taken at the time of surgery and at follow-up to evaluate for osteoarthrosis using the Ahlbäck score 4 and to measure joint-space narrowing and inspect for osteophytes. 53 Measurements of tibial tunnel placement were determined by the Good method, analyzing the inner orifices’ position with respect to sagittal depth of the medial plateau at the bone cartilage junction. 20 The tibial tunnel diameter was determined 1 cm distal to the ACL insertion on the AP and lateral radiographs. 14 Radiography of the contralateral leg was not performed. The number of reoperations was also recorded.
Statistical Analysis
The Student t test and Mann-Whitney nonparametric tests were used to compare mean values (KT-2000, Lysholm, Tegner, subjective evaluation, intra-articular joint-space measurements). The Pearson χ2 test was used to compare IKDC scores at 5 and 11 years. The minimum range of significance was P = .05.
Results
IKDC and Lysholm Scores
The overall IKDC score showed no difference at the 2 follow-up evaluations for the control knees. In fact, more than 90% of patients had normal or nearly normal control knees at both time periods of follow-up (Figure 2). In particular, on the subjective evaluation at 5 years, the surgically reconstructed knee had a score of 93.5% as compared with the contralateral healthy knee; at 11 years, this score decreased slightly to 90.0%. Further, the Lysholm score demonstrated a mild increase from 94.0 at 5 years to 97.3 at long-term follow-up at 11 years (Table 1).
Functional and Subjective Scores a
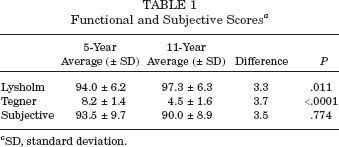
SD, standard deviation.
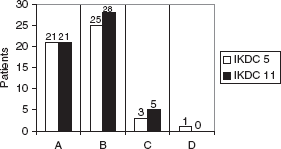
International Knee Documentation Committee (IKDC) score at 5- and 11-year follow-up.
Range of Motion
Extension deficit was measured as the loss of extension of the involved limb as compared with extension in the contralateral, normal control knee. At 5 years, 48 of 50 patients (96%) had regained full extension, while at 11 years, 50 of 54 patients (92%) had full extension. Loss of flexion of more than 5° was found in 1 patient (2%) at 5 years and in 6 patients (11.5%) at 11-year follow-up. Five of these patients with loss of flexion had a C on the IKDC score and the lowest subjective scores.
Manual Testing
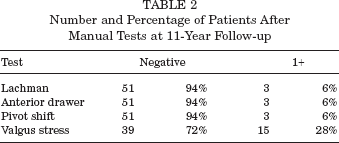
The results of manual knee evaluations were nearly equal over the study period. Three patients who demonstrated a 1+ Lachman, 1+ anterior drawer, and slight pivot shift at 5-year follow-up did not worsen over time, maintaining the same knee evaluation at 11 years. The 15 patients with mild valgus laxity (1+) at 5 years had the same degree of laxity at 11 years (Table 2).
Number and Percentage of Patients After Manual Tests at 11-Year Follow-up
Instrumented Testing
Tables 3 and 4 demonstrate that the KT-2000 instrumented knee arthrometry side-to-side differences at 11 years were similar to those at 5 years, with no significant difference changes over time.
KT-2000 Arthrometer Scores (mm) a
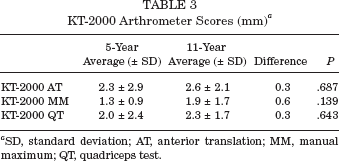
SD, standard deviation; AT, anterior translation; MM, manual maximum; QT, quadriceps test.
Number and Percentage of Patients in the KT-2000 Arthrometer Subgroups at 11-Year Follow-up
Activity Level
Preinjury, the Tegner mean score was 8.8, and was restored to 8.2 after 5 years, while at 11 years, the activity decreased to a 4.5 level (Table 1).
Pain
Anterior knee pain was detected only after strenuous activity in 4 patients. No patient had pain with kneeling or at the harvest site.
Radiographic Findings
The medial, lateral, and patellofemoral compartments were examined for evidence of joint-space narrowing and for the presence of osteophytes (Figure 3). Significant narrowing of the medial joint space was observed in the medial meniscectomized group (20 patients) as compared with those with intact menisci (25 patients) (Table 5). The difference between the 2 groups was 1.17 mm (P = .0095). On the other hand, no significant difference was observed for the lateral compartment (P = .475) (Table 5). For the 3 patients who underwent only lateral meniscectomy and the 6 patients who had both lateral and medial meniscectomy, we decided to evaluate only the Ahlbäck score and the tunnel placement and enlargement, because these 2 small groups were statistically inadequate for joint-space narrowing evaluation and comparison. No degenerative changes were noted in the lateral compartment and no significant worsening of Ahlbäck scores were measured at the last follow-up. Further, no tibial tunnel enlargement was identified when compared with radiographs obtained at the 5-year follow-up. No error in tunnel placement was identified on lateral radiographs.
Medial and Lateral Joint Distance (mm) a
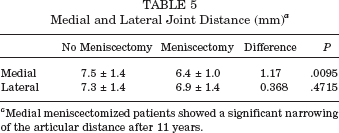
Medial meniscectomized patients showed a significant narrowing of the articular distance after 11 years.

Radiography controls preoperatively (A) and at 12 years and 3 months of follow-up (B) of the right knee of a male patient (no meniscal lesions found at time of surgery).
Complications and Further Surgery
Removal of staples was necessary in 8 patients (13%). Generally, it was the femoral staples that were symptomatic; however, if either the tibial or femoral staple was symptomatic, all were removed. Two patients sustained injury to their contralateral ACL. During the 11-year follow-up period, 3 patients needed arthroscopic partial medial meniscectomy for medial meniscal tears. Postoperatively, 4 patients complained of paresthesias in the saphenous nerve distribution.
Discussion
The results of this study, at a minimum of 10 years of follow-up, demonstrate very good success rates, with more than 90% of knees normal or nearly normal as measured using the IKDC rating system. We also noted a decrease in patient activity at 11 years. Consistent with the findings of Daniel et al, 11 this decrease at long-term follow-up is most likely related to modified lifestyle and reduction of sport activity rather than due to knee problems.
This study is a report of our experience and has as a limitation the lack of a control group of nonsurgically treated patients or patients with ACL reconstruction without an extra-articular tenodesis. The literature is sparse with regard to ACL reconstruction studies that have more than 10-year follow-up. We were only able to find 3 articles reporting ACL reconstruction using hamstring tendon as the graft with a minimum 10-year follow-up.21,37,43 In the case series of Meystre et al, 37 27 patients were evaluated at 10-year follow-up after hamstring graft ACL reconstruction; 96% of those patients had normal or nearly normal knees. Pinczewski et al 43 and Ibrahim et al 21 are the only 2 articles in the literature that we could find that compare patellar tendon and hamstrings ACL reconstruction with 10-year follow-up. The results of those studies were similar in terms of patient satisfaction, activity level, and knee function; in particular, patients in the hamstring graft group had 97% 43 and 84% 21 normal or nearly normal knees. Moreover, the hamstring graft group had fewer patellofemoral problems and loss of knee motion when compared with the patellar tendon graft group. Further, Roe et al 46 found, at an average 7-year follow-up, that there was a greater incidence of degenerative changes in the patellar tendon graft group, while Liden et al, 30 with the same duration of follow-up, did not find any differences in patients with ACL reconstruction comparing the 2 grafts. In a recent meta-analysis, both autografts provided a high rate of success, but the authors found a significantly lower rate of graft failure, a better static knee stability, and increased patient satisfaction in the bone–patellar tendon–bone group; however, this group had an increased rate of anterior knee pain and motion problems requiring surgical treatment. 16
In this series, there was no increase in degenerative changes observed between the 5- and 11-year follow-up after this intra-articular ACL reconstruction with an extra-articular augmentation procedure.
Salmon et al 49 reported a gender comparison of outcome in a series of patients with quadrupled hamstring ACL reconstruction with 7-year follow-up. They noted their results to be 89% and 86% normal or nearly normal knees, when comparing the male and female groups respectively. Beynnon et al 7 and Anderson et al, 6 in studies with 5-year follow-up after ACL reconstruction, reported increasing anteroposterior laxity over time when a single loop of gracilis and semitendinosus tendon were used as the graft. In our series, instrumented arthrometry results did not change between 5 and 11 years.
In the technique reported in this article, the 2 hamstring tendons (semitendinosus and gracilis) were used to reconstruct the intra-articular portion of the ACL reconstruction, leaving their tibial insertion intact. The graft was placed in the over-the-top position, most closely replicating the anatomy of the ACL. Then, with the extra length of the tendons, the extra-articular augmentation (lateral plasty) was performed. This extra-articular augmentation procedure allows better initial control of anteroposterior and rotatory as noted by Zaffagnini et al, using a navigation system intraoperatively (S. Zaffagnini et al, unpublished data, 2008 [poster exhibit at AAOS Annual Meeting]).
Zaffagnini et al 68 have shown that the tibial hamstring insertion is important, as blood vessels enter and supply the graft from the distal (tibial) insertion. Moreover, nerve endings have also been found at the tibial insertion. Since the blood supply for the hamstring tendons comes from distally and the tibial insertion is left intact, there is less likelihood that the graft is avascular. 68 We hypothesize that not losing the vascularization of the graft may allow for earlier or faster incorporation of the graft, and may theoretically be the reason there is no osteolysis or tunnel widening. The concept of enhanced integration of the graft into the tunnel is confirmed indirectly by the fact that although the fixation points of the reconstruction are distant to the intra-articular margin of the reconstruction, no significant tunnel enlargement was observed at 11-year follow-up. Clatworthy et al, 9 L'Insalata et al, 31 and Tsuda et al 62 have shown that tunnel enlargement after ACL reconstruction may be the result of windshield wiper or bungee effects associated with graft fixation distant to the joint. We believe that the lack of significant tunnel enlargement at any point in this study may be the result of early graft incorporation and/or integration into the tunnel, as the fixation sites of the graft are distant relative to the joint.
The presence of the lateral plasty (extra-articular augmentation) protects the graft with less load being applied to the intra-articular portion of the graft. In vitro analysis performed by Engebretsen et al 13 have shown that the extra-articular plasty, when used in combination with intra-articular reconstruction, reduces the stress on the graft by approximately 43%. Sydney et al, 60 using cadaveric knees, demonstrated that extra-articular augmentation with a lateral plasty reduces tibial rotation and the displacement of the lateral compartment with less risk of pivoting of the knee. Draganich et al, 12 in an in vitro study, concluded that combined intra-articular and extra-articular ACL reconstruction does not result in overconstraining the knee by reducing internal rotation and that there is load sharing in both anterior translation and internal rotation.
Some authors41,47,59 have reported a greater risk of degenerative changes in the lateral compartment of the knee when using an extra-articular augmentation. They hypothesize that extra-articular augmentation may overconstrain the knee joint, altering knee kinematics and resulting in joint degeneration as a long-term consequence.
Advanced degenerative change was not observed in our patients, as reported here. In fact, no severe degenerative changes were found in the lateral compartment. Only when medial meniscectomy was performed did we observe a progression of articular change between the 5- and 11-year follow-up evaluations.
The extra-articular procedure used in our technique does not damage any lateral structures commonly used in other extra-articular augmentation procedures. In fact, neither the iliotibial band nor biceps tendon was used or transposed to help control tibial rotation.
The tendons used to perform the extra-articular augmentation (lateral plasty) are part of the intra-articular graft and are fixed in a more isometric position as suggested by Krackow and Brooks. 27 Thus no alteration of the lateral structures is performed, but only an augmentation to excessive coupled rotations is obtained with the extra-articular part of the graft.
As previously observed and reported by Shelbourne and Gray, 54 Wu et al, 65 Cohen et al, 10 Ait Si Selmi et al, 5 Yamaguchi et al, 66 Levy et al, 29 and Warren and Levy, 63 we found a high correlation between meniscectomy and arthritis. It is important to note that no patellofemoral degenerative changes or increase in kneeling pain was observed, as reported by Pinczewski et al 43 in their long-term follow-up of bone–patellar tendon–bone ACL reconstructions.
Another important observation is that most of the patients in this series achieved complete active and passive range of motion as compared with the contralateral knee. In this series, we identified a significant correlation between subjective evaluation, IKDC score, and the maintenance of complete range of motion at long-term follow-up.
It is interesting to note that the cases in which a range of motion deficit was observed at last follow-up were the cases that had a medial or lateral meniscectomy at the time of surgical reconstruction. It may be that the late loss of motion is the result of the degenerative changes associated with the meniscectomy.
The technique presented is a highly reproducible procedure in our hands, with a high percentage of satisfactory results, and eliminates the risk of surgical error that may be associated with placement of the femoral tunnel. Although the over-the-top position is not exactly an anatomic reconstruction, Karlson et al 26 have shown that no significant clinical differences were identified when comparing patients who underwent hamstring ACL reconstruction using the over-the-top position with those who had a drilled femoral condylar tunnel for femoral graft placement in a prospective study.
Another benefit of this technique is that it uses only 3 titanium staples for graft fixation, which results in a reduction of surgical costs. This technique is also a simple solution for revision cases, eliminating the issues of management of femoral tunnel malposition, presence of intra-articular hardware, or tunnel enlargement. Yiannakopoulos et al 67 reported 86% satisfactory results for revision ACL reconstruction using the over-the-top position.
The highly satisfactory results obtained in this series show that, from a clinical point of view, a combination of intra- and extra-articular procedures for ACL reconstruction is a valid option.
Pearl and Bergfeld 42 concluded that there is a limited role for extra-articular procedures, but we propose that this thinking should be reconsidered. Although we acknowledge that the majority of ACL reconstruction can be solved by an isolated intra-articular reconstruction, we do believe there is need to reconsider the use of extra-articular augmentation. First, in many series, the failure rate of ACL reconstruction using a single-bundle intra-articular reconstruction may reach 25% of the cases. The cause of graft failure, and potentially degenerative arthritis, may be attributed to lack of rotational control with a single-bundle intra-articular ACL reconstruction. For this reason, recently some authors1,38,48,56 have suggested a more anatomic reconstruction (double bundle) to better control the rotational component laxity. In other studies, it has been suggested that for higher demand activities, no graft and no technique seems to be able to control tibial rotation.8,19,45 Perhaps current procedures do not correctly reproduce the complex 3-dimensional ACL structure. Some authors recommend use of a more lateral 58 and oblique32,39,51,64 femoral tunnel to increase the moment arm and to reproduce the posterolateral bundle, which has been revealed to be fundamental in rotational control. 19 Our procedure, by attempting to control rotation laterally, further away from the pivot point of the knee, may be better suited to control rotational motion by having a better lever arm. A simple intra-articular procedure combined with an extra-articular augmentation may achieve better results in maintaining rotational control with less risk of technical error and complications as compared with the double-bundle technique. This may be one of the reasons why we did not have any patients with severe degenerative joint disease. However, as our study did not include a control group with only an intra-articular procedure, we cannot know for certain that the extra-articular portion of the reconstruction improved the results. We agree with Pearl and Bergfeld 42 that there still is a lack of research validation of the extra-articular augmentation to effectively control rotational stability of the knee; however, this could be performed with computer-assisted surgery in vivo in the future.
In conclusion, we found that a combination of single-bundle ACL reconstruction plus extra-articular augmentation is capable of maintaining stability, and without an increased rate of degenerative arthritis, at more than 10 years’ follow-up. On the basis of our experience, we think that the reasons for these satisfactory results using a nonanatomic and double-stranded hamstring technique are the easy and highly repeatable surgery, the aggressive rehabilitation, the fast recovery, and the restoration of stability. Based on our laboratory tests and in vivo studies, we believe the extra-articular tenodesis improves the control of rotational laxity. But we need a control group to prove that it is one of the keys for slowing down the degenerative joint disease process.