
Abstract
Background: Tears of the gluteus medius tendon at the greater trochanter have been termed “rotator cuff tears of the hip.” Previous reports have described the open repair of these lesions.
Hypothesis: Endoscopic repair of gluteus medius tears results in successful clinical outcomes in the short term.
Study Design: Case series; Level of evidence, 4.
Methods: Of 482 consecutive hip arthroscopies performed by the senior author, 10 patients with gluteus medius tears repaired endoscopically were evaluated prospectively. Perioperative data were analyzed on this cohort of patients. There were 8 women and 2 men, with an average age of 50.4 years (range, 33-66 years). Patients had persistent lateral hip pain and abductor weakness despite extensive conservative measures. Diagnosis was made by physical examination and magnetic resonance imaging and was confirmed at the time of endoscopy in all cases. At the most recent follow-up, patients completed the Modified Harris Hip Score and Hip Outcomes Score surveys.
Results: At an average follow-up of 25 months (range, 19-38 months), all 10 patients had complete resolution of pain; 10 of 10 regained 5 of 5 motor strength in the hip abductors. Modified Harris Hip Scores at 1 year averaged 94 points (range, 84-100), and Hip Outcomes Scores averaged 93 points (range, 85-100). There were no adverse complications after abductor repairs. Seven of 10 patients said their hip was normal, and 3 said their hip was nearly normal.
Conclusion: With short-term follow-up, endoscopic repair of gluteus medius tendon tears of the hip appears to provide pain relief and return of strength in select patients who have failed conservative measures. Further long-term follow-up is warranted to confirm the clinical effectiveness of this procedure.
Similar to knee and shoulder arthroscopy, pathologic conditions that were once addressed with open techniques are now routinely treated in the hip with an arthroscopic approach such as labral tears, loose bodies, femoroacetabular impingement, chondral lesions, tears of the ligamentum teres, coxa saltans (snapping hip syndrome), and synovial chondromatosis.11,19
Symptomatic tears of the abductor tendons of the hip are another entity that can now be evaluated endoscopically. Previous reports have noted the similarities between the insertion of the gluteus medius and minimus tendons at the greater trochanter and the rotator cuff tendons at the greater tuberosity, leading some authors to define these injuries as “rotator cuff tears of the hip.”3,8,9,13 Treatment was described in an open fashion when encountered as an incidental finding in the setting of refractory iliotibial band syndrome and hip arthroplasty. The true incidence of gluteus medius and minimus tears is unknown in the general and athletic population. A prospective study by Bunker et al 3 of 50 patients with fractures of the femoral neck revealed a 22% incidence of tears of the gluteus medius and minimus. In another prospective study of 176 consecutive patients who underwent total hip arthroplasty for osteoarthritis, Howell et al 7 identified 20% with degenerative changes of the abductor mechanism.
Recently the senior author (B.T.K.) described a surgical technique for treatment of diseases of the peritrochanteric space and the endoscopic repair of gluteus medius and minimus tears. 20 To our knowledge, this is the first report describing the outcome of patients with gluteus medius and minimus tears repaired endoscopically.
Materials and Methods
Of 482 consecutive hip arthroscopies performed by the senior author, 10 patients (8 women and 2 men) with gluteus medius tears repaired endoscopically were evaluated prospectively. Average follow-up was 25 months (range, 19–38 months). Average age was 50.4 years (range, 33–66 years). Preoperative, intraoperative, and postoperative data were analyzed on this cohort of patients. All patients had persistent lateral hip pain and abductor weakness despite extensive conservative measures including physical therapy, anti-inflammatory drugs, and ultrasound-guided corticosteroid injection of the trochanteric bursa. Diagnosis was made by physical examination, radiographs of the hip and pelvis, and magnetic resonance imaging (MRI) and was confirmed at the time of endoscopy in all cases (Figure 1).
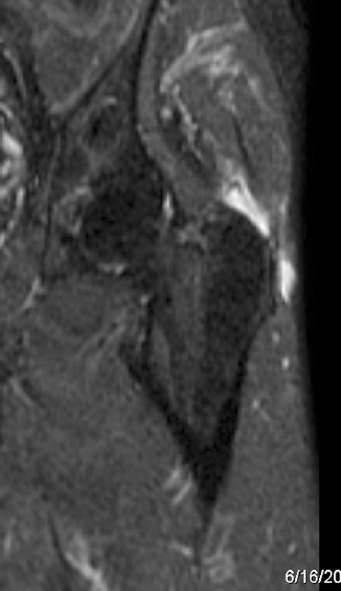
Magnetic resonance imaging of the left hip preoperatively, revealing increased signal within the gluteus medius tendon at the attachment to the greater trochanter consistent with a tear.
Abductor strength was assessed by manual resistance with the patient in the lateral decubitus position. All MRIs were read by senior radiologists at our institution who specialize in musculoskeletal imaging. No patient had any previous surgery, open or arthroscopic, on the hip. One patient had a previous ipsilateral sacroiliac joint fusion. All patients underwent diagnostic intra-articular arthroscopy and endoscopic evaluation of the lateral peritrochanteric space of the hip. A complete bursectomy was performed using a mechanical shaver to allow visualization of the abductor tendon. Next, 5.0-mm metal suture anchors (Linvatec, Largo, Florida) were used to repair gluteus medius and minimus tears as we have previously described (Figures 2 and 3). 20

Endoscopic image of the left hip with the probe displaying a full-thickness tear of the gluteus medius tendon.

Endoscopic image of the left hip after final repair of the gluteus medius tear.
Postoperative rehabilitation consisted of 6 weeks of crutch-protected weightbearing with the goal of 20 lb of pressure on the operative extremity. A continuous passive motion (CPM) machine was begun in the recovery room and continued as an outpatient. An abduction brace was used for 6 weeks. Gentle passive range of motion began the first postoperative week. At 6 weeks, active range of motion was begun, and early abductor strengthening was started. By the third month, strengthening continued, and sport-specific activity was begun by month 4. Running was not allowed until abductor strength was equal to the contralateral side by manual testing. At the most recent follow-up visits, patients completed the Modified Harris Hip Score and Hip Outcomes Score surveys as validated by Martin et al. 15
Results
Ten of 10 patients (8 left and 2 right hips) reported lateral hip pain as the predominant symptom. Six of 10 patients (60%) had an acute injury that resulted in the onset of symptoms. In these 6 patients, the mechanism was a fall. The remaining 4 patients had insidious onset of symptoms limiting daily activities. Ten of 10 patients had tenderness to palpation over the greater trochanter on examination, and 9 of 10 patients (90%) had 4 of 5 muscle strength on a scale of 5 with manual testing of the abductor muscles. One patient (10%) had full muscle strength but displayed pain over the abductors with active abduction. One patient had groin pain with flexion and internal rotation of the hip, and 1 patient had snapping of the iliotibial band in addition to lateral hip pain. There were no limitations of hip range of motion in any patient. All 10 patients underwent therapeutic and diagnostic injection of the trochanteric bursa with corticosteroid, and 5 patients underwent 2 or more injections with at least short-term resolution of pain. All patients reported the duration of symptoms to be a minimum of 3 months without any resolution through traditional conservative measures including rest, physical therapy, anti-inflammatory medications, and corticosteroid injections.
Radiograph findings of the hip were normal in 5 of 10 patients (50%). Two patients (20%) had pincer-type femoroacetabular impingement lesions, 1 (10%) had mild acetabular protrusion, 1 (10%) had exostosis of the greater trochanter, and 1 (10%) had sacroiliac arthrodesis. The MRI of the hip revealed increased signal intensity in the trochanteric bursa along with increased signal within the gluteus medius tendon consistent with a tear. No patient had complete avulsion of the abductor tendon footprint from the greater trochanter or evidence of atrophy within the muscle. Eight of 10 (80%) patients displayed anterior labral tears, 1 (10%) displayed mild osteoarthritis, 1 (10%) displayed hypertrophic labrum, and 1 (10%) displayed exostosis of the greater trochanter.
At the time of endoscopy, 5 (50%) patients had full-thickness tears of the gluteus medius tendons from the greater trochanter that were repaired with suture anchors. Five (50%) patients had high-grade partial-thickness tears that were identified after bursectomy and examined with a probe. These tears were completed and repaired in the same fashion as the full-thickness tears. All patients underwent bursectomy of the greater trochanteric bursa, 8 of 10 (80%) patients underwent anterior labral debridement, 1 (10%) underwent labral repair, 1 (10%) underwent exostectomy of the greater trochanter, 1 (10%) underwent debridement pincer lesion, 1 (10%) underwent release of the iliotibial band, and 2 (20%) underwent psoas tendon release.
At an average of 2 years’ follow-up, all patients had complete resolution of pain in the lateral hip. Ten of 10 (100%) patients had 5 of 5 abductor muscle strength. All patients maintained full hip range of motion. One patient developed new groin pain at the time of most recent follow-up. There were no clinical failures of the abductor repair and no perioperative complications in this group.
Modified Harris Hip Scores at 1 year averaged 94 points (range, 84–100), and Hip Outcomes Scores averaged 93 points (range, 85–100). Seven of 10 patients said their hip was normal, and 3 said their hip was nearly normal. Additionally, 3 patients had follow-up MRIs at a minimum of 6 months to assess healing of the abductor tendon. All 3 demonstrated healed tendons with no evidence of retear (Figure 4).

Magnetic resonance imaging of the right hip at 12 months postoperatively, revealing an intact repair of the gluteus medius tendon with suture anchors (*) present.
Discussion
Recent advances in hip arthroscopy have led to a significant evolution in its use for the treatment of athletes and patients in the general public with a broad spectrum of hip lesions. Recalcitrant hip pain and lack of response to conservative management with a presumed diagnosis of trochanteric bursitis constitute a relative indication for MRI.5,11,19 This may reveal a previously unappreciated tear of the gluteus medius, which has been well described in the literature as a possible cause of greater trochanteric pain syndrome.2,4,12,13 In this study, we prospectively evaluated the results of patients undergoing endoscopic repair of the gluteus medius tendons. To our knowledge, this is the first report describing the results of endoscopically repaired hip abductors.
In our series of patients with short-term follow-up, all 10 cases experienced complete resolution of lateral hip pain, and 100% of patients regained full motor strength. Weaknesses of our study include small sample size, short-term follow-up, lack of preoperative baseline outcomes measures, and lack of quantitative strength testing.
Several authors have described tears of the gluteus medius and minimus tendons as “rotator cuff tears of the hip.”3,8,9 As with rotator cuff tears in the shoulder, it could be hypothesized that the “rotator cuff tears” of the hip may also be associated with increasing age. Although the cause is uncertain, tears of the hip abductor tendons may also occur through a progressive, degenerative process as they do in aging rotator cuff tears in the shoulder.4,5,17,18,21
Studies have yet to determine the true incidence of gluteus medius and minimus tears in the athlete and general population and their correlation with symptomatic hip pathology. A prospective study by Bunker et al 3 of 50 patients, average age of 83.5 years (range, 56–98 years), with fractures of the femoral neck revealed a 22% incidence of tears of the gluteus medius and minimus treated with open repair. No suture anchors were used. In another prospective study of 176 consecutive patients who underwent total hip arthroplasty for osteoarthritis, Howell et al 7 identified 20% of patients with degenerative lesions of the abductor mechanism. The hip capsule usually was involved, but in 6 patients (16%), the gluteus minimus or medius tendons were involved in isolation. After completion of the arthroplasty, tears of the gluteus minimus and gluteus medius were repaired. If necessary, bone sutures were employed to reattach the tendinous insertion of the gluteus medius. Tears were more common in women, and the prevalence increased with age for men and women. Kagan8,9 described tears of the gluteus medius and minimus encountered during open surgical treatment of recalcitrant trochanteric bursitis in 7 patients with an average age of 69 years. The tendons were reattached to bone using heavy nonabsorbable suture. At a median follow-up of 45 months, all patients were pain free.
Calcific tendinitis of the hip abductors and trochanteric bursitis have been described by some authors as contributing to gluteus medius and minimus pain.6,14 The successful treatment of trochanteric bursitis and calcific tendinitis of the gluteus medius and minimus through an arthroscopic (eg, endoscopic or bursoscopic) approach has recently been described in the literature in a patient with a 2-year history of lateral hip pain. 10 Also, Baker et al 1 recently published a prospective follow-up in 25 patients treated with endoscopic bursectomy at a mean follow-up of 26.1 months and demonstrated significant improvements using visual analog scores, Harris Hip Score, and SF-36. None of the patients in this study underwent repair of the abductor tendons. All 10 patients in our study displayed increased signal in the trochanteric bursa on preoperative MRI and underwent trochanteric bursectomy before abductor repair. Trochanteric bursectomy alone may be sufficient to alleviate pain in patients with recalcitrant trochanteric bursitis. In concert with trochanteric bursectomy, repair of the abductor tendons may contribute to pain relief and regaining strength of the gluteus medius when the combination of lateral hip pain, abductor weakness, increased signal intensity on MRI, pain relief with lateral hip injection, and a confirmed tear at the time of endoscopy are present.
Magnetic resonance imaging has aided in diagnosing tears of the gluteus medius tendon in patients with suspected trochanteric bursitis and an ambulatory limp due to weakness in the hip abductors that failed conservative treatment.5,16,19 We routinely rely on noncontrast MRI to assist in confirming our clinical findings in preparation for surgery. Each MRI of the hip performed at our institution includes a screening examination of the whole pelvis, acquired with use of coronal inversion recovery and axial proton density sequences. Imaging is obtained with use of a surface coil over the hip joint, with high-resolution, cartilage-sensitive images acquired in 3 planes (sagittal, coronal, and oblique axial) with use of a fast-spin echo pulse sequence and an intermediate echo time. 19 Although MRI is excellent for intra-articular lesions, we have found it difficult to delineate high-grade partial tears of the abductor tendons from full-thickness tears. We rely on our knowledge of the anatomy of the abductor tendon footprint on the greater trochanter 16 and area of increased signal on MRI 17 to identify the site of injury at the time of endoscopy. When a complete avulsion of the abductor tendons from the greater trochanter with retraction is present on MRI, we routinely address these with an open repair. Given the early evolution of this technique, we believe that an open repair will have the opportunity for a more durable repair in the setting of complete tendon avulsion with retraction. As techniques improve, it may become feasible to address even these larger tears with an all endoscopic technique.
In conclusion, endoscopic repair of the gluteus medius tendons to the greater trochanter can be performed in a reproducible manner. In the short term, resolution of pain and return to activity are predictable. Long-term follow-up and a larger number of patients in prospective trials will provide further insight into the treatment of abductor tendon tears.