
Abstract
Background: There is inadequate evidence to determine when to perform surgery on anterior cruciate ligament—deficient knees.
Purpose: To study the association between timing of anterior cruciate ligament reconstruction and the risk of having meniscal tears and cartilage lesions.
Study Design: Cohort study (prognosis); Level of evidence, 2.
Methods: All patients registered in the Norwegian National Knee Ligament Registry who had undergone primary anterior cruciate ligament reconstruction from 2004 and throughout 2006 were reviewed. Logistic regression analyses were used to estimate the relationship between time from injury until anterior cruciate ligament surgery and the risk of meniscal tears or cartilage lesions.
Results: Of a total of 3475 patients, there were 909 patients (26%) with cartilage lesions, 1638 patients (47%) with meniscal tears, and 527 patients (15%) with both cartilage and meniscal lesions. The odds of a cartilage lesion in the adult knee (>16 years) increased by 1.006 (95% confidence interval, 1.003-1.010) for each month that elapsed from injury to surgery. The cartilage in young adults (17-40 years) deteriorated further with an increase in odds of 1.03 (95% confidence interval, 1.02-1.05) related to the aging in years of the patient. The odds for meniscal tears in young adults increased by 1.004 (95% confidence interval, 1.002-1.006) for each month that elapsed since injury. The presence of 1 degenerative lesion increased the odds of having the other degenerative lesion by between 1.6 and 2.0 in all patient groups.
Conclusion: The odds of a cartilage lesion in the adult knee increased by nearly 1% for each month that elapsed from the injury date until the surgery date and that of cartilage lesions were nearly twice as frequent if there was a meniscal tear, and vice versa.
The decision on when to perform surgery on an ACL-deficient knee varies among knee surgeons. Whereas there is some agreement on being conservative and delaying surgery in children with open physes until skeletal maturity is reached, 10 timing of surgery in the adult population varies from the very first day after the injury to several years due to a long waiting list or the choice of the patient or surgeon. Surgery was frequently done acutely in the late 1970s and early 1980s, but a study by Shelbourne et al 14 from 1991 on avoiding arthrofibrosis changed the field from a time-dependent to a function-dependent timing of surgery. Their data suggested that surgery should be performed after the swelling has subsided and range of motion is normal. A review of the literature on the treatment of ACL injuries by Beynnon et al 1 concluded that “it appears that the time interval from ACL injury to reconstruction is not as important as the condition of the knee at the time of surgery.” Despite this, a recent study 2 concluded that primary ACL reconstruction surgery should be carried out within 1 year after injury to minimize the risk of meniscal tears and degenerative changes.
The present study is based on data from the Norwegian Knee Ligament Registry (NKLR), established in 2004, 4 with the aim to study the association between timing of ACL reconstruction and the risk of having meniscal tears and cartilage lesions in the ACL-injured knee.
Materials and Methods
We reviewed all patients registered in the NKLR who had undergone primary ACL reconstruction surgery in Norway between June 7, 2004, and December 31, 2006.
The NKLR is a cohort designed to collect information prospectively on all cases of cruciate ligament reconstruction surgery performed in Norway. Because of logistic and diagnostic issues, patients not receiving surgical treatment for their ACL injuries are currently not included in the NKLR cohort. 4 Thus, no control group is included in this study.
The NKLR makes use of both objective and subjective end points. The hard end points are revision surgery after cruciate ligament surgery and insertion of a total knee replacement. The NKLR includes routine follow-ups on all patients at 2, 5, and 10 years postoperatively using the Knee Injury and Osteoarthritis Outcome Score (KOOS) 9 as a soft end point. The KOOS form is also completed preoperatively by the patients.
The NKLR has a compliance rate of 97% with respect to all reconstructive ACL surgeries in Norway. Further details about the registry are described in Granan et al (2008). 4
From the NKLR, we obtained preoperative details about age at time of surgery, sex, date of injury and date of surgery, location of any associated meniscal tears, and location and grading (according to the International Cartilage Repair Society [ICRS]) 7 of any associated cartilage lesions.
The patients were divided into 3 different age groups according to age at time of surgery: children, 16 years and younger; young adults, 17 to 40 years; and older adults, 41 years and older. Children are expected to differ from adults due to skeletal immaturity, whereas older adults are expected to differ from younger adults due to the natural process of degenerative changes in the aging knee.
Logistic regression analyses were used to estimate the relationship between time from injury until primary reconstructive ACL surgery and the risk of meniscal tears or cartilage lesions. The risk for cartilage lesion (1) or not (0), as well as for meniscal tears (1) or not (0), was studied using the logistic regression models. First, unadjusted analyses were performed to identify potential confounders. The relationships between time from injury until surgery and risk factors and between potential confounders and the risk of cartilage lesions or meniscal tears were calculated. Risk factors with a significant relationship (using P < .20) with time from injury until surgery and potential confounders with a significant relationship (using P < .20) to either cartilage lesion or meniscal tear prevalence were used as adjustment factors for potential confounding in the adjusted logistic regression models. The factors identified were age, sex, previous knee joint surgery (ie, surgery to medial collateral ligament [MCL], lateral collateral ligament [LCL], posterolateral corner [PLC], cartilage, medial meniscus, lateral meniscus, or other specified structure), current knee ligament injury (ie, LCL, MCL, and/or PLC), meniscal tears, and cartilage lesions. The analyses were stratified by age groups and adjusted for time to surgery, sex, age (as a continuous variable), previous knee joint surgery, current knee ligament injury, and the presence of cartilage lesions or meniscal tears at the time of surgery.
Unadjusted analysis was performed to estimate the mean difference in months from injury until surgery between risk factors and confounding factors. P values less than .05 were considered to be statistically significant. Odds ratios are presented with 95% confidence intervals (CIs).
All statistical analyses were performed using SPSS for Windows, version 15.0 (SPSS, Chicago, Illinois).
Results
A total of 4212 procedures were registered in the NKLR, and 3699 of these were primary ACL reconstructions (Figure 1). After excluding patients with previous or current posterior cruciate ligament injury or surgery and cases in which the date of injury was unknown, we were left with 3475 knees. The median time from injury to surgery was 7 months (range, 9 days to 482 months). Of the 3475 cases identified, there were 1977 (57%) male and 1498 (43%) female patients, with a median age of 27 years (range, 12–67 years).
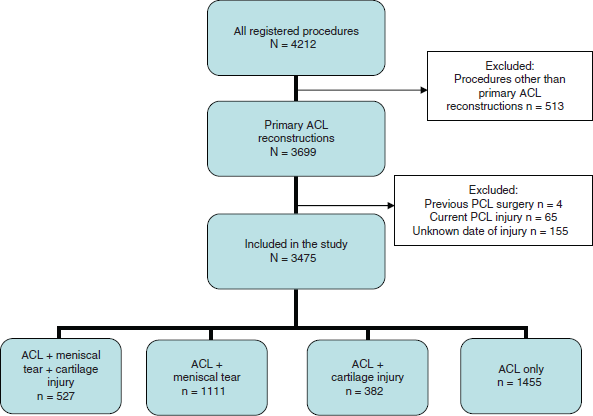
Patient distribution and exclusion criteria.
The number of patients, sex, age, distribution of current and previous surgeries, and distribution of meniscal and cartilage injuries across age groups are shown in Table 1. Of 246 cases with at least 1 cartilage lesion grade 3 or 4, 120 cases (49%) had 1 or more lesions larger than 2 cm2.
Patient Characteristics and Injury Distribution at Time of Surgery
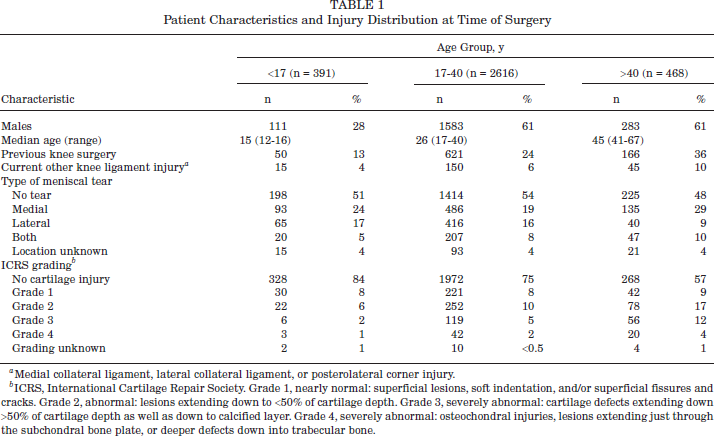
Medial collateral ligament, lateral collateral ligament, or posterolateral corner injury.
ICRS, International Cartilage Repair Society. Grade 1, nearly normal: superficial lesions, soft indentation, and/or superficial fissures and cracks. Grade 2, abnormal: lesions extending down to <50% of cartilage depth. Grade 3, severely abnormal: cartilage defects extending down >50% of cartilage depth as well as down to calcified layer. Grade 4, severely abnormal: osteochondral injuries, lesions extending just through the subchondral bone plate, or deeper defects down into trabecular bone.
Among children, we were not able to detect a significant effect of time elapsed from injury until surgery on the prevalence of either cartilage lesions (Table 2) or meniscal tears (Table 3). The presence of cartilage lesions led to increased odds for the presence of meniscal tears (Table 3). Conversely, the odds for cartilage lesions were also increased in the presence of meniscal tears (Table 2). Within this age group, we also found that the prevalence of meniscal tears decreased with age.
Logistic Regression Analysis of Cartilage Lesions a
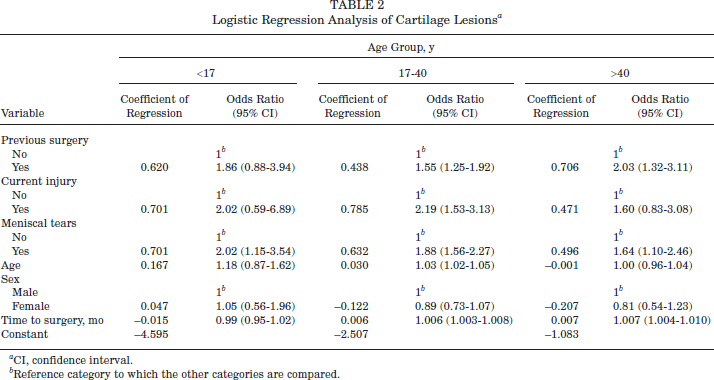
CI, confidence interval.
Reference category to which the other categories are compared.
Logistic Regression Analysis of Meniscal Tears a
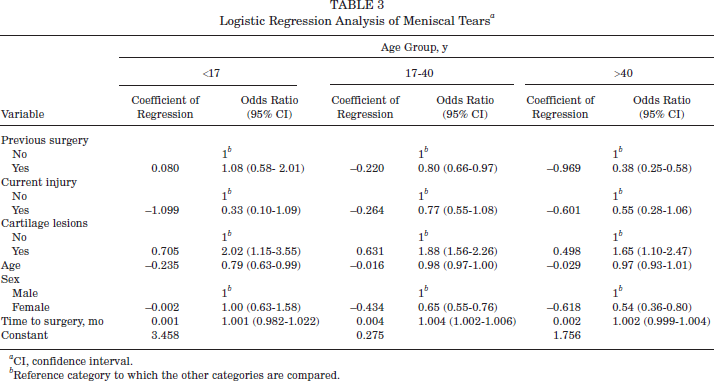
CI, confidence interval.
Reference category to which the other categories are compared.
In the young adult group, there were several factors that influenced the prevalence of cartilage and meniscal lesions. An increase in odds with time to surgery was seen for both types of lesions. The odds for a cartilage lesion increased by 1.006 (95% CI, 1.003–1.008) for each month that elapsed from the injury date until the surgery date. The same applied to meniscal tears, where we observed a monthly increase in odds by 1.004 (95% CI, 1.002–1.006). Previous surgery increased the odds for having a cartilage lesion (Table 2), whereas it decreased the odds for having a meniscal tear (Table 3). A current injury of the MCL, LCL, and/or PLC was associated with increased odds for cartilage lesions (Table 2). The presence of a meniscal tear increased the odds for cartilage lesions (Table 2) and vice versa (Table 3). The older the young adults were, the higher the odds were for a cartilage lesion (Table 2), whereas the odds for having a meniscal tear decreased with increasing age (Table 3). Being female reduced the odds of having a meniscal tear (Table 3), whereas there was no gender effect on the risk for cartilage lesions (Table 2).
In the older adult group, the odds for having a cartilage lesion increased by 1.007 (95% CI, 1.004–1.010) for each month that elapsed from the injury date until the surgery date, whereas there was no association between time until surgery and the odds for meniscal tears. The presence of previous surgery to knee ligaments, cartilage, and/or menisci increased the odds for having cartilage lesions (Table 2), whereas the odds for having meniscal tears were decreased (Table 3). An additional meniscal tear increased the odds for a cartilage lesion (Table 2) and vice versa (Table 3). Being female reduced the odds of having a meniscal tear (Table 3), but there was no effect on the odds for cartilage injuries.
Table 4 displays the mean differences in months from injury until surgery between sexes, previous knee joint surgery to the index knee, current knee ligament injury other than cruciate ligament injuries, patient age groups, and the presence of either meniscal tears or cartilage lesions.
Mean Difference in Months From Injury Until Surgery Between Risk Factors and Confounding Factors
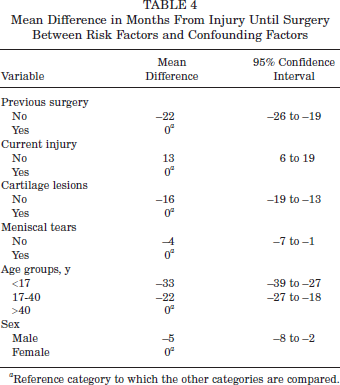
Reference category to which the other categories are compared.
Discussion
The main findings of this study were that the odds for a cartilage lesion in the adult knee increased by nearly 1% for each month that elapsed from the injury date until the surgery date and that cartilage lesions were nearly twice as frequent if there were a meniscal tear and vice versa.
The main strength of our study is the large number of patients included. Another strong point is that the patients originated from a national and general population of ACL-injured patients. The main weakness of this study is that all details regarding the patients are solely based on the individual orthopaedic surgeons reporting to NKLR. The collected data regarding the condition of the cartilage and menisci are based on the arthroscopic findings of many different surgeons, and their estimations of cartilage injury location, size, and depth may vary. One level III study regarding ICRS scoring has been published suggesting that this system is valid for the assessment of cartilage repair and has been found to have good interpersonal value and be repeatable and, as such, is regarded as a precise tool in the evaluation of cartilage repair. 9
In the present study, patients who had asymptomatic cartilage or meniscal injury before their ACL injuries represent a potential source of bias. One cannot be entirely sure that the cartilage and meniscal tears reported to the NKLR had been sustained at or after the index ligament injury. Another potential limitation is that patients who expect instability to be a problem or cannot afford instability problems (eg, manual laborers, professional athletes, those who perform pivoting leisure-time activities) are more likely to undergo surgery early in contrast to patients who receive surgery after having experienced at least 1 episode of instability or giving way of the knee. One might expect that older patients are more likely to try nonoperative treatment first and wait longer before undergoing surgery. This is an argument supported by the data presented in Table 4. In addition to this, previous data from Norway 5 have estimated that at least 50% of patients with ACL injuries are treated nonoperatively. On the other hand, it is also likely that as time goes by, the chance of having surgery increases if you sustain further injuries to the knee. Then again, surgeons do have different practice profiles. Some are in favor of early surgery, some are leaning toward surgery after a thorough rehabilitation period, and some are somewhere between these 2 practice profiles. The consequence of one, some, or all these aspects is that we might overestimate the importance of time as a risk factor for developing degenerative lesions. The registration of preoperative KOOS data might to some degree counterbalance these limitations. One could argue that trying to formalize and register the patients' reasons for delaying or undergoing reconstructive surgery would be a more desirable approach. The NKLR's steering committee is currently reviewing this issue.
There are 2 other important variables that might bias the results; unfortunately, they are not yet part of the NKLR's registration form. These are the patient's weight and activity level. Either one of these factors is considered to increase the incidence of cartilage lesions and/or meniscal tears.6,12,15 Both factors are under consideration by the NKLR's steering committee for inclusion in both the preoperative and postoperative patient assessments.
There are different opinions on whether reconstructive surgery will result in fewer degenerative changes in the ACL-deficient knee in the long run compared with nonoperative treatment. A recent article by Drogset et al 3 suggested that early surgical intervention would be beneficial because the knees at an early stage had far less cartilage damage than did knees with late surgery. Our results confirm this. A recent study 2 based on review of 183 cases concluded that primary ACL reconstruction surgery should be carried out within 12 months of injury to minimize the risk of meniscal tears and degenerative changes. In this study, presence and type of meniscal tear and type of degenerative change were recorded. The incidence of meniscal tears and degenerative change was assessed and related to the timing from injury to surgery. The patients were divided into an early group (surgery within 12 months of injury) and a late group (surgery more than 12 months from injury). Incidence of meniscal tears was significantly higher in patients undergoing reconstruction late compared with those in the early group (71% vs 42%).
Six percent of the patients with ACL injuries had additional ligament injuries. The presence of these additional injuries might be owing to more severe trauma or more instability and as such explain the reason for these patients receiving surgery 1 year earlier than did those without other ligament injuries. Whereas Beynnon et al 1 found that ACL injuries are more prevalent among female athletes than male athletes, more ACL reconstructions are performed on male athletes because more males participate in at-risk sports, such as team handball and soccer.
Regarding the children's age group, the distribution in time from injury to surgery in relation to type of meniscal tear and ICRS grading does reflect relatively fewer findings (data not shown) in the children who received surgery in the latter end of the time scale. This probably reflects 2 tendencies among Norwegian orthopaedic surgeons. First, the most severely injured knees are operated on fairly soon. And second, in Norway, ACL reconstruction in children seldom occurs before the age of 14 years. This leads to a long time period between injury and stabilizing surgery for children with an early ACL tear. The protocol for these children consists of activity modification and use of a brace when performing knee-demanding activities. These data indicate that this approach does not lead to high incidence of meniscal tears and/or cartilage lesions. 13
The change in odds for a single patient who chooses to have late surgery, the accumulated odds of 1 specific patient at a given time, and the difference in odds between 2 patients may be calculated using the coefficient of regression presented in Tables 2 and 3. This is illustrated in the following 2 examples (described in more detail in the appendix, available online at http://ajs.sagepub.com/supplemental/): a 34-year-old patient with previous surgery to the index knee has an additional ligament injury and a meniscal tear. The increase in odds for having a cartilage lesion for a 2-year difference in the timing of surgery is 1.2. This illustrates that the statistical risk for cartilage lesions increases by 20% for a 2-year difference in the timing of surgery for patients belonging to the patient group of young adults with the same risk profile as presented in this example. This example only calculates the additional increased odds for having cartilage lesions if surgery is 2 years later and does not include the increased risk at time zero (ie, previous surgery to the index knee, additional ligament injury, and a meniscal tear giving a baseline odds of 1.3).
Another example illustrates the difference in odds between 2 patients. Patient A is a 17-year-old male with no previous surgery to the index knee, no additional ligament injuries, and no damaged menisci. Patient B is twice as old (34 years), is the same sex, has previous surgery to the index knee, and has an additional ligament injury and a meniscal tear. These risk profiles will give patient B a 10.6 times increased odds for having cartilage lesions in relation to patient A, which gives an increased odds of 960%, based on the logistic regression model.
On the basis of our results on adults, early surgery may be recommended. However, it is important to remember that many surgeons consider these patients to benefit from preoperative rehabilitation8,16 and that some patients may do well without surgery if they do not participate in high-risk activities.1,11 If sufficient improvement is not achieved within reasonable time, surgery should be considered. A reasonable cutoff can be calculated for each patient based on Tables 2 and 3.
Church and Keating 2 specifically attempted to relate the development of degenerative changes in the knee to the timing of primary reconstruction surgery of the ACL. Our findings do concur with their main conclusions. To extend their findings, we have tried to provide both the physicians and the physical therapists with a new and more individualized tool to help in the decision making.
In conclusion, the odds for a cartilage lesion in the adult knee increased by nearly 1% for each month that elapsed from the injury date until the surgery date, and the presence of cartilage lesions was associated with a nearly 2-fold increase in the risk of having meniscal tears, and vice versa, independent of patient age. Our data suggest that early surgery is associated with fewer meniscal tears and cartilage injuries.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.