
Abstract
Background: Severe glenoid bone loss in recurrent anterior glenohumeral instability is rare and difficult to treat.
Purpose: The authors present a surgical technique using allogeneic bone grafting for open anatomic glenoid reconstruction in addition to the capsular shift procedure.
Study Design: Case series; Level of evidence, 4.
Methods: Nine consecutive patients with a history of recurrent anterior shoulder instability underwent reconstruction of large bony glenoid erosion with a femoral head allograft combined with an anteroinferior capsular shift procedure. Preoperative computed tomographic and arthroscopic evaluation was performed to confirm a ≥120° osseous defect of the anteroinferior quadrant of the glenoid cavity, which had an “inverted-pear” appearance. Patients were followed for at least 4.5 years (range, 4.5-14). Serial postoperative radiographs were evaluated. Functional outcomes were assessed using Rowe scores.
Results: All grafts showed bony union within 6 months after surgery. The mean Rowe score improved to 84 from a preoperative score of 24. The mean loss of external rotation was 7° compared with the normal shoulder. One subluxation and 1 dislocation occurred after grand mal seizures during follow-up. These 2 patients regained shoulder stability after closed reduction. The remaining patients did not report recurrent instability. All patients resumed daily activities without restricted motion.
Conclusion: This technique for open reconstruction is viable for the treatment of recurrent anterior glenohumeral instability with large bony glenoid erosion.
As surgical techniques and implant design have advanced in recent years, high success rates have been reported for the repair of soft tissue Bankart lesions, whether performed by open surgery or arthroscopically.3,6,7,10,15 Reported osseous defect rates of the anterior glenoid rim have ranged from 5% to more than 70%.25,26,32 These rates seem to vary according to imaging and quantification technique. The defects are associated with poor arthroscopic stabilization outcome without bone graft for significant bony loss of the anterior glenoid.4,6,16,26,31
Several biomechanical studies have shown that large bony glenoid defects destroy the contour of the glenoid cavity, which is important in shoulder stability.8,17,18,20 Bigliani et al 4 performed coracoid transfer for bony defects of more than 25% of the glenoid surface. Similarly, Itoi et al13, 14 concluded that osseous defects wider than 21% of the glenoid length caused shoulder instability and limited range of motion after Bankart lesion repair; bone grafting was strongly suggested.
Open repair procedures related to operative treatment of anterior shoulder instability with major bony glenoid defects, such as the Latarjet, Trillat, Bristow, and other modified procedures, have been documented.1,9,11,12,22,27,30 However, they do involve risk of complications such as advanced arthritis, motion loss, broken screws, and nonunion or resorption of the bone graft. 35 These approaches not only ruin the normal coracoid process, scar the subscapularis, and alter the normal positions of the conjoined tendon origins, but also result in nonanatomic reconstruction of the depth and congruency of the glenoid cavity.
In this article, we present our clinical experience with 9 cases of intra-articular reconstruction of large bony erosion or defect of the glenoid rim with allogeneic bone grafting for recurrent anterior shoulder dislocation, and reveal the importance of anatomic restoration of glenoid depth and congruency.
Materials and Methods
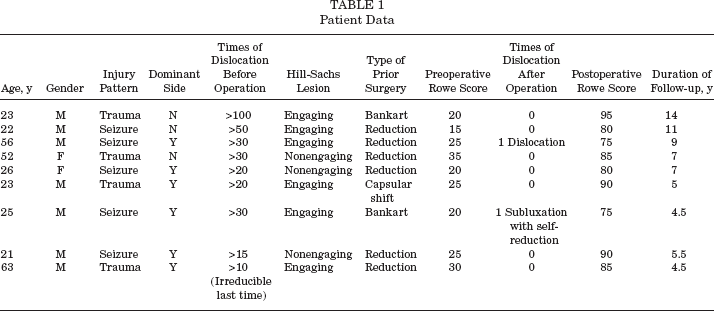
This prospective study followed 9 consecutive patients with recurrent anterior shoulder dislocation following an initial trauma who underwent surgery at our institution between 1993 and 2003. Initial injuries occurred at least 6 months before surgery. All patients gave informed consent. All procedures were performed by the same senior surgeon (C.-H.L.) at the same institute. The study population consisted of 7 men and 2 women with a mean age of 34.6 years (range, 21–63). Six dominant shoulders were affected. Five injuries were epilepsy-related. Three of the 9 patients had undergone prior surgeries (Table 1).
Patient Data
Diagnoses were made by means of history, physical examination, and imaging studies. All cases showed a positive anterior apprehension sign and normal rotator cuff function, and no cases of neurovascular deficit were observed. In addition to plain preoperative radiography, including true AP glenoid views, axillary lateral views, Stryker notch views, and West Point views, all patients underwent CT for suspected bone loss of the anterior glenoid rim (Figure 1). The bony defect measured at least 120° of the glenoid rim, and the glenoid was characterized as having an “inverted-pear” arthroscopic appearance, indicating significant bone loss of the anteroinferior glenoid rim in the normally pear-shaped glenoid cavity.6, 19

A CT arthrogram showing significant bony deficiency of the anteroinferior glenoid rim.
Arthroscopic Evaluation
The patient was placed in the beach-chair position with the table head elevated 30° to 45° and a sandbag wedged under the spine at the medial end of the scapula to allow free movement of the affected arm and complete exposure of the anterior aspect of the shoulder joint. Examination under anesthesia for anterior instability of the affected shoulder was performed before diagnostic arthroscopy. A 4-mm arthroscope was introduced through a standard posterior portal, which confirmed the ≥120° osseous defect of the anteroinferior quadrant of the glenoid cavity, with its “inverted-pear” appearance.
Surgical Technique
Using a deltopectoral approach, the surgeon identified the cephalic vein and retracted it laterally with the deltoid muscle. The subscapularis tendon and conjoined tendon were exposed, and the conjoined tendon was retracted medially. The subscapularis tendon was carefully stripped off the underlying capsule from approximately 1 cm medial to the bicipital groove, and retention sutures were placed in the tendon. The subscapularis was then retracted, and an oblique incision was made with splitting down the capsule along the humeral head cartilage margin from the level of the rotator interval region. A ring retractor was used to help retract the humeral head laterally. Another blunt, curved retractor was inserted onto the glenoid neck to expose the anterior glenoid rim. The size and shape of the bony defect could be visualized directly, and prepared by cleaning away fibrous tissue to make a solid, decorticated surface. The size of the defect was measured as compared with the radius and curvature of the residual glenoid; the bone grafting was also based on this measurement.
An allograft from a femoral head was used to reconstruct the glenoid rim. After the cartilage of the femoral head surface was removed, a quarter-graft of the femoral head was obtained for contouring with a small saw and bur (Figure 2). The graft was solidly fixed with 2 AO 3.5-mm cortical screws; the glenoid surface was curved using the bur along the remaining curvature, and the glenoid surface was designed slightly wider than anatomically normal to prevent engagement of a large Hill-Sachs lesion, if found under arthroscopy. As the graft was contoured to match the desired dimensions for a nearly anatomic anterior glenoid rim with good fixation, 2 or 3 FASTak suture anchors (Arthrex, Naples, Florida) were used to reattach the capsule to the edge of the graft (Figure 3). To eliminate excess capsular volume, a horizontal incision for the middle capsule of glenoid side was performed to create a T-plasty incision of the capsule. The inferior capsule flap of the glenoid side is shifted superolaterally to the humeral side, and the superior flap of the glenoid side is moved over the inferior flap in an inferolateral direction to the humeral side. The transverse portion of the capsulotomy is then closed. The subscapularis tendon was reattached to its insertion anatomically with the arm at 30° of abduction and external rotation.

A quarter-allograft was obtained from the femoral head.
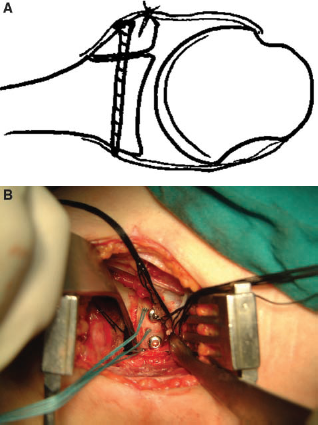
The allograft is shaped to extend the glenoid surface contour and is fixed in place with 2 AO 3.5-mm cortical screws. The capsule is then reattached to the edge of the allograft using 2 or 3 suture anchors. A, drawing; B, operative photograph.
Postoperative Rehabilitation and Assessment
After the surgical procedure was complete, the arm was immobilized in a sling and swathed while the patient recovered from general anesthesia. The shoulder was maintained in an abduction sling for the first postoperative week, after which the sling was removed. During the next 2 weeks, forward flexion was limited to 90°, external rotation was limited to neutral, and pendulum exercises were performed. From the fourth week, all patients were encouraged to resume active range of motion, strength training, and progress toward daily activities.
True AP glenoid views were obtained immediately after, 6 weeks after, and 3 months after surgery to evaluate the fixation of screws and suture anchors and follow the progression of bone healing. For objective evaluation, the postoperative range of motion in the affected and unaffected shoulders was measured with a goniometer, for internal and external rotations in the supine position and forward flexion when standing. Comprehensive evaluation of shoulder stability, range of motion, and functioning were performed before and after surgery using the Bankart rating scale of Rowe. Results were graded as excellent (score >90 points), good (75–89), fair (51–74), or poor (<50 points). 26 Patients were followed for at least 4.5 years (range, 4.5–14 years; mean, 7.5). Findings of all postoperative evaluations were noted by a single observer.
Statistical analysis was carried out using the Wilcoxon signed-rank test (P = .05).
Results
All nine patients were evaluated clinically by means of the Rowe score (Table 1). 26 The postoperative score averaged 84 (range, 75–90), compared with a mean preoperative score of 24 (range, 15–35). This difference was statistically significant (P < .001). Results were graded as excellent in 3 patients and good in 6.
At the last follow-up after surgery, anterior apprehension and relocation tests were conducted. These tests were negative in all patients, and none complained of instability. At 15 and 21 months after surgery, among the patients with epilepsy, 1 experienced shoulder dislocation and another experienced subluxation after grand mal seizures. The subluxated shoulder underwent self-reduction after the seizure episode, and the dislocated shoulder underwent closed reduction with minimal traction under general anesthesia. Under good control for the epilepsy and with rehabilitation, no recurrence was noted for 8 years for this dislocated shoulder and for 3 years for the subluxated one. The other 7 patients had no incidence of dislocation after surgery. All 9 patients resumed their daily activities without restricted motion. Operated shoulders had a mean loss of external rotation of 7° (range, 5°–12°) compared with the nonoperated shoulders.
Preoperative CT showed that each patient had a Hill-Sachs lesion on the humeral head, which was confirmed at arthroscopy. Follow-up radiography showed no signs of significant resorption, screw migration, or screw breakage in any of the 9 grafts. Bony union was demonstrated for all grafts within 6 months after surgery (Figure 4). All patients had painless, stable shoulders, and reported that postoperative loss of external rotation did not affect their quality of life.
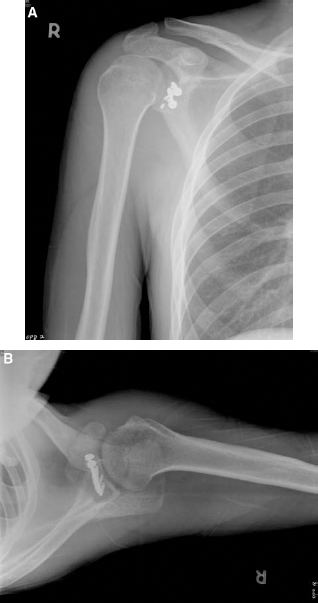
Follow-up AP (A) and axial (B) radiographs, taken 6 months after surgery, showing the position of the two 3.5-mm cortical screws and 3 suture anchors. Anatomic restoration of the glenoid contour is shown on an axial view.
Discussion
Bigliani et al 4 recommended coracoid transfer for rim defect lesions that exceed 25% of the glenoid surface. According to the cadaver study by Itoi et al, 14 an osseous defect wider than 21% of the glenoid length may cause instability and limit the shoulder's range of motion after simple capsular repair. They also measured the size of anteroinferior bony Bankart lesions by CT and emphasized the need for bone grafting. 12 Burkhart and DeBeer 6 analyzed the results of 194 arthroscopic Bankart repairs, identifying significant bony defects as having an inverted-pear appearance and concluding that they were not candidates for arthroscopic Bankart repair. The glenoid cavity plays 2 major roles in the containment of the humeral head. One is its “deepening effect,” through which it resists shear forces to avoid anterior dislocation. The other role is through the effect of glenoid arc length, which allows the glenoid cavity to resist axial forces at various angles from the humerus. 6 In addition, several biomechanical studies have established the importance of the buttressing effect of the anteroinferior glenoid rim.8,17,18,20 This indicates the need for anatomic bone reconstruction in cases of large defects of the anterior glenoid rim. Lai et al 16 and Rhee and Lim 24 found that Bankart lesion size is an important factor in surgical outcome after Bankart repair with simple capsular reattachment. Regardless of this technique being arthroscopic or open, they concluded that poor surgical outcomes would follow from large bony Bankart lesions. Sugaya et al 31 used reconstructed 3-dimensional CT to quantify the percentage of bone loss of the glenoid cavity area and confirm the existence of an osseous fragment at the anteroinferior glenoid. Bone loss of more than 25% was found in 23 of 42 glenoid cavities. They reported successful outcomes for arthroscopic osseous Bankart repair for chronic, large glenoid defects in these 42 patients. Porcellini et al 23 also reported good results for the arthroscopic technique using suture anchors for fixation of the avulsed bone fragment to the healthy glenoid rim of isolated acute bony Bankart lesions involving slightly less than 25% of the glenoid cavity. However, despite these reports of success, arthroscopic osseous Bankart repair techniques still use the original avulsed osseous fragment and are based on the concept of restoration of glenoid shape.
In a 2-part anatomic study including live subjects and cadavers, Lo et al 19 reported that the inverted-pear glenoid appearance represents significant bone loss of at least 25% to 27% of the inferior glenoid width. Although some recent studies have reported that CT or reconstructed 3-dimensional CT images can be used to estimate glenoid osseous defects, which is valuable for determining appropriate surgical procedures, we adapted arthroscopic evaluation for identification of the inverted-pear appearance of the glenoid cavity before open surgery.13, 31 We also used it for confirmation of glenoid defect size. Arthroscopy can also determine the presence of an engaging Hill-Sachs lesion and provide treatment for labral or chondral lesions, which could affect postoperative results. Because of its minimal invasiveness and advanced techniques, arthroscopic evaluation is still beneficial and reasonable; CT images do not have these advantages.
Recurrent Bankart lesions often coexist with an engaging Hill-Sachs lesion with an articular-arc deficit. Burkhart and DeBeer 6 suggested that surgeons must not only repair the Bankart lesion but also perform an open capsular shift procedure to adequately restrict external rotation and prevent the Hill-Sachs lesion from engaging the anterior glenoid cavity. Compared with arthroscopic capsular plication or thermal capsulorrhaphy, the required extent of restricted external rotation is unpredictable.
The most common postoperative complications after open treatment of shoulder instability are limited range of motion, recurrent instability, and glenohumeral degenerative change.21, 33 In this series, no recurrent apprehension was observed and no evidence of pullout of suture anchors or degenerative change was noted from radiography.
In the present study, we used 2 separate fixation methods for the graft and capsule. One involved AO 3.5-mm screws for fixation of the graft to the glenoid cavity near the glenoid neck, and the other involved FASTak suture anchors (Arthrex) for fixation of the capsule and graft on the reconstructed rim. Simple fixation of the avulsed fragment with cannulated screws has been associated with a higher rate of early anterior shoulder pain due to screw impingement. 28 We placed the suture anchors under the joint line of the rim to prevent implant impingement and reduce the rate of postoperative anterior shoulder pain, which could adversely affect the rehabilitation program and the ultimate surgical results.
Serial radiographs taken during follow-up showed all allografts to be in place, with good bony union. Allografts avoid potential complications involving autografts at the donor site. Because the femoral head is bulky enough to shape the anteroinferior glenoid rim, the problem of the limited size of the iliac crest is avoided when autografts are used. Even if the graft is made somewhat wider than the lost glenoid surface, combination with the appropriate capsule plication in an open procedure provides more external rotation and shoulder stability.
In our series, 5 of the 9 patients were epileptic. Regarding postoperative shoulder dislocation after grand mal seizure, we discussed humeral head grafting with patients after review of the preoperative evaluation of a large and engaged Hill-Sachs lesion. However, patients were satisfied with the present condition and had no desire for additional surgery. Postoperative Rowe scores for the 2 patients with recurrence were relatively low. The most common type of shoulder instability as a complication of epileptic seizure is posterior dislocation. 29 In a study by Buhler and Gerber 5 with a mean follow-up time of 10 years, 34 shoulders in 26 patients had initial dislocation after epileptic seizure, and 17 shoulders in 13 patients were treated for anterior dislocation. The recurrence rate after initial repair of anterior dislocation was much higher than for posterior dislocation (47% vs 12%), and large bony Hill-Sachs lesion defects and glenoid rim loss were the trademarks of shoulder instability after epilepsy, which had a relatively high rate of recurrence. The authors suggested that skeletal reconstruction was needed to achieve clinical stability, especially for the more difficult treatment of anterior dislocation. They also noted that good compliance with a regimen of anticonvulsive medication was important in this patient population.
In line with a similar concept in a recent study by Auffarth at al, 2 47 shoulders with glenoid rim fractures after recurrent anterior dislocation were stabilized by anatomic glenoid reconstruction with an iliac crest, bicortical J-shaped autograft. Encouraging long-term results in terms of clinical outcome and radiologic assessment were reported, although mild to moderate arthropathy developed in some patients. Compared with another biomechanical study, stability testing of 8 cadaveric shoulders was carried out in a dynamic shoulder simulator by Wellmann et al. 34 They found that the Latarjet procedure outperformed the structural intra-articular bone graft in reducing translation with significant anteroinferior glenoid bone defects. However, they did not perform the capsular shift procedure for intra-articular bone grafting and were unable to evaluate the practical effects of the additional stability of healed capsulorrhaphy. This biomechanical comparison cannot estimate the clinically consecutive complications of the Latarjet procedure, such as laceration and scarring of the subscapularis tendon, along with shoulder joint arthrosis stemming from impingement of the transferred coracoid segment.
There are some limitations to the current study. Although a high union rate and good stability for allogeneic bone grafting intra-articularly have been shown as midterm outcomes, long-term effects are yet unknown. The long-term outcome could include degenerative diseases of the glenohumeral joint, resulting from possible intra-articular graft impingement of the humeral head. It may suppress bony union for extra-articular bone grafts. Also, our patients were not involved in athletics. The suitability of these procedures for athletes needs more investigation. Clinical evaluation of the Rowe rating system does not cover a specific assessment of shoulder pain, and is also not sensitive to loss of external rotation. We recorded the external rotation additionally at postoperative follow-up and compared it with the unaffected side.
Conclusion
Anatomic open reconstruction with allogeneic femoral head bone grafting can increase glenoid curvature in cases of significant bone loss. Combination of this procedure with subsequent capsular shift can further increase shoulder stability, even with an engaging Hill-Sachs lesion. Although chronic recurrent anterior glenohumeral instability is a challenging condition, it can be a viable alternative if it follows the practical steps laid out in this article.