
Abstract
Background: There is limited information regarding directly measured load responses of the posterior oblique and superficial medial collateral ligaments in isolated and multiple medial knee ligament injury states.
Hypotheses: Tensile load responses from both the superficial medial collateral ligament and the posterior oblique ligament would be measurable and reproducible, and the native load-sharing relationships between these ligaments would be altered after sectioning of medial knee structures.
Study Design: Descriptive laboratory study.
Methods: Twenty-four nonpaired, fresh-frozen adult cadaveric knees were distributed into 3 sequential sectioning sequences. Buckle transducers were applied to the posterior oblique ligament and the proximal and distal divisions of the superficial medial collateral ligament; 10 N·m valgus moments and 5 N·m internal and external rotation torques were applied at 0°, 20°, 30°, 60°, and 90° of knee flexion.
Results: With an applied valgus and external rotation moment, there was a significant load increase on the posterior oblique ligament compared with the intact state after sectioning all other medial knee structures. With an applied external rotation torque, there was a significant load decrease on the proximal division of the superficial medial collateral ligament from the intact state after sectioning all other medial knee structures. With an applied external rotation torque, the distal division of the superficial medial collateral ligament experienced a significant load increase from the intact state after sectioning the posterior oblique ligament and the meniscofemoral division of the deep medial collateral ligament.
Conclusion: This study found alterations in the native load-sharing relationships of the medial knee structures after injury. Sectioning both the primary and secondary restraints to valgus and internal/external rotation of the knee alters the intricate load-sharing relationships that exist between the medial knee structures.
Clinical Significance: In cases in which surgical repair or reconstruction is indicated, consideration should be placed on repairing or reconstructing all injured medial knee structures to restore the native load-sharing relationships among these medial knee structures.
Keywords
Injuries to the medial knee structures, often inaccurately referred to as injuries to the medial collateral ligament (MCL), are the most common knee ligament injuries. § A complete understanding of medial knee biomechanics is necessary to assess which structures are to be given consideration when performing a repair or reconstruction. There are a number of quantitative biomechanical studies that have increased the knowledge of medial knee structure function. ‖ Previous sequential sectioning studies have provided information regarding either the amount of increased motion or the decreased external applied force required to produce abnormal motion in ligament-deficient knees. ¶ However, both of these study designs are indirect measures of the compensatory load-sharing characteristics of the individual medial knee structures in injury states and do not provide individualized information for each individual ligament or its relationship to associated ligaments during injury.
References 5, 7, 11, 12, 14, 21, 23, 26.
References 2, 3, 22, 27, 29, 32, 35, 36.
References 1, 4, 9, 10, 13, 24, 25, 28, 30, 31, 33.
Because of the indirect measurement methods used in these previous studies, a complete understanding of the complex interaction of the medial knee structures has not been fully attained. Our previous study directly measured the tensile forces on the intact medial knee structures for this same group of knees during external force application. 6 Directly measuring the compensatory loads in medial knee structures in an injury state would provide insight into the clinical importance of repairing or reconstructing medial knee structures and understanding of the cause of graft failure in combined injury patterns.
The purpose of this study was to comprehensively examine the abnormal motion and load redistribution associated with injury to medial knee structures. In part 1 of this study, we quantified the roles that the posterior oblique ligament (POL), the proximal and distal divisions of the superficial MCL (sMCL), and the meniscofemoral and meniscotibial divisions of the deep MCL (dMCL) have in providing primary and secondary stabilization roles to valgus, external rotation, and internal rotation for the medial knee after sequential sectioning of medial knee structures. In part 2 of this study (this article), our purpose was to examine the compensatory load-sharing characteristics of the POL and the 2 divisions of the sMCL after sequential sectioning of the POL, the proximal and distal divisions of the sMCL, and the meniscofemoral and meniscotibial divisions of the dMCL. Our hypothesis was that tensile load responses from both the sMCL and the POL would be individually measurable and that the native load-sharing relationships between these ligaments would be altered after sectioning of medial knee structures.
Materials and Methods
Specimen Preparation
Twenty-four nonpaired, fresh-frozen cadaveric knees with no evidence of prior injury with a mean age of 69.5 years (range, 45–87 years) were used for parts 1 and 2. The femur was potted in polymethylmethacrylate 20 cm proximal to the knee joint, and the tibia was sectioned 12.5 cm distal to the knee joint. A threaded rod was inserted into the tibial intramedullary cavity, parallel with the long axis of the tibia, and fixed in position with polymethylmethacrylate. A hexagonal lock nut was attached to the tibial rod to allow for application of external loads.
The knee-testing apparatus firmly secured the femur at a horizontal angle, while allowing uninhibited movement of the tibia at the measured knee flexion angles. After the knee was aligned in the testing apparatus, buckle transducers were securely fastened to the POL, the proximal division of the sMCL, and the distal division of the sMCL (Figure 1).
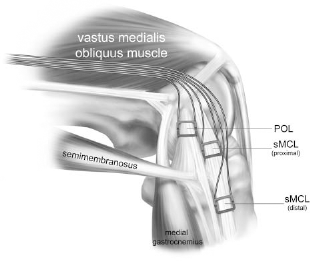
Buckle transducer placement on the posterior oblique ligament (POL) and the proximal and distal superficial medial collateral ligament (sMCL) divisions. The sMCL buckles were placed proximal to their respective attachment sites (medial view, left knee). Reprinted with permission from Griffith CJ, Wijdicks CA, LaPrade R F, et al. Force measurements on the posterior oblique ligament and superficial medial collateral ligament proximal and distal divisions to applied loads. Am J Sports Med. 2009;37:140–148; Figure 2.
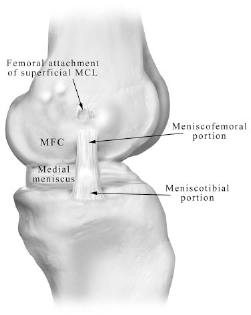
The meniscofemoral and meniscotibial portions of the deep medial collateral ligament (medial aspect, left knee) with the posterior oblique ligament and remaining medial capsule removed. MFC, posterior aspect of medial femoral condyle.
Observed Ligament Load via Buckle Transducers
The buckle transducers consisted of a crossbar and a rectangular frame containing semiconductor strain gauges. The use of these devices has been previously described in detail.6,16,17,19,20 Surrounding bone or soft tissue impingement of the buckle frames and undesirable ligament damage during biomechanical testing were minimized by using crossbars of assorted depths. 19 Buckle transducer application consisted of placing the frame over the ligament of interest and inserting the crossbar both below the ligament and above the frame. Therefore, ligament tension, caused by loading of the specific ligament, pushed the crossbar against the frame, similar to 3-point bending. Deformation of the buckle frame induced a voltage response in the strain gauge contained within the buckle frame. Finally, this voltage output was relayed to a data acquisition system. Prior work has reported that there is a linear relationship between applied load and voltage output. 20 Therefore, the voltage outputs were converted to kilonewtons according to a conversion factor determined by posttest calibration of each buckle with a known load. Buckles were zeroed before each external load application to ensure accurate load measurements. Buckle transducers have been reported to be repeatable to within 0.7% using a similar biomechanical testing protocol. 19
External Force Application
Each knee was tested at 0°, 20°, 30°, 60°, and 90° of knee flexion. Knees were randomly assigned to 3 sequential sectioning sequences with a total of 8 knees per sequence (Table 1). The sequences involved sectioning of the POL, the proximal and distal divisions of the sMCL, and the meniscofemoral and meniscotibial divisions of the dMCL (Figure 2). A 100-N force model SM S-type load cell (Interface, Scottsdale, Arizona; manufacturer reported nonrepeatability error of ±0.01%) was used to apply a 10-N·m valgus moment on the tibial rod 22.9 cm distal to the joint line; 5-N·m external and internal rotation torques were applied to the lock nut on the tibial rod with a 15-N·m capacity model TS12 shaft style reaction torque transducer (Interface, manufacturer reported nonrepeatability error of ±0.02%). Varus moments were not applied to the knee because pilot testing of 3 specimens revealed no load responses from these structures during the application of a 10-N·m varus moment. Before experimental testing, the load cell and torque transducer were calibrated to establish a linear relationship between voltage output and force application. For each sequential sectioning series and flexion angle, external loads were applied to the specimen 3 times and the results averaged.
Sequential Sectioning Groups of Medial Knee Structures for 3 Groups of 8 Knees for Biomechanical Testing a
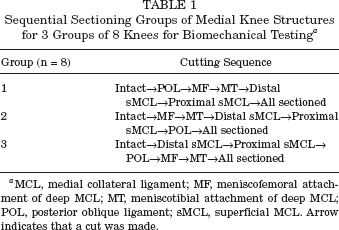
MCL, medial collateral ligament; MF, meniscofemoral attachment of deep MCL; MT, meniscotibial attachment of deep MCL; POL, posterior oblique ligament; sMCL, superficial MCL. Arrow indicates that a cut was made.
Data Analysis
Ligament tensile forces during testing were determined by calibrating the measured buckle voltages against a standardized load. After sectioning of a ligament, the buckle of interest was calibrated by directly tensioning the ligament using a load cell according to a previously described method.6, 20
Voltage measurements during biomechanical testing were simultaneously collected from the buckle transducers and the previously described torque transducer or load cell. When the external force applied to the structure equaled the target force, the correlating buckle voltage outputs were converted to force measurements according to the previously defined linear regression outlined above. These force measurements were indicative of the tensile load response in the ligament of interest.
Statistical Analysis
A 2-way analysis of variance was used to compare each particular ligament's load response to valgus loads and internal and external rotation torques for each particular flexion angle between sectioned states. Tukey's honestly significant difference was used for post hoc comparisons to detect significant differences between particular pairs of the load responses considered in each analysis of variance. A significant difference was determined to be present for P < .05.
Results
Force on the POL
Compared with the intact state, there was a significant load increase to an applied valgus moment on the POL after sectioning the proximal and distal divisions of the sMCL and the meniscofemoral and meniscotibial divisions of the dMCL at 0° (14.9 vs 24.3 N), 20° (12.0 vs 28.3 N), and 30° (12.0 vs 26.4 N) of knee flexion (P < .05) (Figure 3). There was also a significant increase in load on the POL with an applied external rotation torque after sectioning both divisions of the sMCL and the dMCL at 60° (11.7 vs 13.0 N, P < .05) of knee flexion.
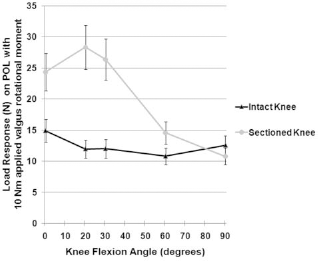
Forces measured on the posterior oblique ligament (POL) during application of a 10-N·m valgus load comparing the intact state to the sectioned knee (all of the structures except for the POL). Error bars indicate the standard error of the mean.
Forces on the Proximal Division of the sMCL
Compared with the intact state, there was a significant load decrease to an applied external rotation torque on the proximal division of the sMCL after sectioning the POL, meniscofemoral and meniscotibial divisions of the dMCL, and distal division of the sMCL at 30° (48.6 vs 19.0 N, P < .05) and 90° of knee flexion (54.3 vs 15.9 N, P < .05) (Figure 4).
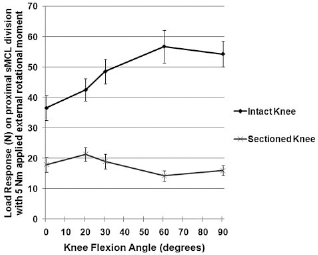
Forces measured on the proximal superficial medial collateral ligament (sMCL) division during application of a 5-N·m external rotation torque comparing the intact state to the sectioned posterior oblique ligament, deep MCL, and distal division of the sMCL. Error bars indicate the standard error of the mean.
Force on the Distal Division of the sMCL
Compared with the intact state, there was a significant load increase to an applied valgus load on the distal division of the sMCL after sectioning of the meniscofemoral division of the dMCL at 90° of knee flexion (75.4 vs 78 N, P < .05). With an applied external rotation load, there was a significant load increase seen on the distal division of the sMCL at 0° and 20° of knee flexion after sectioning the POL and the meniscofemoral division of the dMCL (P < .05) (Figure 5). With an applied internal rotation load, there was a significant load increase after sectioning the POL and meniscofemoral and meniscotibial divisions of the dMCL at 20° of knee flexion seen on the distal division of the sMCL from the intact state (25.6 vs 38.8 N, P < .05).
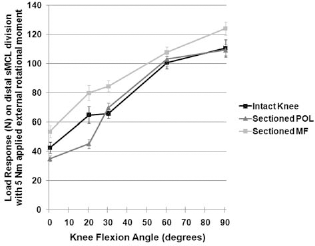
Forces measured on the distal superficial medial collateral ligament (sMCL) division during application of a 5-N·m external rotation torque comparing the intact state to the sectioned posterior oblique ligament (POL) and subsequent meniscofemoral (MF) division of the deep MCL. Error bars indicate the standard error of the mean.
Discussion
Our unique experimental setup allowed us to directly measure the changes in tensile force experienced by ligaments in an injury state. This information is useful because it identifies alterations in the native load-sharing relationships of medial knee structures after injury. Furthermore, our multiple sectioning sequences allowed us to demonstrate the effects resulting from injury to secondary stabilizers when the primary stabilizers were intact. Our previous study directly measured and reported on the tensile loads experienced by the POL and the 2 divisions of the sMCL in the intact knee on the same knees as this study. 6 This previous study quantitatively reported on the distinct importance of the distal division of the sMCL in response to valgus moments and the previously underestimated function of the POL in resisting internal rotation torques at knee flexion angles close to extension. 6
The anatomy of the sMCL is well described in the literature.3,15,18,34 It has an attachment to the femur proximoposterior to the medial epicondyle,15, 25 a proximal tibial attachment on the soft tissue medial to the anterior arm of the semimembranosus,3, 15 and a distal tibial bony attachment anterior to the posteromedial crest of the tibia.15, 25 These 3 attachment sites divide the functional anatomy of the sMCL into a proximal and a distal division.
Although the proximal tibial attachment is a readily identifiable structure, this primarily soft tissue attachment is not as static as either the femoral or distal tibial attachments, which attach directly to bone. Furthermore, it has been noted that the more superficial, or medial, fibers of the sMCL do not attach to the proximal tibial attachment. The distal division of the sMCL was reported to be a primary knee stabilizer to external rotation in part 1 of this 2-part study. The difference in attachment site fixation could be an explanation for the significant decrease in external rotation load response that we observed in the proximal sMCL division at 30° after sectioning of the other medial knee structures. We theorize that as a result of the primarily soft tissue attachment on the proximal tibia, the proximal division of the sMCL was not statically tethered, resulting in the significantly decreased load response to external rotation. In addition, we theorize that the more medial sMCL fibers, which do not attach directly to its proximal tibial attachment, become less taut during external rotation loads, resulting in the decrease in force seen on the proximal division of the sMCL. Subsequently, the increased load not absorbed by the proximal division of the sMCL was likely diverted to a structure not measured in this study, such as the dMCL or the cruciate ligaments.
With regard to the forces seen on the POL, we found a significant increase in valgus load compared with the intact state after sectioning the components of both the dMCL and sMCL at 0°, 20°, and 30° of knee flexion. This observation correlates both with a previous article that demonstrated that the POL experiences tensile load to valgus forces in intact knees especially close to knee extension 6 and with the previous literature that reported the POL has a secondary stabilization role in valgus stability of the knee.8,28,34 Therefore, it is logical that the POL would demonstrate an increased load response in sMCL- and dMCL-deficient knees.
The limitations of this study include that we were only able to apply buckle transducers to the POL and the proximal and distal divisions of the sMCL. Because of the limitations of buckle transducers, we were not able to apply them to the meniscofemoral and meniscotibial portions of the dMCL because it would create impingement by the sMCL, which would result in inaccurate readings for these structures. In addition, we did not apply buckle transducers to other supporting knee structures and thus were not able to measure which structures took up the additional load seen with specific structure sectioning. We did not anticipate our findings of a decrease in load for the proximal division of the sMCL with external rotation loading with sectioning of other structures. Although we theorize this decrease in measured load on the proximal division was owing to the lack of stability provided by the more medial fibers becoming untethered with external rotation loads due to the distal attachment being sectioned, it was possible that other structures not measured in this study, such as the dMCL, may have taken up this load.
Our results add to part 1 with load information pertaining to an increase in motion after sectioning. Our results demonstrated that medial knee injuries alter the intricate load-sharing relationships that exist between all of the medial knee structures, which, if left untreated, could potentially increase the risk for further injury. Therefore, in cases in which surgical repair or reconstruction is indicated, consideration should be given to repairing or reconstructing all injured medial knee structures to restore the normal load-sharing relationships among these structures at the time of surgical treatment.