
Abstract
Background: Lateral ulnar collateral ligament (LUCL) reconstruction using a tendon graft is a well-accepted procedure used in the treatment of posterolateral rotatory instability. However, unlike most other ligament reconstructions, anatomical guidelines for the isometric points for tunnel placement of LUCL reconstruction have not been defined.
Purpose: To determine if isometric points exist for tunnel placement for LUCL reconstruction and, if so, to determine their anatomical guidelines.
Study Design: Controlled laboratory study.
Methods: A series of 1.8-mm drill holes was placed in potential ligament reconstruction origin and insertion sites in 13 normal cadaveric elbows along the supinator crest of the ulna and in the lateral epicondyle of the humerus. The prepared specimens were mounted in a plastic test frame with electromagnetic sensors inserted into the drill holes. The distance between each potential pair of insertion sites was measured throughout the arc of elbow motion to determine the most isometric combinations of humeral and ulnar insertion sites.
Results: We could not locate truly isometric points for tunnel placement for LUCL reconstruction. For LUCL reconstruction, the position of most isometric tunnel placement was on the supinator crest 16 to 20 mm distal to the proximal margin of the radial head for the proximal wall of the ulnar tunnel, and between the 3:00 and 4:30 o’clock positions on the lateral epicondyle for the posterior/distal wall of the humeral tunnel.
Conclusion: Similar to the native LUCL, there is no truly isometric location for LUCL tendon graft reconstruction tunnels. Also similar to the native LUCL, the distance between the optimal tunnel position decreases in elbow extension and often increases in elbow flexion.
Clinical Relevance: The most isometric position for LUCL reconstruction tunnel placement was defined using anatomical references.
Keywords
Lateral ulnar collateral ligament (LUCL) reconstruction using a tendon graft is a well-accepted procedure used in the treatment of posterolateral rotatory instability (PLRI) of the elbow.5,16–19,23,25 Although the native LUCL classically has been thought to be nearly isometric, with little change in the distance between origin and insertion from 0° to 120° of elbow flexion,3,13,15,21 a recent MRI study has shown that the native LUCL is tighter in flexion than in extension, leading to questions regarding whether it is the primary stabilizer against PLRI. 14 Regardless, tendon graft reconstruction of the LUCL has been reported to have excellent results in the treatment of PLRI.16–19,23,25
Most ligament reconstructions have well-defined anatomical guidelines for tunnel placement, with the isometry of these sites well studied.1,2,6–8,26 However, anatomical guidelines for the isometric points for tunnel placement of LUCL tendon graft reconstructions have not been well defined. Current recommendations are to drill the ulnar tunnels close to the tubercle of the supinator crest, whose exact proximal-distal location is inconsistently described in the literature; the supinator crest extends from a level proximal to the radial head to a level distal to the radial neck (Figure 1). For humeral tunnel placement, the recommendation is to use a suture placed through the ulnar tunnels to determine the isometric point on the lateral epicondyle.9,16–19,23,25 Cohen 4 has noted anatomical references for graft placement based on clinical experience, but without biomechanical verification. He recommended that the humeral tunnel be placed “at the base of the (lateral) epicondyle where the epicondyle flattens onto the lateral aspect of the capitellum.” An accompanying figure in the Cohen article shows that the posterior wall of this tunnel is at the anterior aspect of the lateral epicondyle. He recommends placement of the ulnar tunnel at the proximal margin of the radial head. Moritomo et al 14 recommended anatomical guidelines based on the center of the capitellum. However, this study did not use actual cadaveric specimens and it is difficult to put their recommendations into practice, as the humeral drill holes for LUCL reconstruction are usually placed through the lateral epicondyle, not the flat surface of the lateral condyle.16,17,19,20,23,25
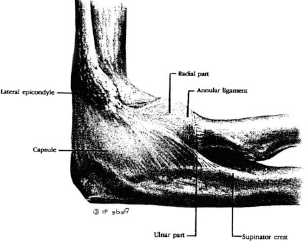
The supinator ridge of the ulna extends from a level proximal to the radial head to a level distal to the radial neck. (Reprinted with permission from O'Driscoll SW, Horii E, Morrey BF, Carmichael SW. Anatomy of the ulnar part of the lateral collateral ligament of the elbow.
The purpose of the present study was to determine if an isometric point exists for tunnel placement for LUCL reconstruction, and to determine the most isometric points for placement of ulnar and lateral epicondylar tunnels for LUCL tendon graft reconstruction using a microBIRD measurement system. The Ascension microBIRD system (Ascension Technology Corporation, Burlington, Vermont) was used to provide minimally invasive measurements of 3-dimensional motion of bones in real time and to provide a method to immediately assess the quality of the measurements.
Materials and Methods
Seventeen unembalmed fresh-frozen, human cadaveric elbows and forearms were examined. Four were found to have excessive laxity, as will be described, and 3 were found to have restricted range of motion; thus, 10 uninjured specimens with a full range of motion were accepted. The mean age of the cadavers was 67 ± 12 years. The specimens were amputated at the level of the humeral midshaft. Muscle attachments were stripped from the proximal 5 cm of the humeral stump, which was potted in PVC pipe. The specimens were completely thawed before being studied. A lateral approach was made to the elbow, reflecting the skin and subcutaneous tissues from the lateral ulna without disturbing the muscles, LUCL, or the joint capsule of the elbow. A small arthrotomy was made anterior to the LUCL to visualize the proximal margin of the radial head and to inspect the joint to ensure that there was no arthritis or other abnormality. Physical examination ensured that there was no clinically significant instability present, which was later confirmed by comparing isometry measurements in supination with measurements in pronation.
A series of 1.8-mm drill holes were placed in potential ligament repair insertion sites in both the humerus and ulna through splits in line with the muscle-fascial fibers; the native ligaments were not disrupted. All holes were oriented orthogonally to the overlying cortex. For the ulna, these were in 4-mm increments linearly along the supinator crest of the ulna, starting 4 mm proximal to the proximal margin of the radial head to a point 32 mm distal to the proximal margin of the radial head. Points were labeled with respect to their distance distal to the proximal margin of the radial head, from −4 to +32. A position of “0” was defined to be at the level of the proximal margin of the radial head. Positive positions were distal to that point and negative positions were proximal to that point (Figure 2).
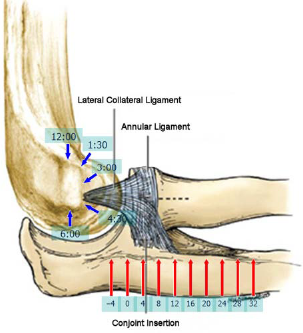
Location of the markers at the origins and insertions of the virtual lateral ulnar collateral ligament tendon graft reconstruction.
For the humerus, defining the most proximal aspect of the lateral epicondyle (ie, toward the humeral shaft) as “12:00 o'clock” and the anterior aspect of the lateral epicondyle as 3:00 o'clock, 1.8-mm drill holes were placed into the lateral epicondyle at the 12:00, 1:30, 3:00, 4:30, and 6:00 o'clock positions (Figure 2). Owing to the size of the sensor and the necessity of having thick enough tunnel walls to prevent breakthrough, this was the maximum number of drill sites that could be reproducibly obtained. To place these drill holes, the anterior half of the lateral epicondyle was exposed using a series of tendon splits, without detachment.
The prepared specimen was mounted in an all-plastic test frame. Electromagnetic sensors (1.8 mm diameter, the microBIRD system) were inserted into the aforementioned drill holes in both the humerus and ulna, flush with the cortex, and maintained in position by a press fit. Each potential pair of insertion sites was tested with the forearm fully supinated and at 0°, 15°, 30°, 45°, 60°, 90°, 120°, and 150° of flexion, and then fully pronated at 15°, 30°, and 45° of flexion, as measured by a goniometer. We tested these flexion angles in pronation because these are the positions of elbow motion where PLRI occurs.13,16,17 To ensure that the LUCL of our specimens did not have subtle laxity, it was necessary to confirm that forearm rotation did not affect the values obtained at angles of elbow flexion where subtle PLRI would manifest itself.
Testing was performed starting with the 12:00 o'clock humeral site, which was tested with each ulnar site for each angle of flexion, and then the 1:30 o'clock humeral site was tested with each ulnar site for each angle of flexion, proceeding distally to test all combinations of humeral and ulnar sites against each other. Using the electromagnetic tracking system, the distance between the humeral and ulnar insertion sites was measured for each potential pair of insertion sites and for each position of the elbow. This provided 550 data points per elbow. For each data point, 10 trials were automatically collected and the results averaged. If the range (maximum minus minimum) of these measurements was more than 0.5 mm, the data point was repeated. A custom program was written to measure the distance between the 2 sensors. The position of each sensor was routinely visually checked to verify that the sensors did not shift during testing.
The microBIRD system provided 6 degree-of-freedom position measurements and a software interface to calculate relative motions from the data. The resolution of this measurement system is 0.5 mm root mean square. Interference in this measurement system caused by metal objects in the field can be detected by erratic behavior of the transducer output. To avoid errors from interference, measurements were only taken when the output was stable. Any position measurement that was not stable during the data acquisition was detected and repeated.
Measurements were taken at 15°, 30°, or 45°, both with the forearm fully pronated and supinated, which represents the range of motion where PLRI is symptomatic. Ninety-five percent of the differences between measurements taken in pronation were less than 3 mm different from corresponding measurements taken with the arm supinated. Therefore, a difference in these measurements of 3 mm or greater was assumed to be due to laxity of the native LUCL and disqualified the specimen from analysis; 4 specimens were excluded after review of the data. The proximal-distal length of the radial head plus neck of each specimen, from where the shaft began to increase its diameter (the metadiaphyseal junction) to the proximal margin, was measured with a caliper 3 times and the results were averaged.
Statistical Analysis
Maximum strains were calculated as the maximum change in distance between candidate tunnel placement points for all positions of elbow flexion studied, divided by the distance between the candidate points at the angle of tensioning. Descriptive statistics and analysis of variance were completed for both the displacement and the strain data.
Results
We could not locate truly isometric points for tunnel placement for LUCL reconstruction. The corresponding sites in the humerus and ulna that displayed the most isometry and the second most isometry are noted in Table 1. The difference between the minimum and maximum distances between the humeral and ulnar points throughout the range of elbow flexion-extension is noted as the maximum displacement.
First and Second Most Isometric Tunnel Combinations for Each Specimen Tested, Along With the Maximum Change in Graft Length (mm) That Would Occur If the Graft Was Placed at the Most Isometric Position
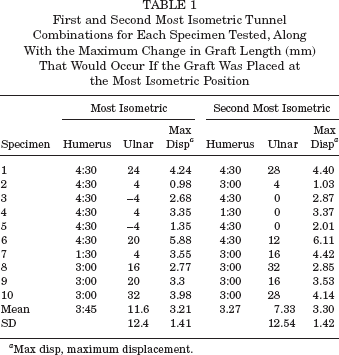
Max disp, maximum displacement.
Analysis of variance indicated that the humeral position (P < .0001) and ulnar position (P = .0015) both had a significant effect on the maximum displacement between potential graft insertion points. The results also varied significantly with the specimen (P < .0001), suggesting that not all specimens would have the same optimal position and that the most isometric point is likely to be patient-specific. Because of this individual variation, the data from different specimens could not be pooled to determine if there was a significant difference between potential insertion points.
The humeral positions of 3:00 or 4:30 o'clock were the most isometric for 9 of the 10 specimens, with 1:30 o'clock being the most isometric position for 1 specimen. The mean most isometric humeral position was 3:45, half-way between the 3:00 and 4:30 o'clock positions. The 3:00 and 4:30 o'clock positions were also second best for 9 of the 10 specimens, with 1:30 o'clock being the second best position for 1 specimen. The mean, second most isometric humeral position, 3:27, was approximately 3:30 o'clock.
The most isometric ulnar position was somewhat more variable, and isometry was not as sensitive to ulnar tunnel placement; that is, there was not a large difference between the results for adjacent ulnar holes. The ulnar position of −4 to 4 was the most isometric for 5 of the 10 specimens. For the other 5 specimens, ulnar positions from 20 to 32 were best. The second most isometric ulnar positions were 0 to 4 for 4 of the 10 specimens, with the other 6 ranging from 12 to 32.
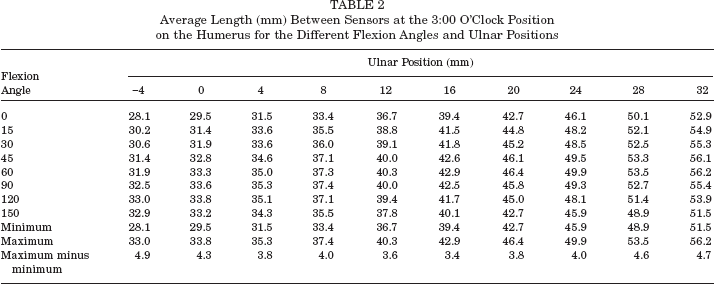
We further investigated the most isometric humeral positions of 3:00 and 4:30 o'clock. With the humeral tunnel at 3:00 o'clock, the most isometric ulnar position was 16, with a maximum-minus-minimum difference of 3.4 mm between the humeral and ulnar sensors throughout the elbow's range of motion. The minimum distance between the humeral and ulnar positions was at 0° for ulnar positions −4 to 20, and at 150° for ulnar positions 24 to 32. The maximum distance between the humeral and ulnar positions was at 120° for ulnar positions −4 and 0, at 90° for ulnar positions 4 and 8, and at 60° for ulnar positions 12 to 32. With the humeral tunnel at 4:30 o'clock, the most isometric ulnar position was at 20, with a maximum-minusminimum difference of 3.8 mm between the humeral and ulnar sensors throughout the elbow's range of motion (Table 2). The minimum distance between the humeral and ulnar positions was at 0° of elbow flexion for all ulnar positions. The maximum distance between the humeral and ulnar positions was at 150° for ulnar positions −4 and 0, at 120 for ulnar positions 4 to 12 and at 90° for ulnar positions 16 to 32 (Table 3).
Average Length (mm) Between Sensors at the 3:00 O'Clock Position on the Humerus for the Different Flexion Angles and Ulnar Positions
Average Length (mm) Between Sensors at the 4:30 O'Clock Position on the Humerus for the Different Flexion Angles and Ulnar Positions

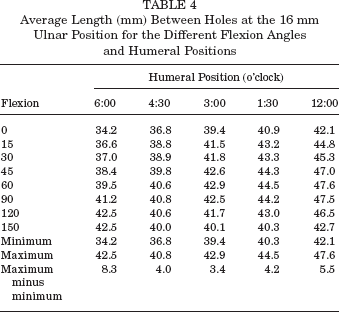
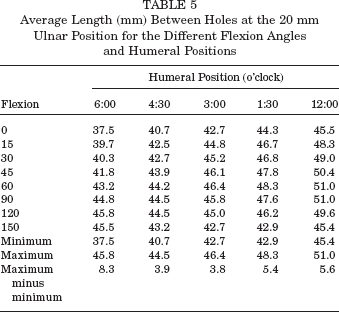
Because of the wide range of the most isometric ulnar tunnel position compared with the narrow range for the humeral tunnel position, we restricted analysis of the ulnar position to those that were most isometric for humeral tunnel positions of 3:00 and 4:30 o'clock, that is, 16 and 20 mm. With the ulnar tunnel at either 16 or 20 mm, the greatest isometry occurred with the humeral tunnel at the 3:00 o'clock position and the second most isometric humeral position was at the 4:30 o'clock position (Tables 4 and 5).
Average Length (mm) Between Holes at the 16 mm Ulnar Position for the Different Flexion Angles and Humeral Positions
Average Length (mm) Between Holes at the 20 mm Ulnar Position for the Different Flexion Angles and Humeral Positions
To determine the optimal position of elbow flexion for graft tensioning, the graft length and maximal strain that a graft would experience throughout a full range of elbow motion were calculated for tensioning at 30°, 45°, and 90° of elbow flexion, which are the recommended positions for tensioning that are found in the literature. For a humeral tunnel positioned at either the 3:00 or 4:30 o'clock position, there were no significant differences in the mean graft lengths or maximum strains for different angles of tensioning (P > .05). However, it must be noted that with the large standard deviations due to individual variations and small sample size the statistical power was limited (0.1 to 0.3).
The height of the radial heads were 10.7 ± 1.03 mm. This means that the ulnar position of +12 corresponds approximately to the level of the radial neck.
Discussion
The principal finding of this study was that there were no universally isometric points for tunnel placement for LUCL reconstruction, and that there was a statistically significant degree of individual variation for optimal insertion points between specimens. The most isometric point for the posterior/distal wall of the humeral tunnel was between the 3:00 and 4:30 o'clock positions on the lateral epicondyle, which were most isometric when paired with an ulnar tunnel whose proximal wall was located 16 to 20 mm distal to the proximal margin of the radial head. For reference, the height of the radial heads of the elbows used in this study from the metadiaphyseal junction to the most proximal margin were roughly 11 mm, meaning that the ulnar tunnel can be placed 5 to 9 mm distal to the radial head-neck junction. This may be verified radio-graphically intraoperatively, if so desired. Van Riet et al 24 have determined that the distance from the proximal aspect of the radial tuberosity to the distal border of the articular cartilage of the radial head averages 13 mm. There was no significant difference in the angle of graft tensioning between 30°, 45°, and 90°.
In the only previous cadaveric study comparing the biomechanical stability of different drill hole placements, there was no significant difference noted between an ulnar tunnel placed distally at the level of the supinator crest (at the level of the radial neck, according to the figure accompanying the article) and a tunnel placed proximally at the level of the proximal aspect of the lesser sigmoid notch (ie, the proximal margin of the radial head). 10 Differences in stability for different humeral tunnel placements were not evaluated. As both proximal and distal ulnar tunnel placement provided similar stability, recommendations for tunnel placement should be based on isometry to allow for maximum postoperative elbow motion.
Even though Ball et al 3 have stated that “it is critical that the graft be placed at the isometric point of the elbow or the reconstruction will constrain normal motion,” we were unable to locate tunnel locations for LUCL tendon graft reconstruction that were completely isometric. We noted that the humeral and ulnar tunnels became closer in extension, decreasing graft tension when graft tension is most needed to restrain PLRI. This is similar to the results of Moritomo et al, 14 who noted that the native LUCL is loose in elbow extension and becomes tight with flexion. This may also lead to increased tension and strain in the tendon graft at increasing angles of elbow flexion. The LUCL tendon graft reconstruction probably relies on some degree of graft creep to allow full elbow flexion, as well as some scarring of secondary stabilizers to prevent PLRI in elbow extension. As the native LUCL is nonisometric, it is currently unclear as to whether a tendon graft should optimally be made more isometric or more anatomical. However, an isometric graft should re-create a check-rein against instability in all positions of elbow motion while still allowing full mobility.
It should be noted that the tendon graft resists abnormal supination of the radial head off the capitellum in supination and relative extension (ie, PLRI) by providing a properly tensioned check-rein against the distal/posterior humeral tunnel wall and the proximal ulnar tunnel wall in extension. Therefore, this study should be interpreted as suggesting where the distal wall of the humeral tunnel and the proximal wall of the ulnar tunnel should be placed, not where these tunnels should be centered. This is similar to the advice of Cohen, 4 who notes that it is important that the posterior edge of the (humeral) tunnel is at the (most) isometric point, as the graft functionally heals along this posterior cortex. As PLRI occurs in extension, the literature suggests that it may be helpful to err on the side of placing the humeral tunnel slightly anteriorly/superiorly to the most isometric point so that the graft is not lax in extension, where it is most needed.4,16,17,19 Our recommendation for humeral tunnel placement is similar to that of Cohen, 4 whose figure illustrates the posterior wall of his tunnel at approximately the 3:00 o'clock position. His recommended position for the ulnar tunnel at the level of the proximal margin of the radial head is similar to the most isometric or the second most isometric point found in 5 of our 10 specimens. However our mean most isometric point for all 10 cadavers was 16 mm distal to this point, closer to that recommended by Morrey and O'Driscoll,16,17 Nestor et al, 18 and O'Driscoll and Morrey 19 : at the level of the radial head-neck junction, which averaged 11 mm distal to the proximal margin of the radial head.
Although up to 2 to 3 mm of valgus laxity may be tolerated on the medial side of the elbow even in throwing athletes2,3,22 and valgus laxity of even greater magnitudes may not be symptomatic in the majority of patients, especially those not performing heavy labor or engaged in vigorous sports,9,11 it is unclear what degree of laxity may be tolerated on the lateral side by the majority of patients. Similar to the medial side of the elbow, it is very possible that the degree of laxity allowed by a few millimeters of graft laxity is well tolerated. Therefore, a slight amount of graft laxity in full extension may not be symptomatic.
The literature disagrees on optimal LUCL tunnel placement, but many authors recommend graft placement and tensioning guidelines similar to those presented here. Olsen and Sojbjerg 20 advised placing the drill holes in the lateral epicondyle at the center of joint rotation and one ulnar tunnel at the level of radial head-neck junction, with another more distal. They recommended graft tensioning at 90° of flexion. Yadao et al 25 included a figure showing one ulnar tunnel at the level of the radial neck and another more distal. The distal wall of the humeral tunnel is shown at the 4:30 o'clock position. Lehman 12 shows a single ulnar tunnel at the level of the radial neck and a humeral tunnel at the 4:30 o'clock position.
Nestor et al 18 state that the ulnar hole is just posterior to the tubercle of the supinator crest. A figure published in their article shows the ulnar drill holes to be at the level of the radial head-neck junction and distal to that. The humeral tunnel is made at the point of isometry, which is located by “placing a temporary suture in the ulnar tunnel and holding the ends of the suture against the humerus with a snap while the elbow is moved.” A figure shows the distal wall of this hole to be at the 3:00 o'clock position. The reconstruction is tensioned with the elbow flexed 30° and the forearm fully pronated. 18 Morrey and O'Driscoll16,17,19 advise placing the ulnar hole just posterior to the supinator crest at the level of the radial head-neck junction, with a second hole 1 to 1.25 cm proximally, near the insertion of the annular ligament. The same advice involving suture determination of humeral tunnel isometry is given, with the isometric spot on the humerus noted to be “generally more anterior and proximal than might be apparent.” The figures accompanying their articles show this isometric point to be between the 3:00 and 4:30 o'clock positions. The graft is tensioned at 40°.
The illustration in the article by Cohen 4 shows that he also recommends a humeral tunnel location close to 3:00 o'clock, between 3:00 and 4:30. He recommends placing the ulnar tunnels at the level of the proximal margin of the radial head. He notes that, theoretically, more distal tunnels may provide better resistance to varus stress, while more proximal tunnels provide better resistance to joint subluxation in supination. He recommends graft tensioning at 45°.
Moritomo et al 14 published an MRI study that recommended placement of the humeral tunnel 2 mm proximal to the center of the capitellum, anterior to the lateral epicondyle. However, most authors recommend placement of the humeral tunnel through the lateral epicondyle, with excellent clinical results reported.16,17,19,20,23,25 These authors noted a detouring of their virtual LUCL reconstruction's path due to the bone of the lateral condyle; this might have been increased by their placing the humeral origin of the virtual reconstruction on the flat part of the surface of the lateral condyle instead of through the lateral epicondyle.
This study has all of the usual limitations of cadaveric studies. We used simple markers to represent tunnel sites; full-sized tunnels were not actually drilled and tendon grafts were not actually inserted. However, this should not decrease the accuracy of the measurements obtained. In addition, this model assumes that the LUCL travels in a straight line from origin to insertion, which may not truly mimic normal anatomy. Only discrete pairs of points were tested, and the optimally isometric point may not have been captured for each elbow. Although the overall effects of humeral and ulnar positions were statistically significant, one of the main findings of the study was the large variability between individual elbows in the maximally isometric graft insertion points. There may be specific anatomical features relating to individual joint morphologic characteristics that can explain this variability, but we did not identify those features in this study. Nevertheless, while we could not identify the most optimal isometric points with statistical significance, the data as a whole describe a general trend that can provide guidance to surgeons in selecting graft insertion sites.
The exact isometric points could not be determined by this study, and we merely localized the most isometric point for the posterior/distal wall of the humeral tunnel to be between the 3:00 and 4:30 o'clock positions on the lateral epicondyle. However, we believe that our data can help surgeons achieve a repair that is close to the maximally isometric points. We also understand that there is more to performing a successful surgical reconstruction than merely obtaining isometric tunnel positions; the graft must also be fully tensioned and appropriately secured. This study does not provide evidence that decreasing the strain on a tendon graft will improve the longevity of the repair. However, graft isometry should allow optimal tension to be maintained throughout the greatest arc of joint motion while minimizing the creation of joint contractures.
Conclusion
We could determine no truly isometric points for humeral and ulnar tunnel placement for LUCL tendon graft reconstruction. There was a significant degree of individual variation in the maximally isometric insertion sites. Lack of isometry may simply be a reality when trying to reconstruct a ligament complex with a 2-cm wide insertion with a relatively narrower tendon graft. 5 The most isometric points were on the supinator crest, 16 to 20 mm distal to the proximal margin of the radial head for the proximal wall of the ulnar tunnel and between the 3:00 and 4:30 o'clock positions on the lateral epicondyle for the posterior/distal wall of the humeral tunnel.