
Abstract
Background: Double-bundle ACL reconstruction popularity is increasing with the aim to reproduce native ACL anatomy and improve ACL reconstruction outcome. However, to date, only a few randomized clinical studies have been published.
Purpose: The aim of this study was to prospectively compare the clinical results of single- and double-bundle ACL reconstruction.
Study Design: Randomized controlled clinical trial; Level of evidence, 1.
Methods: Seventy patients with a chronic unilateral ACL rupture who underwent arthroscopically assisted ACL reconstruction using a hamstring graft were randomized to receive a single- (SB) or double-bundle (DB) reconstruction. Both groups were comparable with regard to preoperative data. A double-incision surgical technique was adopted in both groups. The graft was fixed by looping the hamstring tendons around a bony (DB) or a metallic (SB) bridge on the tibial side and with interference screws reinforced with a staple on the femur. The same rehabilitation protocol was adopted. Outcome assessment was performed by a blinded, independent observer using the visual analog scale (VAS) score, the new International Knee Documentation Committee (IKDC) form, the Knee Injury and Osteoarthritis Outcome Score (KOOS), and KT-1000 arthrometer evaluation.
Results: All the patients reached a minimum follow-up of 2 years. No differences between the 2 groups were observed in terms of KOOS and IKDC subjective score. A statistically significant difference in favor of the DB group was found with the VAS ( P < .03). The objective IKDC final scores showed statistically significantly more “normal knees” in the DB group than in the SB group ( P = .03). There was 1 stability failure in the DB group and 3 in the SB group. The KT-1000 arthrometer data showed a statistically significant decrease in the average anterior tibial translation in the DB group (1.2 mm DB vs 2.1 mm SB; P < .03). The incidence of a residual pivot-shift glide was 14% in DB and 26% in SB (P = .08).
Conclusion: In the 2-year minimum follow-up, DB ACL reconstructions showed better VAS, anterior knee laxity, and final objective IKDC scores than SB. However, longer follow-up and accurate instrumented in vivo rotational stability assessment are needed.
Double-bundle (DB) ACL reconstruction is increasing in popularity with the aim to reproduce native ACL anatomy and improve ACL reconstruction outcome. In particular, DB supporters aim at improving anterior and rotational knee stability and increasing knee function.
Controlled laboratory studies26,31,41,42 have shown the superiority of DB ACL reconstruction in restoring intact knee kinematics, including translations and rotations. On the other hand, short-term comparative clinical trials † have achieved conflicting results, with some papers failing to show a difference.1,19,33,35,39 Recent acquisitions in native bundle anatomy, ‡ number of tibial tunnels required, 25 tunnel positioning, and graft tensioning7,20,40,42,43 should improve DB procedures and may lead to different clinical results. At the present time, several DB techniques have been described, including transtibial, 45 transportal, 40 and outside-in3,25 approaches.
References 1, 3, 19, 22–24, 28, 33, 35, 39, 44.
References 6, 9, 10, 11, 27, 30, 34, 36, 38, 47.
In a previous level II clinical trial from our institution, 3 we observed better results in DB ACL reconstruction with an outside-in technique than with a transtibial. This can be explained by a more anatomic femoral tunnel placement achieved by the outside-in technique. The control group consisted of single-bundle (SB) transtibial reconstructions. The current level I study was designed to prospectively compare after a minimum 2-year follow-up outside-in SB and DB reconstructions in patients with chronic ACL injuries treated with the same surgical technique and graft fixation. We hypothesized that a closer replication of ACL anatomy with a DB outside-in technique is more effective than an outside-in SB reconstruction.
Materials and Methods
Seventy consecutive patients with complete, isolated, and chronic ACL lesions (injury surgery interval >6 weeks) were randomized to receive an SB or DB ACL reconstruction with hamstring tendon graft (Figure 1).

CONSORT flow diagram.
All patients fulfilled the following inclusion criteria: (1) closed physes and younger than 40 years old, (2) healthy contralateral knee, (3) no previous surgeries in the index knee (apart from partial meniscectomy), (4) chondral lesions less than Outerbridge grade III, 29 (5) no patellofemoral symptoms, (6) absence of systemic illnesses, and (7) compliance to enter the 2-year follow-up study. Ethical approval was obtained from the Internal Review Board. All subjects were informed of the study design and gave informed consent, but they were blinded to the type of procedure adopted. The patients became aware of the received procedure 1 year after surgery, when they underwent a radiographic evaluation.
Demographics, Injury History, and Preoperative Assessment
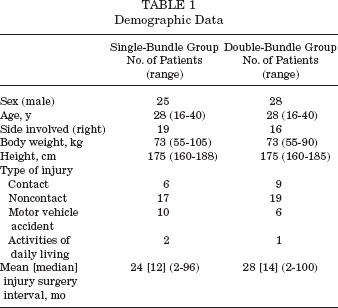
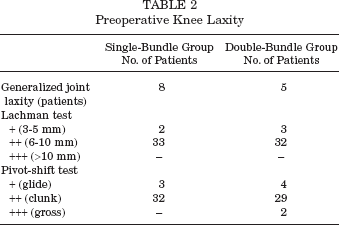
Patients were comparable for age, sex, body weight, height, generalized joint laxity, operated side, preinjury sports activity level, mechanism of injury, time from injury to operation (Table 1), and preoperative anterior and rotational knee laxity (Table 2). Generalized joint laxity according to the criteria of Carter and Wilkinson 5 was observed in 8 patients in the SB group and in 5 patients in the DB group. Twenty-four patients (69%) in the SB group and 27 patients (77%) in the DB group played pivoting sports before injury. Previous surgery included 4 partial arthroscopic medial meniscectomies in the DB group only. The above differences were not statistically significant. Preoperative stability assessment revealed no differences between the 2 groups (Table 2).
Demographic Data
Preoperative Knee Laxity
Surgical Technique
All the procedures were performed by the senior author (P.A.) with the use of a tourniquet. Complete ACL tear was confirmed at arthroscopy. The medial meniscus was torn in 10 knees (29%) in both groups. The lateral meniscus was torn in 5 knees (14%) in the SB group and in 3 (9%) in the DB group. Three medial meniscal lesions were sutured in the SB group. A limited partial meniscectomy was performed in all other cases. A stable longitudinal lesion (<1 cm) of the medial or lateral meniscus was left untreated in 4 knees (11%) in the SB group and in 5 knees (14%) in the DB group.
Semitendinosus and gracilis tendons were harvested through an oblique approach medial to the tibial tubercle over the pes anserinus by using a smooth tendon stripper (Linvatec, Largo, Florida). The tendons were cleaned of soft tissue, and the free ends were armed with No. 1 Vicryl absorbable sutures in a criss-crossing Chinese finger-trap pattern. The grafts were pretensioned on the suture board. In both groups, the torn ACL was debrided, and the anatomical tibial and femoral footprints of the 2 bundles, when present, were preserved and marked with a radiofrequency ablator (VAPR, De Puy Mitek, Raynham, Massachusetts). No notchplasty was necessary. All graft diameters were measured in 0.5-mm increments, and the tibial and femoral bone tunnels were drilled accordingly.
DB Procedure
Two tibial tunnels were drilled. The anteromedial (AM) guide wire was drilled through the Howell 65° tibial guide anterior hole as previously described 3 (Figure 2). The posterolateral (PL) guide wire was drilled with a prototype rod guide (Smith & Nephew Inc, Andover, Massachusetts), which was inserted in the AM tunnel (Figure 3). The articular exit of the PL guide wire was at a fixed distance (8 mm) posterior to the center of the AM tunnel toward the lateral aspect of the posterior cruciate ligament (PCL) (Figure 4). This prototype guide represents the evolution of a previously validated guide demonstrated to accurately and reproducibly place the tibial guide wire in an anatomic position. 18 The previous guide 18 was improved to include a different slot to drill the PL femoral tunnel. The angulations and directions of the tibial tunnel were preserved.

In the double-bundle (DB) technique, to aim the center of the AM bundle attachment, the tibial anteromedial (AM) guide wire was inserted through the Howell 65° tibial guide anterior hole.
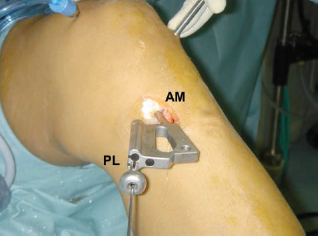
The posterolateral (PL) guide wire was drilled with a prototype rod guide inserted in the anteromedial (AM) tunnel.
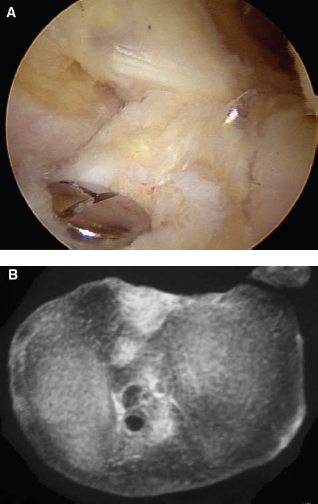
A, The articular exit of the posterolateral (PL) guide wire was 8 mm posterior to the center of the anteromedial (AM) tunnel, and its mediolateral position could be adjusted relying on an aiming sulcus on the tip of the rod. B, Computed tomography (CT) scan in axial view showing the position of the intra-articular exit points of the tibial tunnels in the tibial plateau.
The 2 femoral tunnels were drilled outside-in keeping the knee at 90° of flexion. The arthroscope was inserted into the joint from the AM portal, looking at the lateral wall of the notch. We believe that the view from the AM portal is particularly useful for adjustment of the deep-shallow position of the tunnels. The AM guide wire was inserted with a front-entry guide (Shino Guide, Smith & Nephew Inc) as deep as possible on the lateral wall below the over-the-top position so as to have the entire tunnel exit on the lateral wall and not on the roof (Figure 5). The PL wire was drilled 9 mm apart and shallow, about 5 mm from the cartilage border 45 (Figure 6A), using the same prototype rod guide described for the tibial PL tunnel but through a different hole (Figure 6B). With the knee at 90° of flexion, the 2 tunnels in the femur are almost in line and parallel to the tibia. A bony bridge between the tunnels was always present (Figure 7).
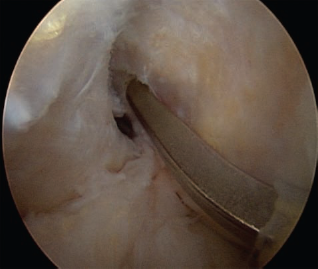
Arthroscopic view from the anteromedial (AM) portal showing the intra-articular arm of the Shino guide and the point we aimed at on the lateral wall of the notch to drill the AM wire (knee at 90° of flexion).
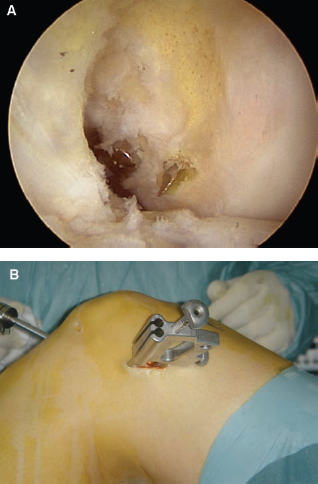
The posterolateral (PL) wire was drilled 9 mm apart and shallow, about 5 mm from the cartilage border (A) using the same prototype rod guide described for the tibial PL tunnel but through a different hole (B). With the knee at 90° of flexion, the 2 tunnels in the femur are almost in line and parallel to the tibia.
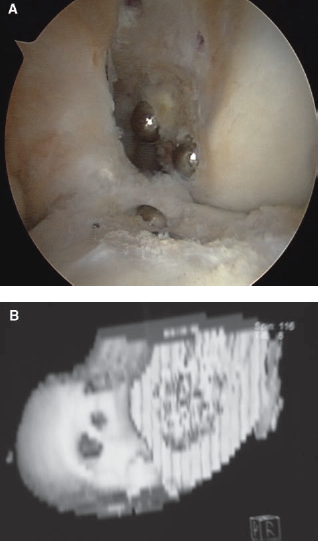
A, Arthroscopic view from the anteromedial (AM) portal showing the position of the 2 exit holes of the 2 femoral tunnels into the wall of the notch. A bony bridge between the tunnels was always present. B, A 3-dimensional computed tomography (CT) scan in sagittal view showing the position of the intra-articular exits of the femoral tunnels on the wall of the notch.
A single semitendinosus/gracilis tendon graft was looped around the bony bridge between the 2 tibial tunnels, exited, and was stitched to the periosteum. The tendon free ends were passed into the joint and exited the lateral femoral cortex. The PL and AM grafts were fixed with the knee at 20° and 40° of flexion, respectively, with two 6-mm outside-in titanium rounded cannulated interference (RCI) screws (Smith & Nephew Inc), under a manual tension per bundle of approximately 20 N. An additional staple secured both grafts to the lateral femoral cortex (Figure 8).

Postoperative radiographic anteroposterior (AP) (left) and lateral (right) views after ACL reconstruction using the double-bundle (DB) technique (left knee). Both femoral tunnels were drilled on the lateral wall and not on the roof.
SB Procedure
The tibial guide wire was drilled with the Howell 65° tibial guide (Arthrotek, Warsaw, Indiana) as previously described. 3 On the femur, the attachments of the 2 bundles were marked as performed in the DB technique, and an “anatomic” (not isometric) SB tunnel was drilled outside-in on the lateral wall of the notch, right in the middle of the AM and PL bundle attachments, using the same Shino guide (Figure 9).
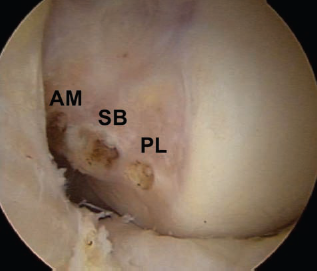
In the single-bundle (SB) technique, the femoral guide wire was drilled aiming a position in the middle of the anteromedial (AM) and posterolateral (PL) bundle attachments.
A pretensioned doubled semitendinosus/gracilis graft was mounted on the working station with the PAG tibial device (Citieffe, Bologna, Italy) and passed into the joint. The PAG is a suspension device and consists of a cortical low profile titanium button articulating with an eyelet of variable length (10 or 20 mm), where the tendons are looped around. Femoral fixation was achieved with a 7- or 8-mm titanium RCI screw at 20° of flexion after cycling under a manual tension of approximately 40 N. An additional staple on the lateral femoral cortex was employed to improve fixation (Figure 10).

Postoperative radiographic anteroposterior (AP) (left) and lateral (right) views after ACL reconstruction using the single-bundle (SB) technique (left knee). A metallic suspension device, which relied on the tibial cortex, was employed to fix the graft distally.
A previously described brace-free rehabilitation protocol 2 was adopted in both groups and initiated after 1 week of postoperative isometric strengthening and flexion restriction. Full range of motion and closed chain strengthening exercises were initiated after 4 and 6 weeks, respectively. Running was allowed after 3 months and return to sport-specific training after 4 to 5 months.
Follow-up Examinations
All the patients were evaluated before surgery, every 2 weeks up to the second postoperative month, monthly up to 4 months after surgery, and then at 1 and 2 years thereafter by an independent and blinded observer (F.G.). Both knees of the patient were covered with a stockinette to prevent any information about the operated side and the incisions.
All the patients were evaluated subjectively and objectively using the visual analog scale 12 (VAS), the Knee injury and Osteoarthritis Outcome Score 32 (KOOS), and the new International Knee Documentation Committee (IKDC) evaluation form. 21 To assess the VAS, we asked the patient to answer the following question: “How would you rate the function of your knee?” marking the score on a line divided in 10 points with 0 labeled as “very poor” and 10 labeled as “excellent.”
Range of motion was measured in relationship to the opposite normal knee using a long-arm goniometer. Extension deficit was determined with the subject lying in the prone position with the legs hanging off the bed, so hyperextension was allowed. Side-to-side difference was evaluated both with a long-arm goniometer and as heel-height difference with the contralateral limb.
Side-to-side difference in anterior tibial translation was assessed with the knee flexed 30° using the KT-1000 arthrometer (Medmetric, San Diego, California) at 134 N and manual maximum force. 8 The pivot-shift test was performed with the patient supine as described by Galway and McIntosh 14 and graded according to the IKDC form as absent, glide, clunk, or gross compared with the contralateral knee.
Before the investigation was initiated, the sample size was estimated on the basis of the hypothesis that there was no difference in anterior-posterior knee laxity between the treatment groups. A clinically relevant difference between groups was considered to be a 1-mm difference in anterior knee laxity when compared with the contralateral uninjured side. The standard deviation, as in a previous trial, 15 was set at 1.5 mm. A power calculation was performed with a confidence level of 95% (α = .05) and a power (1-β) of 80%. This yielded an estimated sample size of 35 patients per group. The randomization was performed via a computer-generated list of random numbers, while the patients were recruited according to the general waiting list by the hospital secretary who was not aware of the study.
All statistical analyses were conducted on Stat Win II software (StatSoft, Tulsa, Oklahoma). We used the Student t test to compare differences between groups and used the χ 2 test and Fisher exact test for categorical variables. In all tests, an a level of .05 was considered significant.
Results
No intraoperative or postoperative complications were recorded. We recorded 3 nontraumatic failures for instability at 1-year follow-up, 1 in the DB group and 2 in the SB group. A traumatic rupture was recorded at 2-year follow-up in the SB group. None of the patients underwent a revision ACL procedure. Two other patients in the DB group underwent surgery during the follow-up period. In one case, at 1 year from ACL surgery, we removed the hardware because of pain and swelling in the distal part of the iliotibial band during sports activities. Another patient with a longitudinal and stable lesion of the posterior horn of the medial meniscus at the time of ACL reconstruction suffered a new meniscal lesion while playing volleyball at 18 months after ACL reconstruction. We performed a partial medial meniscectomy and a second-look arthroscopy, which showed a good and competent ACL.
The mean VAS, KOOS, and subjective IKDC scores significantly increased with time and were improved compared with preoperative scores. No differences were found between the 2 groups in IKDC subjective score and KOOS. After 2 years, the VAS score was significantly higher in the DB group (P < .04) (Table 3).
Subjective Assessment a
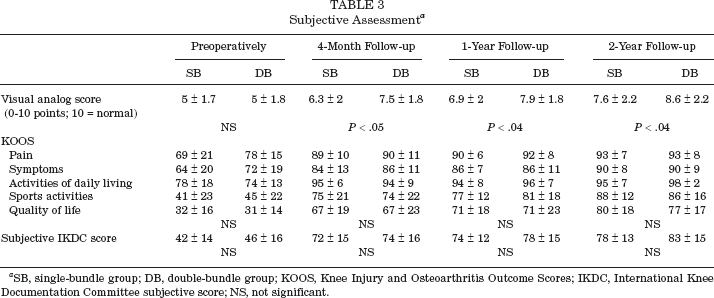
SB, single-bundle group; DB, double-bundle group; KOOS, Knee Injury and Osteoarthritis Outcome Scores; IKDC, International Knee Documentation Committee subjective score; NS, not significant.
All the patients recovered full range of motion within 4 months from surgery. In the SB and DB groups, the range of motion was 2.4° ± 1.7°/0°/133.1° ± 5.9° and 2.1° ± 1.4°/0°/133.3° ± 3.4°, respectively. As to knee extension, the heel-height side-to-side difference in prone position with the leg hanging from the table was within 1 cm in all the cases.
At the last follow-up, a 1+ Lachman test result with a firm end point was recorded in all the patients except 4 (3 in SB group and 1 in DB group). A pivot-shift glide (1+) was recorded in 9 knees (26%) in the SB group and in 5 knees (14%) in the DB group. Three patients (9%) in the SB group and 1 patient (3%) in the DB group had a pivot-shift clunk (2+). The differences between the 2 groups were not statistically significant.
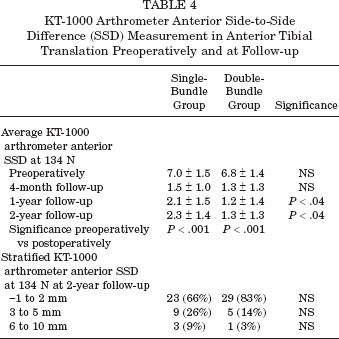
The average KT-1000 arthrometer side-to-side anterior tibial translation showed a significant decrease compared with the preoperative measurements at each follow-up in both groups (P < .001). At 1- and 2-year follow-ups, the average decrease in instrumented knee laxity was significantly greater in the DB group than in the SB group (P < .04) (Table 4).
KT-1000 Arthrometer Anterior Side-to-Side Difference (SSD) Measurement in Anterior Tibial Translation Preoperatively and at Follow-up
At 2-year follow-up, the final objective IKDC score showed significantly more normal results in the DB group (P = .03): normal in 28 (80%) DB and in 20 (57%) SB patients (P = .03), nearly normal in 6 (17%) DB and 12 (35%) SB patients, and abnormal in 1 (3%) DB and 3 (9%) SB patients. No correlations were found between clinical outcomes and sex, meniscectomy, generalized laxity, and anthropometric measurements (height and weight).
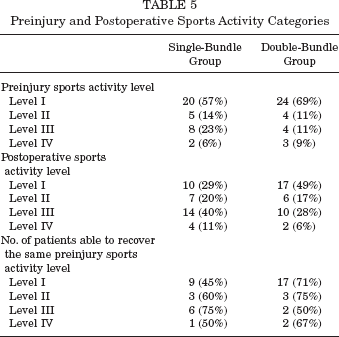
Before ACL injury, 71% (25 of 35) of the patients in the SB group and 80% (28 of 35) of patients in the DB group were involved in IKDC level I or II sports activities. At 2-year follow-up, 17 patients (49%) in the SB group and 23 (66%) in the DB group were active in level I or level II sports activities. If we compare the preoperative and postoperative IKDC level in every single patient, we found that 19 patients (54%) in the SB group and 24 patients (69%) in the DB group were able to recover the same preinjury sports activity level (Table 5). There were no statistically significant differences between the 2 groups, but if we compare the number of patients of the 2 groups able to recover level I sports activities after surgery, we recorded a trend toward significance (P = .08) in favor of the DB group.
Preinjury and Postoperative Sports Activity Categories
Discussion
The main finding of this investigation is that, after 2-year minimum follow-up, outside-in DB ACL reconstruction showed better VAS, final objective IKDC scores, and improved anterior knee stability compared with outside-in SB reconstruction. A trend toward less pivot shift and more sports activities recovery was also observed.
The DB ACL reconstruction was introduced to replicate native ACL anatomy, which consists of 2 main functional bundles, the AM, taut through full range of knee motion, and the PL, taut mainly toward extension. 31 The different behavior of the 2 bundles should affect knee kinematics, and it has been hypothesized13,46,47 that the AM bundle, which is closer to the line of knee axial rotation, controls mainly anterior laxity while the PL bundle, which is more divergent to the axis, should better control rotation. The latter should also be involved in controlling the pivot-shift phenomenon, which is a combination of abnormal rotation and translation.
In vitro laboratory studies have confirmed the superiority of the DB reconstruction in controlling anterior tibial translations,26,31,41,42 internal rotation, and simulated pivot shift.26,31,41,42 Conversely, in vivo comparative studies1,3,22–24,33,35,39,44 had led to different and sometimes conflicting results. While laboratory experiments place the graft exactly at the site of native bundle attachments, in vivo experiences suffer the drawbacks of the subjectivity of tunnel positioning in the lack of definitive landmarks. Furthermore, different approaches (ie, transtibial, transportal, outside-in) lead to different tunnel positions. 16
Adachi et al 1 found no differences between SB and DB reconstruction with a preliminary technique consisting of 1 tibial and 2 transtibial femoral tunnels. Jarvela, 22 after 1 year, reported superior stability results in both translational and rotational in a DB group with a transportal technique. After 2 years, 23 his results were confirmed. In those studies, he also reported a higher incidence of failures with the SB technique. Streich et al 35 and Siebold at al 33 used a transtibial technique both for SB and DB reconstructions and found no advantages in using a DB technique. With the same approach, Kondo et al, 24 in a comparative but not randomized study, evaluated 328 consecutive patients and observed improved anterior stability and less pivot shift after DB compared with SB reconstruction. In our previous comparative level II study, 3 we found better anterior and rotational stability results only when we compared DB outside-in to SB transtibial and no differences between DB transtibial and SB. On the basis of these conflicting in vivo results, we may hypothesize that tunnel placement plays a major role in DB reconstruction outcome.
The transtibial technique has the advantage of achieving a reproducible tunnel positioning, but this is limited by the position and angulation of the tibial tunnels. Moreover, cadaveric studies showed that the transtibial approach is not accurate both in SB4,16 and in DB ACL resconstruction. 18 The transportal technique is less constrained, but knowledge of anatomy is required to place the tunnels in the proper position. The double-incision outside-in approach is today not very popular, mainly because a lateral accessory incision is required. However, the available jigs easily allow the instruments to reach the most posterior and proximal part of the lateral notch, which is where the ACL attachment lies.
In recent years, with the enthusiasm for the DB technique, the ACL attachment anatomy, particularly for the femur, has been revisited.6,10,30,34,47 On the femur, the ACL fibers attach exclusively on the wall and not on the roof of the notch. From an arthroscopic point of view, it is useful to remember that all the femoral ACL attachment lies along the posterior articular cartilage border and is vertical with the knee in extension and assumes a horizontal direction with the knee at 100° of flexion. 34 At 90° of flexion, the AM bundle attachment is deep and high just below the over-the-top position. The PL bundle attachment is shallow, 5 mm from the cartilage contour. 45
With an outside-in approach, the surgeon is free to select the desired position on the wall according to his or her experience and to the data available from the literature. As a consequence, we designed our study to compare a DB technique and an anatomic SB according to the recently revised anatomic landmarks.34,44,46,47 However, in the present study, no CT or MRI scan was performed after surgery to evaluate tunnel position. The anatomic position can be assumed on the basis of the experience of the surgeon, who is well acknowledged and has performed several investigations on ACL anatomy.15,16,17
In our study, the same surgical technique was employed in both groups including graft type, outside-in technique, and graft fixation. The latter relied on cortical bone fixation on the tibia and interference screw plus a staple on the femur. Our unique graft fixation technique ensures the whole length of the tunnel is filled with the graft, and there is a very strong cortical fixation on the tibial side. Alternatively, the graft could be looped around the femoral bone bridge and fixed on the proximal tibia. Furthermore, in our DB technique, the AM and PL bundle grafts have the same diameter. Finally, the SB tunnel was placed right in the middle of the 2 bundle tunnels, on the femur and tibia.
After 2 years, the DB group showed better anterior stability results. We were not able to find a statistically significant difference in terms of residual pivot-shift incidence as we observed in a previous study. 3 In the present study, we were able to record just a trend in favor of DB but not a statistically significant difference. This could be ascribed to several factors: (1) a better performance of the “anatomic” SB outside-in reconstruction,37,42 (2) the subjectivity of pivot-shift testing and grading, and (3) the relatively small number of patients. With the current data, a post hoc power analysis was performed to estimate the sample size required to analyze the pivot shift. As a result, 72 patients per group would be necessary. On the other hand, with objective arthrometric measurement, significant differences between the 2 groups were observed in terms of anterior tibial translation.
The main limitation of this study is that no definitive conclusions can be drawn about the pivot shift. Sample size was calculated on the KT-1000 arthrometer, an anterior tibial translation difference greater than 1 mm, and this allowed us to find significant differences. Furthermore, the pivot-shift assessment still remains subjective, and an instrumented measurement is needed. Nevertheless, a trend toward a pivot-shift reduction was evident and is encouraging.
Conclusion
After 2 years, the clinical results are in favor of the DB reconstruction as demonstrated by the better VAS and final objective IKDC scores and lower KT-1000 arthrometer side-to-side difference in anterior tibial translation. A trend in favor of the DB group in pivot-shift incidence and sports activity recovery was recorded but did not reach statistical significance.