
Abstract
Background: Arthroscopic microfracture is frequently used to repair osteochondral lesions of the talus. However, despite the popularity of this technique, no study has been conducted on cartilage repair after microfracture by second-look arthroscopy.
Purpose: The purpose of the present study was to evaluate cartilage repair in osteochondral lesions of the talus by second-look arthroscopy and to compare arthroscopic findings with clinical outcomes 12 months postoperatively.
Study Design: Case series; Level of evidence, 4.
Methods: Second-look arthroscopies were performed in 20 ankles of 19 patients at 12 months postoperatively. Arthroscopic findings were classified using the Ferkel and Cheng staging system, and cartilage repair was assessed using the International Cartilage Repair System (ICRS). Clinical outcomes were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale.
Results: According to the Ferkel and Cheng staging at second-look arthroscopy, 7 of the 20 ankles (35%) showed incomplete healing (stage D). In terms of ICRS overall repair grades, 8 ankles (40%) were abnormal (grade III). Mean AOFAS scores for Ferkel and Cheng stages A to C (n 5 13) and stage D (n 5 7) were 88.5 and 82.0 points, and those for ICRS repair grades I and II (n 5 12) and grade III (n 5 8) were 88.7 and 82.5, respectively. Good correlations were found between AOFAS scores and Ferkel and Cheng stages and ICRS grades. Overall, 90% of ankles achieved an excellent or good AOFAS score of over 80 points.
Conclusion: Second-look arthroscopic findings at 12 months postoperatively after microfracture for osteochondral lesions of the talus revealed that 40% of lesions were incompletely healed. Nevertheless, the majority of patients achieved a good clinical outcome. Furthermore, postoperative clinical scores were found to be correlated with ICRS repair grades.
Treatments for osteochondral lesions of the talus vary from nonoperative to open and arthroscopic procedures. Operative procedures include debridement, curettage, abrasion, subchondral drilling, microfracture, osteochondral grafting, and chondrocyte transplantation.10,12,13,23
Arthroscopic bone marrow stimulation is the primary technique used to treat symptomatic osteochondral lesions of the talus because the resultant fibrocartilage formation provides satisfactory clinical results at long-term follow-up in many patients, and because the arthroscopic procedure causes less morbidity than open surgery.6,10,24 Microfracture induces a healing response in osteochondral lesions because the microdamage inflicted on subchondral bone stimulates chondroprogenitor cells of the marrow. 25 Several investigators have reported good clinical results in over 70% of patients with osteochondral lesions of the talus after microfracture, and a return to preoperative activity levels at 4 months postoperatively in successful cases.3,9,12
Several studies have evaluated cartilage repair in osteochondral lesions of the talus after microfracture using specialized MRI sequences.3,12, 20 However, the efficacy of MRI in terms of assessing repaired cartilage quality has not been established, and it has been suggested that arthroscopy may better predict the degree of articular cartilage repair.3,22 Nevertheless, no study of cartilage repair after microfracture of osteochondral lesions of the talus by second-look arthroscopy has been performed to date.
The purpose of the present study was to evaluate cartilage repair after microfracture for osteochondral lesions of the talus by second-look arthroscopy and to compare arthroscopic findings with clinical outcomes 12 months postoperatively.
Materials and Methods
This study was approved by the institutional review board of Chonnam National University, and informed consent was obtained from all patients. Between November 2005 and September 2006, 22 patients (23 ankles) with osteochondral lesions of the talus underwent arthroscopic microfracture surgery; 1 patient underwent a staged bilateral microfracture procedure. We suggested to patients that they undergo second-look arthroscopy to evaluate cartilage repair at 12 months postoperatively. Nineteen patients (20 ankles) agreed to the follow-up procedure and 3 refused. However, no patient consented to biopsy during follow-up arthroscopy. The subjects of the present study were 15 men and 4 women with an average age of 38 years (range, 19–51) at the time of index surgery. Mean body mass index (BMI) of patients was 24.2 kg/m2 (range, 19.7–31.1). According to the American Society of Anesthesiologists (ASA) physical status classification, 16 patients were of class I (healthy) and 4 were of class II (mild systemic disease). The mechanisms of injury were believed to be traumatic in 18 ankles and of unknown origin in 2. Mean symptom duration was 22 months (range, 4–60). Osteochondral lesions of the talus involved 13 right and 7 left ankles; the lesions were localized posteromedially in 16 ankles (80%) and anterolaterally in 4 (20%). Mean osteochondral lesion size was 0.9 cm2 (range, 0.6–1.3) (Table 1).
Second-Look Arthroscopic Findings and Clinical Outcomes after Microfracture for Osteochondral Lesions of the Talus a
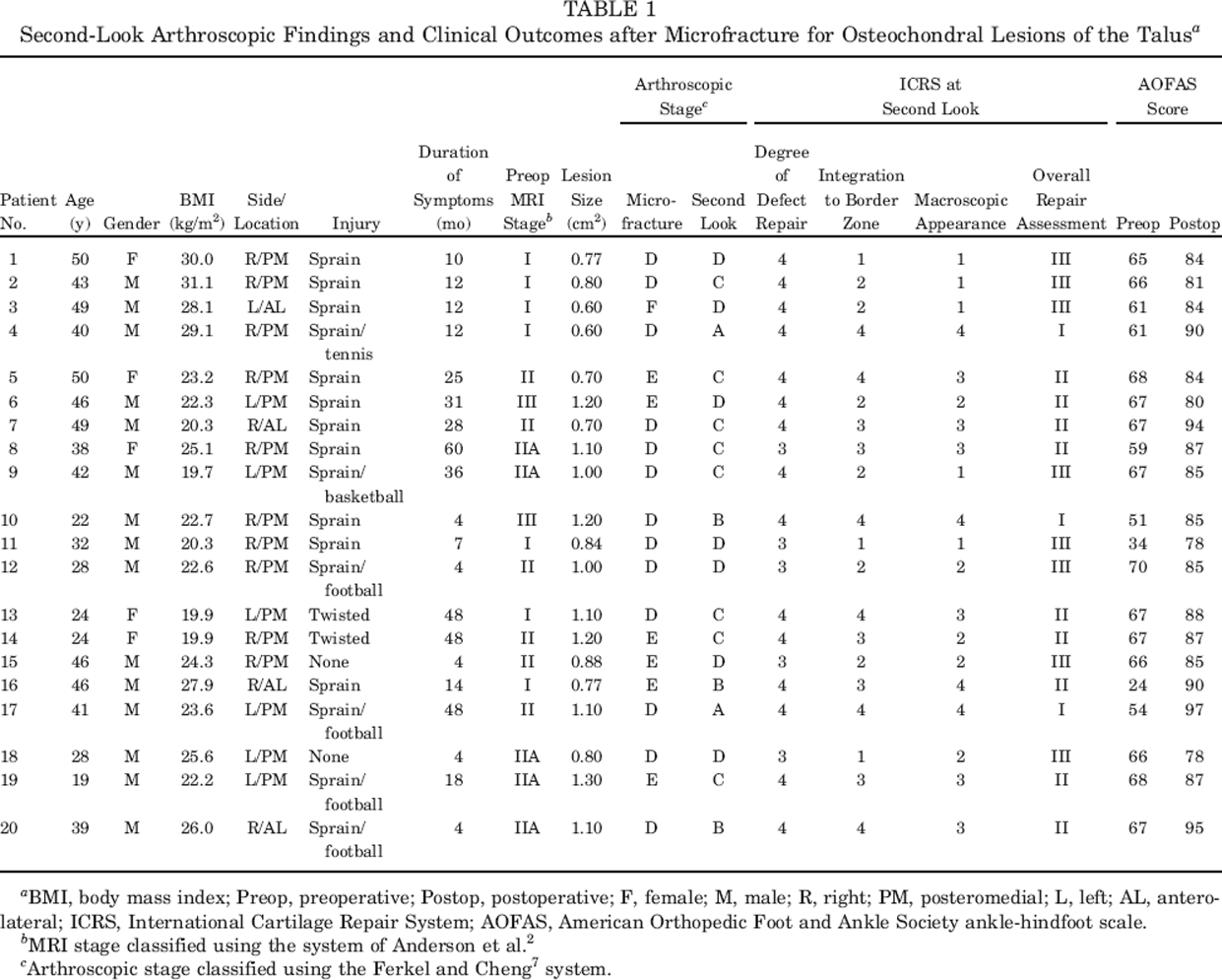
BMI, body mass index; Preop, preoperative; Postop, postoperative; F, female; M, male; R, right; PM, posteromedial; L, left; AL, anterolateral; ICRS, International Cartilage Repair System; AOFAS, American Orthopedic Foot and Ankle Society ankle-hindfoot scale.
MRI stage classified using the system of Anderson et al. 2
Arthroscopic stage classified using the Ferkel and Cheng 7 system.
Radiographic staging was classifiable in 10 of 20 ankles (50%) preoperatively and at 12 months postoperatively using the classification system of Berndt and Harty. 4 An arthritic rating scale employing 4 grades (0-III) was used to classify the extent of degenerative changes for all radiographs. 30 The MRI stage was classified using the system developed by Anderson et al. 2 Preoperative MR images were available for all 20 ankles, but MRI was not performed routinely at 12 months postoperatively (only in 3 patients [3 ankles] who experienced persistent pain after microfracture). All preoperative MR images were independently staged by one radiologist who was unaware of clinical information.
Our candidates for arthroscopic microfracture were selected using the following criteria: chronic symptomatic osteochondral lesions of the talus (no improvement after nonoperative treatment for longer than 3 months), no previous ankle surgery, a lesion of less than 1.5 cm2 with frayed cartilage, and age 50 years or younger. The exclusion criteria applied were degenerative change, ankle instability, and any other associated injury of the ankle joint.
Surgical Techniques and Rehabilitation
Arthroscopic microfractures were performed under general anesthesia using a tourniquet. Atraumatic distraction was performed using a foot strap. A 2.5-mm, 30° arthroscope (ConMed Linvatec, Largo, Florida) and 3 portals (anteromedial, anterolateral, and posterolateral) were used during all procedures. Limited synovectomy was performed in all patients and all unstable cartilaginous and fibrotic tissues were debrided. Sharp, perpendicular margins were created to optimize marrow clot attachment conditions. The microfracture holes were created approximately 3 to 4 mm from the periphery to the center of the lesion with use of a systematic spiral pattern of subchondral bone penetrations throughout the cartilage lesion using arthroscopic awls. The tourniquet was released after this procedure and adequate bone bleeding and marrow fat droplet formation at microfracture holes were confirmed. All procedures were recorded on videotape and arthroscopic photographs were taken.
During the postoperative period, a bulky compressive dressing and a posterior plaster splint were applied in the neutral position; these were worn for 1 week. After this, patients wore a removable posterior splint and started early active range of motion and strengthening exercises. All patients were kept nonweightbearing for 6 weeks, followed by partial weightbearing for 2 weeks, and then full weightbearing.
Second-look arthroscopy was performed using previous arthroscopic portals under local intra-articular anesthesia 12 months postoperatively. Active ankle range of motion and tolerable weightbearing were allowed on the second postoperative day.
Arthroscopic and Clinical Evaluations
Arthroscopic videotapes and photographs of index procedures and second-look arthroscopies were presented in random order and assessed by 2 independent observers to reduce the risk of bias. The observer who reviewed second-look arthroscopic findings was unaware of any prior finding. Arthroscopic grades were evaluated using the Ferkel and Cheng 7 staging system (Table 2) and the International Cartilage Repair System (ICRS)5,21 (Table 3). The ICRS grading has been reported to provide a reliable and relevant means of macroscopically evaluating cartilage repair after microfracture or autologous chondrocyte implantation. 29 However, we were unable to find a similar study on the reliability of the Ferkel and Cheng staging system for evaluating cartilage repair. Nevertheless, we used this system to compare preoperative and second-look arthroscopic findings. The ICRS repair grades are allocated using 3 criteria: the degree to which a defect was filled by repair tissue, the degree of integration of repair tissue with adjacent articular cartilage, and the macroscopic surface appearance of the repair site. These subjective arthroscopic evaluation criteria were each assigned a maximum score of 4 points, which were combined for an overall grade (Table 3).
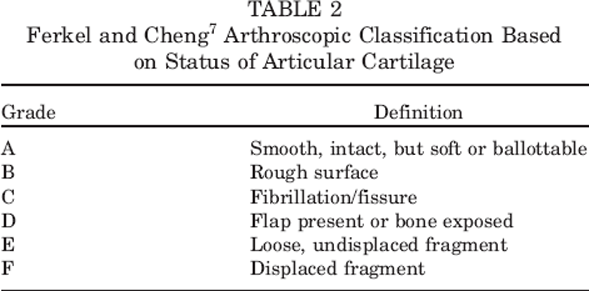
Ferkel and Cheng 7 Arthroscopic Classification Based on Status of Articular Cartilage
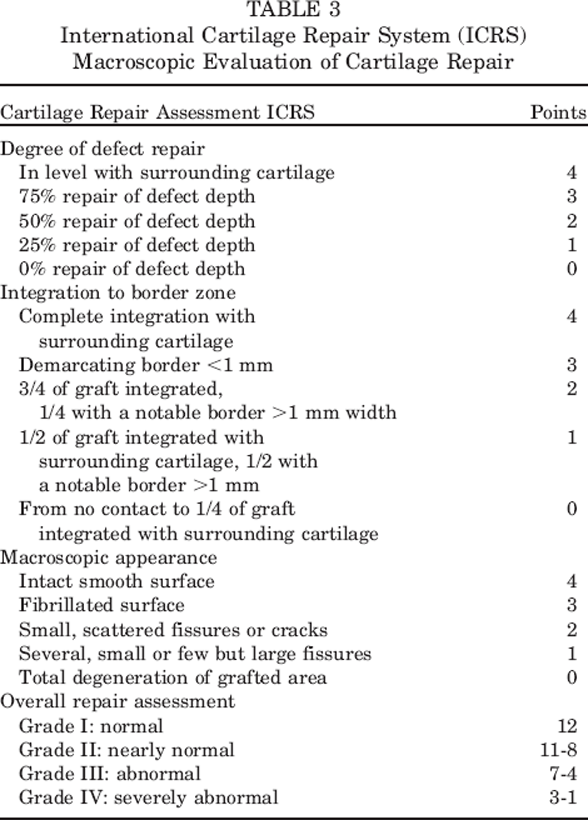
International Cartilage Repair System (ICRS) Macroscopic Evaluation of Cartilage Repair
In addition, clinical outcomes were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale. 14 “Excellent” results were defined as AOFAS scores of 90 to 100, “good” as 80 to 89, “fair” as 70 to 79, and “poor” as less than 70.
Statistical Analysis
Descriptive statistics (arithmetic means, standard deviations, and ranges) were calculated using standard formulas. Correlations between age, gender, BMI, ASA classification, trauma, lesion size, or lesion site and AOFAS scores or ICRS repair grades were analyzed using the independent t test. In addition, we compared arthroscopic repair results (ICRS repair grades, Ferkel and Cheng 7 stages) with AOFAS scores using the independent t test. Probability values of < .05 were considered significantly different. All statistical analyses were reviewed independently by a statistician.
Results
Preoperative plain radiography before the index procedures revealed that 8 ankles were normal and 2 had a subchondral cyst with no apparent osteochondral lesion. Of the 10 ankles classified using the Berndt and Harty 4 staging system, 2 ankles had a stage I lesion, 6 had a stage II lesion, and 2 had a stage III lesion. No stage IV lesion was encountered. Of these 10 ankles radiographed at 12 months postoperatively, 7 had a stage I lesion and 3 had a stage II lesion. According to arthritis rating scale (stage 0-III), the preoperative plain radiographs included 16 stage 0 (80%), 4 stage I (20%), and no radiographs with stage II or stage III arthritis. All patients showed no change in arthritic grade 12 months postoperatively. The results of the AOFAS scores 12 months postoperatively corresponding to preoperative Berndt and Harty 4 stages were as follows: mean 82.5 points for stage I lesion, 86.2 for stage II lesion, and 86.0 for stage III lesion. In addition, we also obtained AOFAS scores at 12 months postoperatively corresponding to preoperative MRI stages: mean 85.0 points in 7 ankles (35%) with a stage I lesion, 86.4 in 5 ankles (25%) with a stage IIA lesion, 88.7 in 6 ankles (30%) with a stage II lesion, and 82.5 in 2 ankles (10%) with a stage III lesion. Arthroscopic microfractures were performed in ankles with preoperative Ferkel and Cheng 7 staging of the following: stage D in 13 ankles (65%), E in 6 ankles (30%), and F in 1 ankle (5%).
Additional arthroscopic findings during index procedures included synovitis in 8 ankles (40%), synovial hypertrophy in 4 ankles (20%), osteophyte in 4 ankles (20%), and loose pieces of cartilage in the joint in 2 ankles (10%). All these lesions were treated at the time of microfracture. By the Ferkel and Cheng 7 classification at second-look arthroscopy, 2 ankles (10%) had a stage A lesion, 3 ankles (15%) had a stage B lesion, 8 ankles (40%) had a stage C lesion, and 7 ankles (35%) had a stage D lesion. Seven of the 20 lesions (35%, stage D) had healed incompletely at second-look arthroscopy. Additional arthroscopic findings at 12 months postoperatively included a fibrotic scar in the joint in 7 ankles (35%) and synovitis in 2 ankles (10%). We treated these lesions and we also performed repeat microfracture on 3 (bone exposed) of 7 lesions with arthroscopic stage D. At second-look arthroscopy, the mean AOFAS score of Ferkel and Cheng stages A through C (n = 13) was 88.5 and the mean score for stages D through F (n = 7) was 82.0, and the scores were significantly different (P =.004).
In terms of ICRS overall repair grades, 12 of the 20 lesions (60%) were of grades I or II (normal or near normal) and 8 (40%) were of grade III (abnormal) (Figures 1 through 4). In detail, based on the 3 subcriteria of the ICRS grading system, 15 of the 20 lesions (75%) showed repair tissue at the level of surrounding cartilage, 6 (30%) revealed complete integration with adjacent cartilage, and 16 (80%) still had macroscopic cracks and fissures. The mean postoperative AOFAS scores of ICRS repair grades were as follows: 88.7 for grades I or II and 82.5 for grade III, and these scores were significantly different (P = .005). Good correlations were found between postoperative AOFAS scores and Ferkel and Cheng 7 stages and ICRS grades (Figure 5).
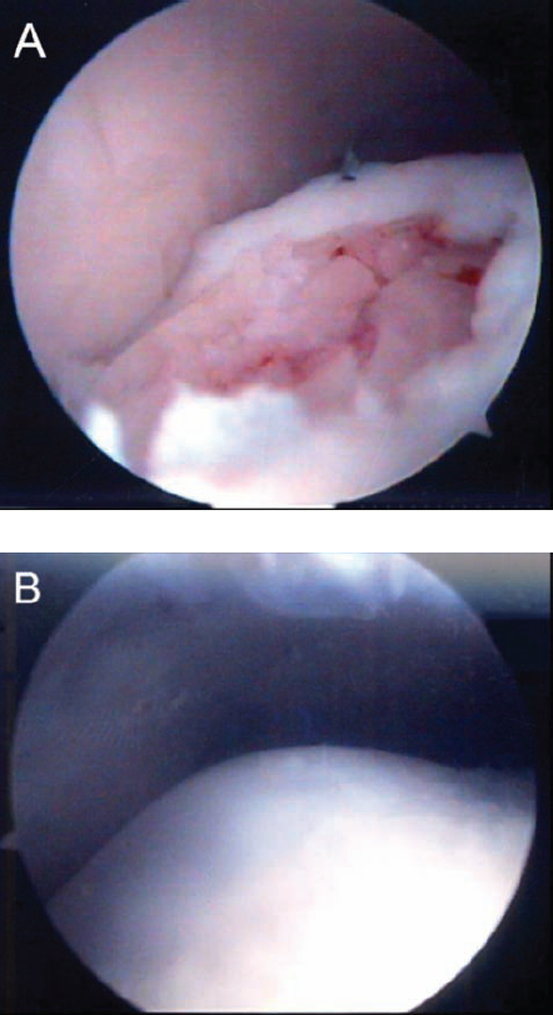
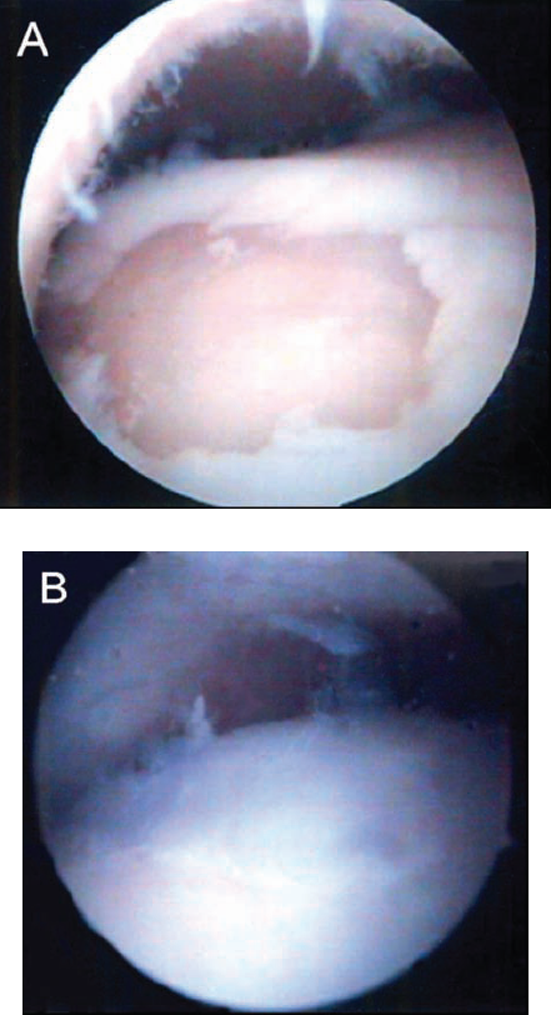
A, arthroscopic view through the anteromedial portal showing the appearance after microfracture in left ankle with a preoperative stage D posteromedial lesion according to the Ferkel and Cheng 7 staging system. B, second-look arthroscopic finding through the anteromedial portal 12 months after microfracture showing an intact smooth surface and completely integrated repair tissue at the level of surrounding cartilage (Ferkel and Cheng stage A and International Cartilage Repair System grade I). The American Orthopaedic Foot and Ankle Society score was improved from 54 points preoperatively to 97 points postoperatively.
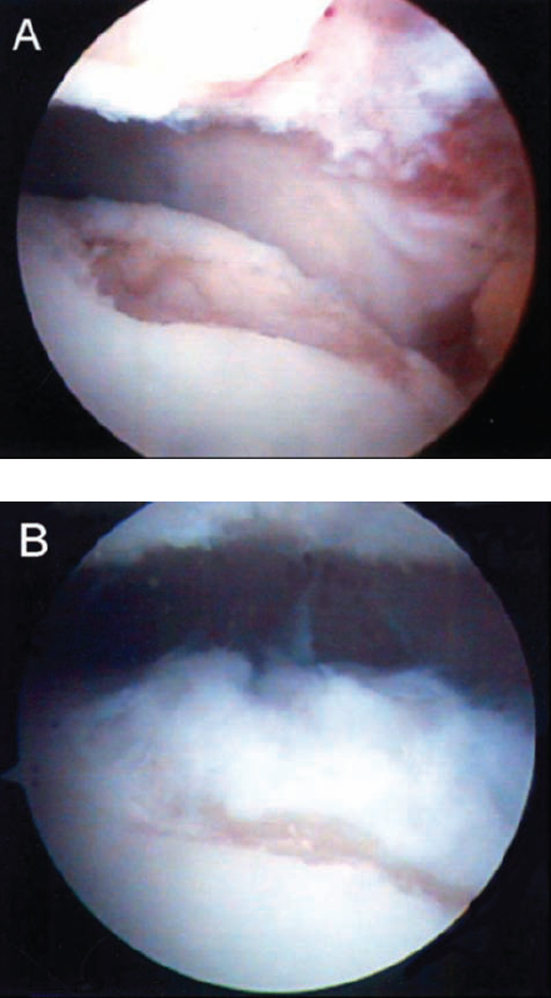
A, arthroscopic view through the anteromedial portal showing status after debridement of loose, undisplaced cartilage in left ankle with a preoperative stage E posteromedial lesion according to the Ferkel and Cheng 7 staging system. B, second-look arthroscopic finding through the anteromedial portal 12 months after microfracture showing a fibrillated soft surface and completely integrated repair tissue at the level of surrounding cartilage (Ferkel and Cheng stage C and International Cartilage Repair System grade II). The American Orthopaedic Foot and Ankle Society score was improved from 68 points preoperatively to 87 points postoperatively.
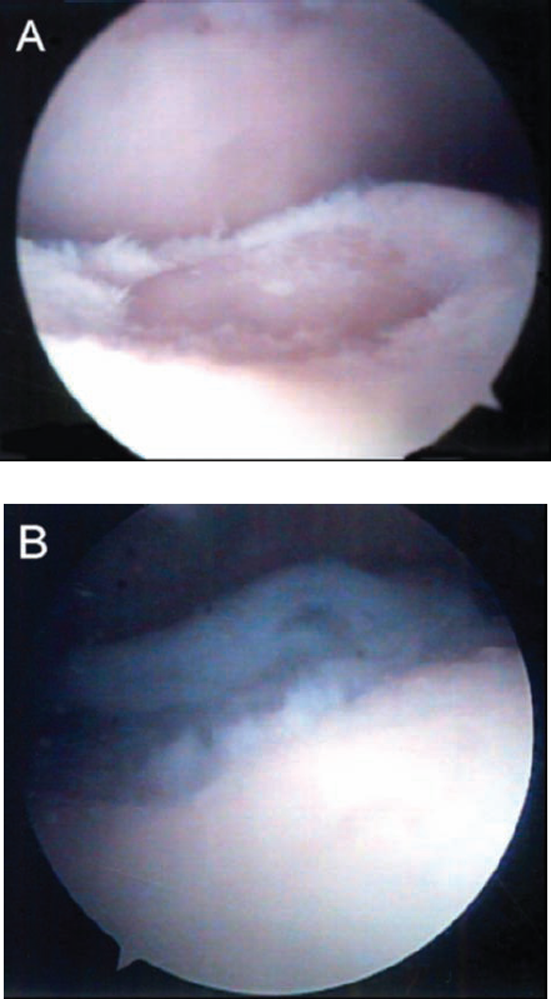
A, arthroscopic view through the anterolateral portal showing the status after debridement of loose, undisplaced cartilage in right ankle with a preoperative stage E lesion (Ferkel and Cheng 7 staging system). B, second-look arthroscopic finding through the anterolateral portal 12 months after microfracture showing soft, hypertrophied, 3/4 repaired tissue integrated with surrounding cartilage, and small fissures of exposed peripheral subchondral bone (Ferkel and Cheng stage D and International Cartilage Repair System grade III). The American Orthopaedic Foot and Ankle Society score was improved from 66 points preoperatively to 85 points postoperatively.
A, arthroscopic view through the anterolateral portal showing status after debridement of flap cartilage in left ankle with a preoperative stage D posteromedial lesion (Ferkel and Cheng 7 staging system). B, second-look arthroscopic finding through the anterolateral portal 12 months after microfracture showing incomplete filling by 50% repair of defect depth and frayed unstable cartilage (Ferkel and Cheng stage D and International Cartilage Repair System grade III). The American Orthopaedic Foot and Ankle Society score was improved from 66 points preoperatively to 78 points postoperatively.
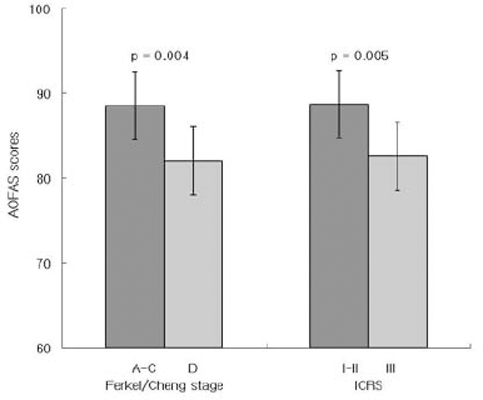
Histogram showing correlation between American Orthopaedic Foot and Ankle Society scores and arthroscopic stages at second-look arthroscopy.
Mean AOFAS scores improved from 60.8 points (range, 24–70) preoperatively to 86.2 (range, 78–97) postoperatively (P < .001), and no patient showed deterioration. Overall postoperative AOFAS scores indicated excellent in 5 ankles, good in 13 ankles, and fair in 2 ankles; that is, 90% of ankles achieved an excellent or good score (>;80 points) (Table 1).
To identify factors that affected clinical scores (AOFAS scores) and arthroscopic repair results (ICRS) at 12 months postoperatively, patients were classified into groups based on patient age, gender, BMI, ASA classification, symptom duration, lesion side and location, and lesion size. However, no significant correlation was found between any of these factors and AOFAS scores or ICRS grades (Table 4).
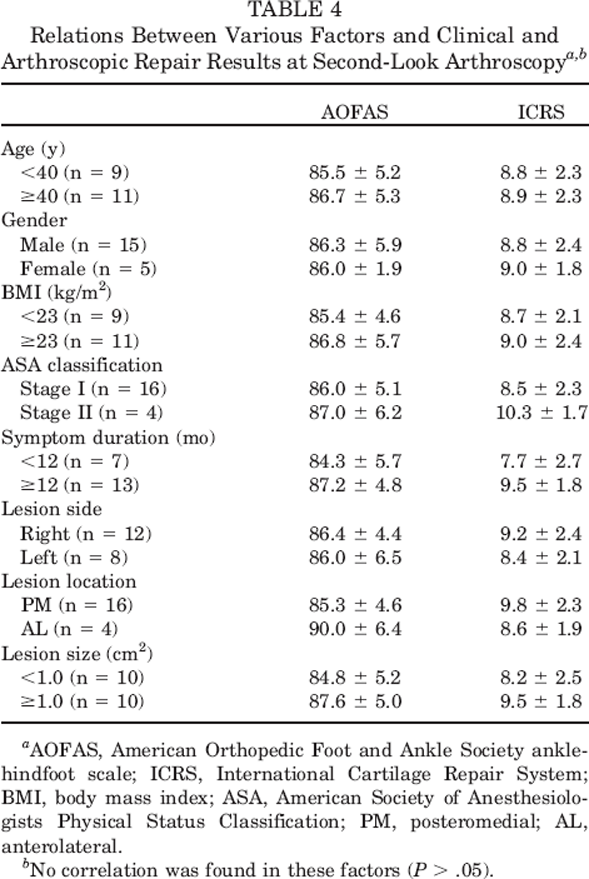
AOFAS, American Orthopedic Foot and Ankle Society ankle-hindfoot scale; ICRS, International Cartilage Repair System; BMI, body mass index; ASA, American Society of Anesthesiologists Physical Status Classification; PM, posteromedial; AL, anterolateral.
No correlation was found in these factors (P > .05).
Discussion
Articular cartilage is a highly specialized tissue type with poor reparative capability, and injuries may lead to chronic pain, joint swelling, the interruption of sports activities, and osteoarthritis. Arthroscopic debridement combined with bone marrow stimulation is the primary treatment for most cases of osteochondral lesions of the talus.6,10 Abrasion, drilling, and microfracture techniques rely on the stimulation of chondroprogenitor cells within the underlying marrow. Drilling has achieved variable success rates.8,17, 27 Recently, Ferkel et al 8 reported long-term results of the arthroscopic treatment for chronic osteochondral lesions of the talus. Arthroscopic excision and drilling were performed in the majority of their patients, which provided 72% excellent and good results by the scale proposed by Alexander and Lichtman, 1 and an average 84 points by AOFAS scores at an average follow-up of 71 months. However, the drawbacks of the transmalleolar approach include iatrogenic damage of opposing tibial articular cartilage due to multiple drill holes and possible heat necrosis when the drilling procedure is conducted without adequate cooling. Furthermore, the transmalleolar approach has been associated with persistent pain and edema, and even the development of stress fractures.23,28
More recently, marrow stimulation by microfracture has gained popularity because it avoids the risk of heat-induced necrosis by drilling and can be used to treat “around-the-corner” lesions using a microfracture awl. 31 Furthermore, it has been reported to produce good clinical outcomes in short-term follow-up studies in both the knee and talus.3,6,16,26
Several factors have been found to influence the outcomes of arthroscopic microfracture.6,8, 23 Chuckpaiwong et al 6 found a strong correlation between lesion size and surgical success in 105 patients who underwent microfracture for osteochondral lesions of the talus. In particular, excellent results were obtained for lesions smaller than 15 mm, regardless of location. Furthermore, the following factors were found to affect outcome negatively: age, a higher BMI, a history of trauma, and the presence of an osteophyte. Ferkel et al 8 reported significant differences between Ferkel and Cheng 7 arthroscopic stages A through C and D through F in terms of Weber and AOFAS scores. However, no relation was found between clinical outcomes and age, gender, lesion side, lesion location, or symptom duration. In the present study, we found a good correlation between arthroscopic repair results at second-look arthroscopy (Ferkel and Cheng stages, and ICRS repair grades) and AOFAS scores.
Some investigators have reported that clinical outcomes progressively deteriorate after microfracture. Kreuz et al 16 reported that deterioration of ICRS score begins 18 months after microfracture of cartilage lesions in the knee and is significantly pronounced in patients older than 40 years. Mithoefer et al 19 also demonstrated that knee function progressively deteriorated mainly in patients with a lack of repair cartilage fill (17% of 48 patients). Furthermore, Ferkel et al 8 reported that 6 of 17 osteochondral lesions of the talus (35%) that had been seen 5 years previously showed a deterioration in terms of clinical result (modified Weber score). Although the reasons for this functional deterioration are unknown, it may be associated with the lack of durability of fibrocartilage. Long-term evaluations are evidently required to determine the durability of cartilage repaired by microfracture.
Several reports have been issued concerning cartilage repair after microfracture of osteochondral lesions of the talus in which the majority of patients were evaluated by MRI. However, the focus of these studies was on clinical outcomes rather than on cartilage repair.3,12, 20 Becher and Thermann 3 reported that all 29 ankles with articular cartilage defects that they examined showed tissue regeneration in microfracture areas by MRI, and that 3 ankles examined by second-look arthroscopy showed softer than normal cartilage but stable complete coverage with redundant fibrocartilaginous repair tissue at 1 year after microfracture. Gobbi et al 12 reported that all 8 ankles in their study showed incomplete filling of cartilage defects by MRI and reduced subchondral edema at 1 year postoperatively. However, the efficacy of MRI with respect to the assessment of cartilage repair has not been established. In fact, arthroscopy continues to be regarded as the procedure of choice. 18 Furthermore, because arthroscopy allows cartilage inspection and palpation with a probe, it also enables soft spots and delaminated areas to be identified.
In the present study, which is the first case series to evaluate cartilage repair after microfracture in osteochondral lesions of the talus by second-look arthroscopy, we describe cartilage repair findings in more detail. Second-look arthroscopic findings at 12 months postoperatively showed that 60% of lesions achieved a normal or near-normal state (ICRS grades I or II) and that 40% lesions remained abnormal (ICRS grade III). Furthermore, it was found that only 30% of the lesions revealed complete integration with adjacent cartilage; that is, lesion peripheries were not as well repaired as lesion centers. Therefore, we recommend that surgeons should pay careful attention to peripheral microfracture.
Nevertheless, in the present study all patients achieved improvements in terms of clinical outcomes. Mean AOFAS scores improved from 60.8 preoperatively to 86.2 at 12 months postoperatively, and overall AOFAS scores revealed excellent or good results of over 80 points in 90% of our patients. These results are consistent with those reported by Gobbi et al, 12 who found that mean AOFAS scores improved from 33.8 to 82.2 regardless of cartilage repair, as determined by ankle MRI at 1 year postoperatively. In addition, Gill and Macgillivray 11 also reported good subjective results in 19 patients with osteochondral lesions of the knee, despite the fact that 58% showed only 0% to 66% defect fill by MRI at a mean follow-up of 3 years.
In terms of knee investigations, Knutsen et al 15 reported an inverse association between macroscopic quality of repair by ICRS and the risk of treatment failure after microfracture. In the present study, ICRS repair grades were found to be significantly correlated with postoperative AOFAS scores, and the 13 patients that improved to Ferkel and Cheng 7 stages A, B, or C also had good or excellent postoperative AOFAS scores (>;80 points). Moreover, 2 fair results (<80 points) were obtained in patients with arthroscopic stage D. Thus, in patients with an unsatisfactory clinical result 12 months postoperatively, second-look arthroscopy with or without further procedure, such as repeat microfracture or osteochondral autograft, can be considered.
The limitations of this study are that the study group was small, the follow-up was short, and no histologic study was conducted. Biopsies present ethical problems, and thus were not performed. Studies involving more cases with long-term evaluations are required.
In summary, second-look arthroscopic findings after microfracture for osteochondral lesions of the talus showed that healing was incomplete at 12 months postoperatively. However, the majority of patients achieved good clinical outcomes, and these improvements were found to be correlated with ICRS repair grades.