
Abstract
Background: Despite improvement in treatment for articular cartilage lesions, prolonged recovery still precludes early return to competitive sports. The challenge of postoperative rehabilitation is to optimize return to preinjury activities without jeopardizing the graft.
Hypothesis: Intensive rehabilitation after second-generation arthroscopic autologous cartilage implantation (Hyalograft C) facilitates graft maturation and safely allows for early return to competition without jeopardizing clinical outcome at longer follow-up.
Study Design: Cohort study; Level of evidence, 3.
Methods: The outcome of 31 competitive male athletes with International Cartilage Repair Society grade III-IV cartilaginous lesions of the medial or lateral femoral condyle or trochlea were evaluated at 1-, 2-, and 5-year follow-up. The athletic cohort was compared with a similar control cohort of 34 nonathletic patients who were treated with autologous chondrocyte implantation. The athletic cohort followed a 4-phase intensive rehabilitation protocol. Eleven of the patients in this cohort were also treated with an isokinetic exercise program and on-field rehabilitation. The patients in the control cohort completed only phase 1 of rehabilitation.
Results: When comparing the 2 groups, a greater improvement in the group of athletes was achieved at 5-year follow-up (P = .037) in the self-assessment of quality of life and International Knee Documentation Committee subjective evaluation at 12 months and at 5 years of follow-up (P = .001 and P = .002, respectively). When analyzing the return to sports activity, 80.6% of the athletes returned to their previous activity level in 12.4 ± 1.6 months; athletes treated with the on-field rehabilitation and isokinetic exercise program had faster recovery and an even earlier return to competition (10.6 ± 2.0 months).
Conclusion: For optimal results, autologous chondrocyte implantation rehabilitation should not only follow but also facilitate the process of graft maturation. Intensive rehabilitation may safely allow a faster return to competition and also influence positively the clinical outcome at medium-term follow-up.
Keywords
The management of chondral lesions is challenging because articular cartilage has limited healing potential because of its isolation from systemic regulation and lack of vessels and nerve supply.5,24,29
In the past 15 years, regenerative techniques such as first- and second-generation autologous chondrocyte implantation (ACI) have emerged as a valid therapeutic option, and recent studies2,3,18,28 suggest the durability of these treatments. Despite improvement in treatment for articular cartilage lesions, recovery may be prolonged, which greatly delays return to competitive sports.
An adequate rehabilitation program is crucial to optimize results of surgery for chondral defects. In fact, rehabilitation protocols may significantly improve cartilage repair and maturation by preventing chondrocyte death, enhancing functional recovery and the capacity to prevent the risk of reinjury. 7
Currently, evidence in favor of ACI rehabilitation is scarce, and few articles specifically address rehabilitation protocols. The rehabilitation strategies proposed focus on different progressive phases based on the current knowledge of the implant maturation process. The implant is most vulnerable during the initial stage. Currently there is a consensus of opinion that weightbearing should be restricted, avoiding peak compressive and shearing forces. 12 The most important milestone in this first stage is the progressive recovery of full weightbearing and walking.
Subsequently, the rehabilitation goal is not only to follow but also to facilitate the graft maturation process. Progressive enhancement of muscle strengthening and neuromuscular re-education and retaining are progressively intensified until return to functional daily activities. Low-impact sports and exercises such as cycling or swimming are then resumed within 6 months.
Because of the risk of damaging the implant with an inappropriate loading of immature tissue, return to high-impact activities such as soccer, rugby, volleyball, basketball, and martial arts is delayed until 12 to 18 months. 12 However, there is no established timeline for graft maturation. The inability to assess graft maturation and the lack of evidence for optimal rehabilitation creates reluctance to prescribe aggressive rehabilitation that may cause deleterious forces, leading to graft failure. Consequently, this fear and the lack of experienced therapists in this field can result in overcautious rehabilitation.
In the treatment of musculoskeletal injuries one of the most important developments has been the understanding that controlled early resumption of activity can promote restoration of function. 4 Many studies have demonstrated the positive influence of exercise and physical training on healing of articular cartilage defects and that physical training improves long-term results after cartilage regenerative treatments.19,23,29 Thus, optimal rehabilitation may improve cartilage healing and potentially “accelerate” return to the previous activity level. The rehabilitative challenge is to optimize, by a customized and progressive framework, the achievement of the goals without jeopardizing the graft vitality.
The purpose of this article was to analyze the short- and medium-term results and the resumption of sports in a group of 31 competitive athletes who underwent second-generation arthroscopic ACI (Hyalograft C, FAB, Abano Terme, Padova, Italy) and followed an intensive rehabilitation protocol. We also compared the clinical outcome at medium-term follow-up of this group with that of a group of 34 nonathletic patients, who were treated by the same surgeon during the same period, to assess the influence of an intensive rehabilitation program and sport activity on the results.
Materials and Methods
Patient Selection
Thirty-one competitive male athletes with International Cartilage Repair Society grade III-IV 13 cartilaginous lesions on the weightbearing surface of the medial or lateral femoral condyle or trochlea were enrolled in the study between 2000 and 2005 and prospectively evaluated every 12 months. The mean follow-up was 5 years, and all patients achieved a minimum of 3 years of follow-up. Clinical experimentation was approved by the local ethics committee, and all patients who gave their consent to participate and comply with the required postoperative rehabilitation regimen were included in the study.
The inclusion criteria of the study included athletes between 16 and 40 years old who had clinical symptoms, such as knee pain or swelling with grade III-IV chondral lesions of the femoral condyles or trochlea from 1.5 to 5.0 cm2. The exclusion criteria included chondral lesions greater than 5.0 cm2 or less than 1.5 cm2, patellar or tibial plateau chondral lesions, diffuse arthritis or bipolar (“kissing”) lesions, uncorrected axial deviation, or knee instability. The patients with ACL lesions underwent an associated surgical procedure for ACL reconstruction during the same surgical session with cartilage harvesting. Patients with infection, tumor, and metabolic and inflammatory conditions were also excluded from the study.
The mean age at surgery was 23.5 ± 5.7 years (range, 16–37 years). The most common cause of the defect was trauma (51.6% of the cases) followed by microtraumatic-degenerative findings (32.3% of cases), and osteochondritis dissecans (16.1% of cases). Twenty (64.5%) chondral lesions were located on the medial condyle, 8 (25.8%) on the lateral femoral condyle, and in 3 cases (9.7%) the lesion was located on the trochlea. The mean size of the defects was 2.2 ± 0.6 cm2 (range, 1.5-4 cm2).
Ten of the patients (32.2%) had undergone previous knee surgery. These operations included 3 ACL reconstructions, 1 patellar tendon suture, 1 loose body removal, 5 meniscectomies, and 4 cartilage arthroscopic repair operations, such as shaving or debridement, and osteochondral grafting (mosaicplasty) was performed in 1 patient. In 17 patients (54.8%) associated procedures were performed during the same operation: 13 ACL reconstructions, 1 posterior cruciate ligament reconstruction, 13 meniscectomies, and 1 loose body removal.
We also analyzed and compared the results obtained in a homogeneous group of 34 nonathletic patients treated during the same period by the same surgeons. This control group included all the nonathletic patients consecutively treated who matched the same inclusion criteria of the athlete group: male patients between 16 and 40 years old who had clinical symptoms, such as knee pain or swelling with grade III-IV chondral lesions of the femoral condyles or trochlea from 1.0 to 5.0 cm2. The groups were homogeneous regarding sex, age, etiology, previous surgery, defect size, and location. The only differences were noted regarding previous or associated ACL reconstruction and meniscectomy, which were more common in athletes (Table 1).
Comparison of the Characteristics of the Athlete and Control Groups a
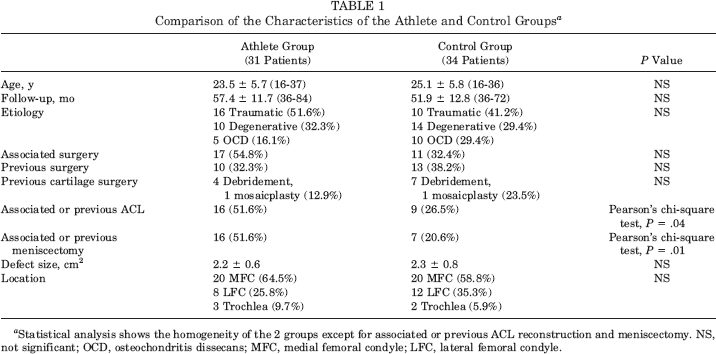
Statistical analysis shows the homogeneity of the 2 groups except for associated or previous ACL reconstruction and meniscectomy. NS, not significant; OCD, osteochondritis dissecans; MFC, medial femoral condyle; LFC, lateral femoral condyle.
Autologous Chondrocyte Implantation Hyalograft C Surgical Technique
The surgical technique described by Marcacci et al 22 was used. The treatment consists of 2 arthroscopic steps. The first procedure consists of a biopsy of healthy cartilage for autologous chondrocyte cell culture. A 150- to 200-mg cartilage specimen is taken from a non-weightbearing site on the articular surface (intercondylar notch) and sent to the processing center in a serum-free nutritional medium. Chondrocytes are seeded on a hyaluronic acid-based scaffold (Hyaff 11) to obtain the bioengineered tissue Hyalograft C.
After 6 weeks the second step is performed. A variable diameter (6.5–8.5 mm) delivery device with a sharp edge is used to evaluate the size of the defect to ensure complete coverage of the defect. 22 A circular area with regular margins for graft implantation is prepared with a specially designed cannulated low-profile drill. The delivery device is then filled with a hyaluronic acid patch, which is transported and placed in the prepared area. The graft is pushed out of the delivery device and precisely placed within the defect, where it remains tightly adhered to the subchondral bone. Because of the physical adhesive characteristics of the graft, no fibrin glue or sutures are used to fix the implant. The stability of implanted scaffolds is evaluated arthroscopically while bending the knee.
Rehabilitation Protocol
The rehabilitation protocol included 4 stages. The transition phase from one stage to the next was allowed when specific functional recovery and clinical outcome goals were reached.
Stage 1: Protection and Recovery of Walking (Week 0 to Week 10 or More)
The primary goal of the first stage was the progressive recovery of full weightbearing and walking. The strategy of this stage was focused on controlling pain and effusion, increasing range of motion, and reducing immobilization-induced muscle atrophy.
To protect the transplant, all the patients walked with crutches without weightbearing for 4 weeks. On the second postoperative day, continuous passive motion for 6 to 8 hours daily with 1 cycle per minute was performed to minimize the adverse effects of immobilization and to improve the healing process. The patients were also given an isometric and isotonic strengthening program to be performed at home during the first 2 weeks after surgery.
After 2 weeks, patients started supervised rehabilitation with 2 dedicated therapists, one in the swimming pool and one in the gym. Cryotherapy 3 times a day for 20 minutes was used for all patients. The details of the rehabilitation program are listed in Table 2.
Stage 1: Protection and Recovery of Walk a
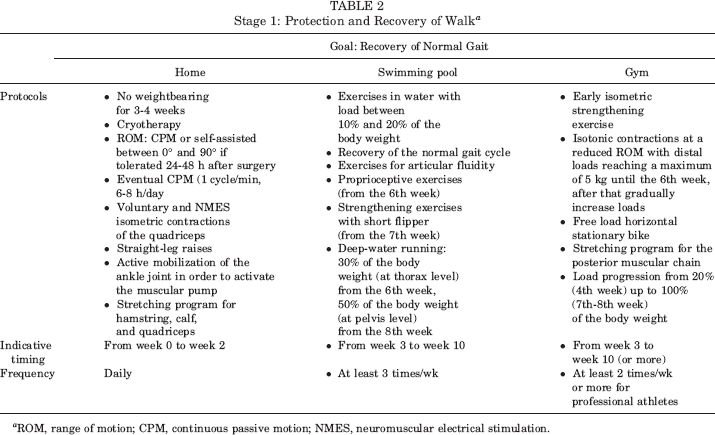
ROM, range of motion; CPM, continuous passive motion; NMES, neuromuscular electrical stimulation.
We allowed transition to the second stage after clinical examination showed no swelling, full knee extension, at least 120° of knee flexion, and ambulation with normal gait.
Stage 2: Transition and Recovery of Running (Week 11 to Week 30 or More)
The primary goal of the second stage was the return to normal running. The strategy of this stage was focused on strengthening exercises in open and closed kinetic chain selecting a pain-free range of motion (ROM), proprioceptive exercises, and aerobic training. After 16 weeks, running on a treadmill was allowed. The details of the rehabilitation program are listed in Table 3. The criteria for progression to the third stage of rehabilitation were no pain or swelling after 8- to 10-km/h running for 15 minutes, a good strength recovery compared with the contralateral limb evaluated with a clinical examination, and one-legged hop test less than 20% difference compared with the contralateral limb.
Stage 2: Transition and Recovery of Running a
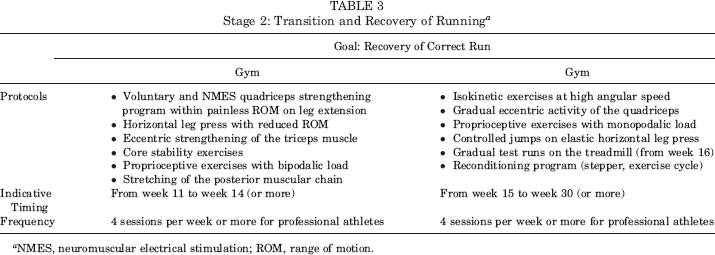
NMES, neuromuscular electrical stimulation; ROM, range of motion.
Stage 3: Maturation and Athletic Recovery (week 31 to week 40 or more)
The primary goal of the third stage was the recovery of sport-specific skills. The strategy of this stage was focused on eccentric strengthening exercises, advanced proprioceptive exercises, and a sport-specific reconditioning program (Table 4). Transition to the fourth stage was permitted when there was no pain and effusion during sport-specific drills and a complete endurance recovery according to the sport performed.
Stage 3: Maturation and Athletic Recovery
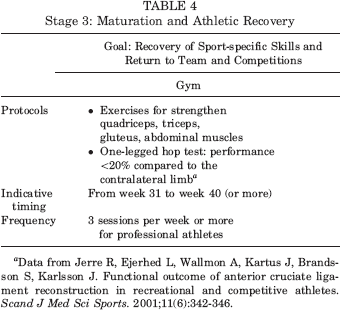
Data from Jerre R, Ejerhed L, Wallmon A, Kartus J, Brandsson S, Karlsson J. Functional outcome of anterior cruciate ligament reconstruction in recreational and competitive athletes. Scand J Med Sci Sports. 2001;11(6):342–346.
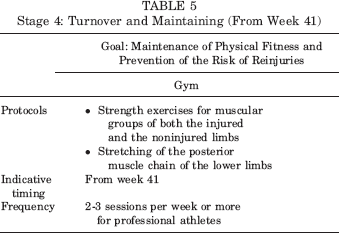
Stage 4: Turnover and Maintaining (From Week 41)
The final goal was bringing the athlete back to competition and preventing the risk of reinjury by progressively reproducing the movements the patient usually does in his own sport activity (Table 5).
Stage 4: Turnover and Maintaining (From Week 41)
The final phases (third and fourth) of rehabilitation preceded the return to sport on a specialized rehabilitation field, under the control of rehabilitation specialists. We call these phases on-field rehabilitation (OFR). The OFR consisted of specific exercises and drills performed under the supervision of rehabilitative personnel, before returning the player to his own sports team. Each OFR session lasted 90 minutes, from 3 to 5 days a week, and took place outdoors on a grass field or indoors on a synthetic field. The progression of each type of exercise followed the principles of strength training and increased functional demand with respect to the musculoskeletal and neurologic components involved in the recovery process.
On-field rehabilitation was divided into 5 phases, each characterized by well-defined, progressive, sport-specific exercises performed in a progressively larger area. During the first phase patients were submitted to global coordination and running exercises on a straight line including monopodalic jumps and landings. In the second phase, focus was placed on eccentric loads, running with stops and single-/double-foot leaps. Progressive changes in direction and speed while running, along with more intense aerobic workouts, characterized the third phase. In the fourth phase patients run backward and, for soccer players, kick the ball at increasing distances, aiming at a target. During the last phase, the focus was on improving each sport-specific pattern while simulating normal match conditions. The criteria for passing to a subsequent phase were exercises performed without discomfort and with good coordination, without fear of reinjury, and without appearance of pain, swelling, or decreased ROM.
The entire group of 31 competitive athletes completed all 4 phases of the rehabilitation protocol. From the third stage, 20 of the athletes reduced the number of gym sessions at our center and at the same time began a separate training program with their own sports team. The other 11 competitive athletes completed a specific isokinetic training and testing exercise program before the last phases of specialized on the field rehabilitation (Figure 1).

Isokinetic training and on-field rehabilitation.
Isokinetic training consisted of ascending/descending pyramidal strengthening sessions: 2 sets for each velocity (300, 250, 200, 180, 120, 90, 120, 180, 200, 250, 300 deg/s) starting with a high number of repetitions at high angular speed (20–25 repetitions at 300 deg/s) and ending with a few repetitions at low angular speed (10 repetitions at 90 deg/s). After at least 10 isokinetic training sessions, the isokinetic test, consisting of 4 repetitions at 90 deg/s and 20 repetitions at 180 deg/s, was performed. We allowed the patients to start the OFR only when the isokinetic testing revealed a quadriceps and hamstrings maximal peak torque of at least 80% compared with the contralateral leg.
The patients of the control group, nonathletic or athletic at an amateur level, completed the first phase of rehabilitation. Twenty-two patients were satisfied with the achievement of normal activities of daily living; the others, who participated in sports at amateur level, were instructed about the next phases but continued the physical recovery on their own.
Follow-up Evaluation
All patients were evaluated preoperatively, at 12 months, and at a mean of 5 years of follow-up. The clinical outcome of all patients was analyzed using the cartilage standard evaluation form as proposed by the International Cartilage Repair Society. 13 A functional knee test was performed by the surgeon according to the International Knee Documentation Committee (IKDC) Knee Examination Form. The lowest ratings in effusion, passive motion deficit, and ligament examination were used to determine the final functional grade of the knee (normal, nearly normal, abnormal, or severely abnormal). Patients were also asked to evaluate the state of their health using the Euro Quality of Life (EQ) visual analog scale (VAS). 13 Returning back to sports was evaluated with the Tegner Score30,31 at 2- and 5-year follow-up and compared with preoperative and preinjury levels. The time needed to return to previous activity level and to competition was also recorded.
The operation was considered to have failed if the patient needed a reoperation because of symptoms due to primary defects. For failures, the last clinical evaluation before reoperation was considered.
Statistical Methods
All continuous data are expressed in terms of mean ± standard deviation of the mean, for the ordinal data the median (25th-75th percentiles) was used. The Kolmogorov-Smirnov test was used to assess the normal distribution and the Levene test was used to investigate the homogeneity of variances.
One-way analysis of variance (ANOVA; normally distributed variables with homogeneous variances) or the Mann-Whitney test (not normally distributed variables or not homogeneous variances) was used to test hypotheses about differences between groups. The Pearson chi-square test, calculated by the exact method for small samples, was performed to investigate the relationships between grouping variables. The paired t test (normally distributed variables) or the Wilcoxon test (not normally distributed variables) was performed to test differences between follow-up times.
For all tests, P < .05 was considered significant. Statistical analysis was carried out by the Statistical Package for the Social Sciences software version 15.0 (SPSS Inc, Chicago, Illinois).
Results
No severe adverse events were observed during the treatment and follow-up periods. Both groups showed a statistically significant improvement of all clinical scores from preoperative to 1- and mean 5-year follow-up.
Group of Athletes
The IKDC objective score increased from 3.2% normal and 12.9% nearly normal knees before the operation (1A, 4B, 18C, and 8D) to 83.9% normal and 16.1% nearly normal knees (26A and 5B) at 12-month follow-up and showed a statistically significant improvement (Wilcoxon test, P < .001). The improvement remained stable over time, with no significant difference between 1 and 5 years (87.1% normal and 9.7% nearly normal knees: 27A, 3B, and 1C). There was a significant improvement in the IKDC subjective score and self-assessment of quality of life (EQ-VAS) from preoperative (44.4 ± 2.9 and 62.7 ± 15.9, respectively) to 1 year of follow-up (84.7 ± 11.7 and 85.2 ± 11.7, respectively; paired t test; P < .001). Further improvement was also observed in the evaluation at mean 5 years of follow-up, with a mean IKDC subjective score of 90.7 ± 11.7 (paired t test; P = .02) and an EQ-VAS value of 91.9 ± 9.7 (paired t test; P = .009).
The sport activity, which was evaluated using the Tegner score, showed a statistically significant improvement from preoperative level to 2 and 5 years of follow-up (paired t test; P < .001). The mean Tegner score was 8.3 ± 1.2 before the injuries, 2.1 ± 1.8 preoperatively, 7.6 ± 1.2 at 2 years of follow-up, and 7.3 ± 1.6 after 5 years. The new level of sport activity at 2 and 5 years was significantly lower with respect to the preinjury level (paired t test; P = .005 and P = .003, respectively); however, these results showed a statistically significant improvement (P < .001) from preoperative level to 2-year follow-up, and the results obtained were stable over time, with no significant difference between 2 and 5 years.
Control Group (Nonathletes)
Three patients had failed results: the first failure was at 2-year follow-up and the patient was treated by mosaicplasty, the second failure was at 4-year follow-up and the patient was treated by knee prosthesis, and the third failure was at 5-year follow-up and the patient was treated again by the matrix-induced ACI technique.
The IKDC objective score increased from 12.9% normal and 29.0% nearly normal knees before the operation (4A, 9B, 9C, and 12D) to 74.2% normal and 33.3% nearly normal knees (23A, 10B, and 1C) at 12-month follow-up and showed a statistically significant improvement (Wilcoxon test, P < .001). The improvements remained stable over time, with no significant difference between 1 and 5 years (77.4% normal and 25.8% nearly normal knees: 24A, 8B, and 2C). There was a significant improvement in the IKDC subjective score and EQ-VAS from preoperative (34.3 ± 14.2 and 56.9 ± 17.0, respectively) to 1 year of follow-up (71.3 ± 16.9 and 83.7 ± 14.9, respectively; paired t test, P < .001). A significant improvement with respect to the preoperative level was also observed in the evaluation at a mean 5 years of follow-up, with a mean IKDC subjective score of 75.7 ± 22.4 (paired t test, P < .001) and an EQ-VAS value of 82.8 ± 18.1 (paired t test, P < .001), and no statistically significant difference with the results obtained at 1 year (see Figure 2).
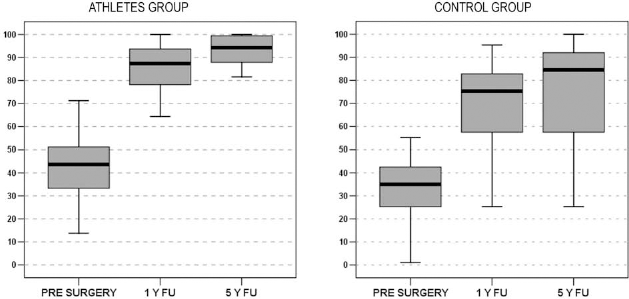
The International Knee Documentation Committee subjective evaluation in the group of athletes and in the control group preoperatively and at 1- and 5-year follow-up (FU).
The sport activity, which was evaluated using the Tegner score, showed a statistically significant improvement from preoperative level to 2- and 5-year follow-up (paired t test, P < .001). The mean Tegner score was 5.9 ± 1.3 before injury, 1.8 ± 1.3 preoperatively, 4.1 ± 2.2 at 2-year follow-up, and 4.3 ± 2.1 after 5 years. The new level of sport activity at 2 and 5 years was significantly lower with respect to the preinjury level (paired t test, P < .001); however, these results showed a statistically significant improvement (P < .001) from preoperative level to 2-year follow-up, and the results obtained were stable over time, with no significant difference between 2 and 5 years.
When comparing the athletic cohort with the nonathletic cohort, no statistically significant different results were obtained with the IKDC objective evaluation at 1 and 5 years and with EQ-VAS at 1 year, whereas in the athletic group a greater improvement was achieved at 5-year follow-up (1-way ANOVA, P = .037) in the EQ-VAS. Moreover, a statistically significantly greater improvement in the athletic group was detected with the IKDC subjective evaluation both at 12-month and 5-year follow-up (1-way ANOVA, P = .001 and P = .002, respectively) (Figure 2).
Further analysis was performed on the athletic cohort to understand the influence of rehabilitation on time to recover and clinical outcome. Among these 31 athletic patients, all followed the intensive rehabilitation protocol, but 11 were also treated with the isokinetic approach and OFR. We analyzed the 2 groups of athletes separately by comparing time to recover, return to previous activity level, and clinical outcome at 1- and 5-year follow-up. The groups were homogeneous regarding all the parameters analyzed (sex, age, etiology, previous or associated surgery, and defect size and location) (Table 6).
Comparison of the Characteristics of the Athletes Treated With the Isokinetic and On-Field Rehabilitation (OFR) Program and the Other Group of Athletes a
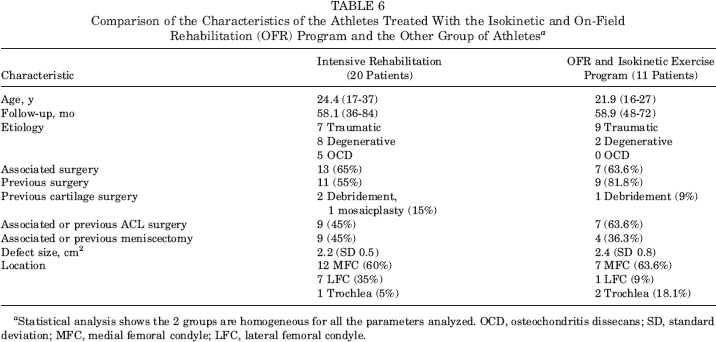
Statistical analysis shows the 2 groups are homogeneous for all the parameters analyzed. OCD, osteochondritis dissecans; SD, standard deviation; MFC, medial femoral condyle; LFC, lateral femoral condyle.
When analyzing the resumption of sports activity, 80.6% of the athletic cohort returned to previous activity level, with no statistically significant difference between the 2 subgroups. The same results were observed in all the scores evaluated at 1- and 5-year follow-up; however, a significant difference was obtained in the time to recover. In fact, patients treated with the isokinetic approach and OFR showed a faster recovery (Mann-Whitney test, P = .024) of previous activity level (8.6 ± 1.7 months) and an earlier return (Mann-Whitney test, P = .039) to competition (10.6 ± 2.0 months) with respect to the other group of athletes (10.6 ± 1.7 and 12.4 ± 1.6, respectively) (Figure 3).

Resumption of sports activity.
Discussion
The number of symptomatic articular cartilage lesions has increased because of the marked increase in sports participation and greater emphasis on physical activity in all age groups; patients’ expectations about recovery have risen as well.1,20 The ultimate goal of cartilage reconstruction is the restoration of the original preinjury level of function, and the time taken to recover is also important.
The rehabilitation program, a critical component of the treatment of cartilage lesions, facilitates graft healing and influences the success of autologous cartilage implantation. Because maturation of the graft takes some time, initial restriction of weightbearing has the beneficial effect of minimizing forces that may compress or delaminate the implant. However, the graft is protected by muscular control and strength, which absorb the forces by acting through the joint surface. Thus, after the initial phase when the graft is most vulnerable, the rehabilitation protocol plays an important role in enhancing the ability of the graft to endure the compressive cyclic loads during functional activities. Weightbearing and joint movement are necessary for tissue homeostasis, by ensuring nutrition and maintaining biomechanical properties of normal cartilage. It would therefore seem a reasonable assumption that mechanical stimuli are also important for the maturation process.
In vitro studies have shown that mechanical forces affect chondrocyte biosynthesis and gene expression. 19 Compression might have a regulatory role on chondrocyte differentiation, and cartilage extracellular matrix synthesis and degradation can be modulated by mechanical events. 9 Static load decreases matrix production; application of cyclic loads enhances matrix synthesis. 25 Although too intensive physical activity or immobilization can cause cartilage degeneration, optimal mechanical stimuli have a positive influence on the healing of chondral lesions. Exercised horses and dogs have significantly thicker, stiffer cartilage compared with nonexercised animals.10,16,17 Also, studies in humans14,15 confirm the role of physical activity in optimum cartilage development: inactive children show a 22% to 25% lower cartilage volume compared with active children. These results are of particular significance because the repair tissue after ACI is also exposed to a remodeling process and thus, as in young developing cartilage, susceptible to mechanical stimuli.
Despite these data, the observation of biopsies26,27 suggests that cartilage regeneration after ACI is a long process. Remodeling of the graft continues for at least 18 months and the graft becomes more hyaline over time. The length of this process has significant implications for the timing of the rehabilitation schedule. The return to high-impact activities is therefore cautiously allowed only at 12 months up to 18 months. 12
Most of the articles about ACI rehabilitation address the first-generation procedure,3,12,19,23,28 which consists of implanting a suspension of cultured autologous chondrocytes beneath a periosteal flap. The good clinical results reported with this technique, however, have to be weighed against its disadvantages, including the potential leakage of chondrocytes from defects, the dedifferentiation of a cellular phenotype, the inhomogeneous distribution of cells, and the risk of periosteal complications. This technique is performed via either open orminiarthrotomy, which produces greater surgical trauma and, consequently, a higher risk of joint stiffness and arthrofibrosis. All of these problems contribute to prolonged rehabilitation for the standard ACI technique.
The development of second-generation ACI,2,15,18,21 which involves tissue engineering technology to create a cartilage-like tissue in a 3-dimensional culture system, addresses all concerns related to the cell culture and the surgical technique. The bioengineered tissue significantly reduces the inherent fragility of the ACI graft during the early postoperative stage and accelerates patient recovery.
Following this rationale Ebert et al, 8 in a randomized controlled study, compared traditional versus accelerated approaches to postoperative rehabilitation following matrix-induced ACI, and showed the possibility to speed up the recovery of normal gait function and reduce knee pain without graft complications. Moreover, the evolution of an arthroscopic approach, resulting in lower surgical trauma and mechanoreceptor disruption, reduces surgical morbidity and has a great impact on rehabilitation, thus enabling a further acceleration of functional recovery.
Accelerating rehabilitation after second-generation ACI may therefore be safely achieved without damaging the graft. The safety of the rehabilitation program is ensured by a goal-oriented protocol with objective criteria, rather than specific timetables, guiding clinical decisions. Progression is criterion-based rather than time-based, and the transition from one stage to the next is allowed when the goals of the stage are achieved without pain or swelling.
In this context, the isokinetic method improves training and monitoring of the rehabilitation progress, which more closely follows graft maturation.
The accommodating resistance during isokinetic training allows the patients to work safely without stressing the graft. Moreover, this kind of training, using both verbal and visual feedback 6 motivates patients to achieve their maximum potential. Finally, the isokinetic machine enables periodic testing of the patient's strength, which is important in evaluating improvement. 11
It is also important to ensure that patients treated with isokinetic rehabilitation complete a full rehabilitation program, including specific sport resumption (OFR). A subgroup of 11 patients treated with isokinetic rehabilitation completed the rehabilitation protocol on the field. We proposed some criteria to start OFR, the course to follow, and some functional outcomes for monitoring. The functional goals we considered for starting OFR were a deficit of less than 20% in isokinetic maximal peak torque of the treated limb for both knee extension and knee flexion and the ability to run on a treadmill for more than 10 minutes at 8 km/h without the onset of pain, swelling, or decreased ROM. Patients treated with the isokinetic rehabilitation and OFR showed a faster return to previous activity (8.6 months, SD 1.7) and an earlier return to competition (10.6 ± 2.0 months) with respect to the other group of athletes (10.6 ± 1.7 and 12.4 ± 1.6, respectively). We can hypothesize that the observed differences may be due to our rehabilitation approach including OFR, isokinetic training, and joint medical and rehabilitation specialist supervision, 13 thus helping to make a decision on when the athlete should safely return to competition.
Currently, there is no evidence that may be used to determine the optimal type, frequency, intensity, and timing of exercises for rehabilitation after ACI. However, it has already been shown that mechanical forces are chondrogenesis-promoting factors, and the postoperative protocol can optimize the results. Other authors 23 have demonstrated that functional outcome, time to recover, and return to sport are related to sport activity level, and that physical training carried out for at least 2 years after surgery can further improve long-term results after ACI. 19
The results of this study support the hypothesis that intensive rehabilitation may facilitate graft maturation and safely allow return to sports. In this study, 80.6% of the highly competitive athletes returned to previous activity level within 1 year, and a strict and intensive rehabilitation program may shorten the time to 10 months. Longer-term follow-up to assess whether intensive rehabilitation would jeopardize the clinical outcomes demonstrated that the results obtainedat 1 year were maintained at the 5-year follow-up. More importantly, the scores were significantly higher in the athletic group compared with the control group.
Limitations of our study include the lack of having 2 equal athletic cohorts, one treated with intensive rehabilitation and the other with less intensive rehabilitation. In fact, the patients in the nonathletic group were not as motivated as the athletes. A randomized controlled trial with longer term follow-up will certainly provide more useful information, but such a study may be difficult to perform.
Conclusion
The postoperative rehabilitation program is crucial to optimizing results of surgery for chondral defects. Rehabilitation should not only follow but also facilitate the process of graft maturation. Competitive athletes who undergo second-generation arthroscopic ACI can optimize the results and shorten the recovery time through an intensive rehabilitation protocol. Intensive rehabilitation may safely allow a faster return to competition.