
Abstract
Background: Revision ulnar collateral ligament reconstruction remains a challenging problem. The objective of this study was to biomechanically evaluate an ulnar collateral ligament reconstruction technique using a suspension button fixation technique that can be used even in the case of ulnar cortical bone loss.
Hypothesis: An ulnar suspension fixation technique for ulnar collateral ligament reconstruction can restore elbow kinematics and demonstrate failure strength comparable to that of currently available techniques.
Study Design: Controlled laboratory study.
Methods: Nine pairs of cadaveric elbows were dissected free of soft tissue and potted. After simulating ulnar cortical bone loss, ulnar collateral ligament reconstruction was performed in 1 elbow of each pair using palmaris longus autograft and a 30-mm RetroButton suspended from the far (lateralmost) ulnar cortex. A docking technique was used for humeral fixation of the graft. Elbow valgus angle was quantified using a Microscribe 3DLX digitizer at multiple elbow flexion angles. Valgus angle was measured with the ulnar collateral ligament intact, transected, and reconstructed. In addition, load-to-failure testing was performed in 1 elbow of each pair.
Results: Release of the ulnar collateral ligament caused a significant increase in valgus angle at each flexion angle tested (P < .002). Reconstructed elbows demonstrated no significant differences in valgus angle from the intact elbow at all flexion angles tested. Load-to-failure tests showed that reconstructed elbows had an ultimate torque (10.3 ± 5.7 N·m) significantly less than intact elbows (26.4 ± 10.6 N·m) (P = .001).
Conclusion: Ulnar collateral ligament reconstruction using a suspension button fixation technique reliably restored elbow kinematics to the intact state. Load-to-failure testing demonstrated comparable fixation strength to several historic controls of primary reconstruction techniques despite the simulated ulnar cortical bone loss.
Clinical Relevance: Ulnar collateral ligament reconstruction using a suspension button fixation technique can be considered in the case of ulnar cortical bone loss in a primary or revision setting.
The fact that the anterior bundle of the ulnar collateral ligament (UCL) is the primary restraint to valgus forces at the elbow has been well established in the orthopaedic literature. 13 High-level overhead throwing athletes can generate valgus forces estimated in excess of 120 N·m, causing repetitive stress to the UCL. 23 Injury to the UCL can lead to pain, instability, and the inability to successfully throw at preinjury levels.2,24
Ulnar collateral ligament reconstruction was first reported by Jobe et al. 11 Their original technique used a palmaris longus tendon graft weaved through bone tunnels in the sublime tubercle of the ulna and medial epicondyle of the humerus. Since then, several alternative fixation techniques have been reported.1,3,6,9,12,15,18 However, to our knowledge, all techniques of UCL reconstruction described require intact ulnar cortical bone. Ulnar cortical bone loss can occur when inadvertent breakage of the bone bridge occurs while drilling the ulnar tunnels or in a revision surgery setting with bone loss contributing to a failed first reconstruction. It has been estimated that 2% of UCL reconstructions fail because of a retear (J. Andrews, unpublished data, 2008).
Revision UCL reconstruction remains a challenging problem, 7 especially in the face of ulnar cortical bone loss at the sublime tubercle. The objective of this study was to biomechanically evaluate a UCL reconstruction technique using a suspension button fixation technique that could be used for revision UCL reconstruction.
The hypothesis of this study is that a UCL reconstruction using a suspension button fixation technique can restore elbow kinematics despite medial ulnar cortical bone loss and demonstrate failure loads comparable to that of currently available techniques of primary reconstruction.
Methods
Specimen Preparation
Nine pairs of fresh-frozen, cadaveric elbow specimens were obtained from 9 human cadavers (average age 45 years, range 23-60; 5 males, 4 females) and dissected free of soft tissue. Care was taken to preserve the capsule, ligaments, and muscle about each elbow. The palmaris longus tendon was harvested using a standard surgical technique. Osteotomies of the humerus, radius, and ulna were performed 14 cm from the joint line to facilitate potting of the specimen with plaster of Paris in polyvinyl chloride piping. One elbow from each cadaveric donor was randomly selected for resection and then reconstruction of the UCL, followed by kinematics and biomechanics testing. The contralateral elbow from the same cadaveric donor was used as a control for biomechanics testing.
Kinematic Testing
The forearm was fixed in neutral rotation and the specimen placed in a testing apparatus that held the humerus in a position parallel to the floor. The radius was placed inferior, the ulna superior, and the gravity valgus position was calculated using a previously published method employing a digitizer (MicroScribe, Immersion Corporation, San Jose, California) to obtain kinematic data.14,16
The elbow valgus angle was calculated using 3 points in space along the forearm relative to 3 points along the humerus in multiple flexion angles with the medial UCL intact, deficient, and reconstructed. The deep fibers of the anterior bundle of the medial UCL were sharply dissected off the humeral attachment site to create the ligament-insufficient condition, resulting in at least 3 mm of joint-space opening with the elbow at 30° of flexion.
Ligament Reconstruction Technique
The UCL reconstruction was performed using the palmaris longus tendons from the cadaveric specimens. The palmaris longus tendon was harvested before dissection of the soft tissues. All of our matched pair cadaveric specimens had at least 1 palmaris longus tendon available for harvesting and use in our reconstruction. The width of each tendon was standardized to 5 mm before placing the tendon on a tissue tensioner set to 15 lb of force to precondition the graft.
A 3.2-mm drill bit was used to create the “conventional Tommy John” tunnels in the ulna at the level of the sublime tubercle as described by Jobe et al. 11 The bone bridge of our ulnar tunnel was then intentionally broken with the drill bit to simulate ulnar cortical bone loss from either failed prior surgery or intraoperative tunnel fracture. A 3-mm spade-tip drill bit (Arthrex, Naples, Florida) was placed at the ulnar footprint of the UCL on the sublime tubercle to center the socket, and was directed at 30° in both the sagittal and coronal planes (Figure 1) to create a hole in the lateral (radial) ulnar cortex. A 5-mm cannulated reamer (Arthrex) was then used over the spade-tip guidewire to create our ulnar socket. The humeral tunnel was then drilled using a 4.5-mm drill bit into the medialmost tip of our medial epicondyle with a 30° cephalad tilt. Smaller medially, as well as anteriorly, located drill holes were placed into the medial epicondyle in a caudal direction to converge with the humeral tunnel for use in docking the graft and securing it over a bone bridge. 18
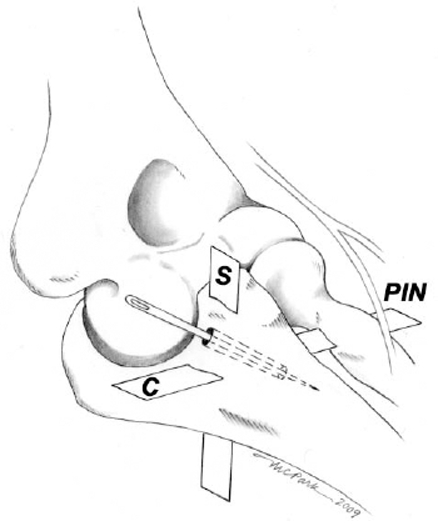
Orientation of the spade-tip drill bit and Keith needle used for ulnar fixation with location of the posterior interosseous nerve (PIN). The drill bit is oriented approximately 30° in both the coronal (C) and sagittal (S) planes.
The palmaris longus tendon graft was then removed from the tissue tensioner and doubled lengthwise. The looped end of the doubled tendon graft was sutured with #2 FiberWire (Arthrex) in a whipstitch fashion to a distance of 1 cm for use in the ulnar tunnel. The remaining 2 free ends of the graft were also whipstitched with separate threads of a #0 FiberWire for use at the humeral tunnel (Figure 2).
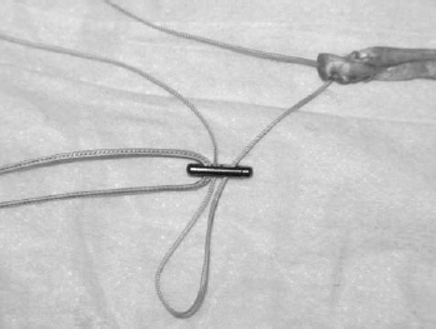
Palmaris longus graft preparation. A 0 Vicryl suture is passed through the distal end of the RetroButton for use as a pull-stitch. A #2 FiberWire is whipstitched through the single-limbed (doubled-over) portion of the graft, and a single limb of the #2 FiberWire stitch is passed through both holes in the RetroButton before RetroButton passage.
A Keith needle was then inserted through the ulnar tunnel from an ulnar to radial direction and allowed to pierce the skin of the dorsal-radial forearm. The Keith needle was advanced and a 0 Vicryl suture (Ethicon, Somerville, New Jersey) was doubled; the looped end was passed back out the medial cortex of our ulnar tunnel. A 30-mm RetroButton (Arthrex) was then threaded onto the single-limbed side of our graft using 1 end of the #2 FiberWire whipstitch, and an additional 0 Vicryl pull-stitch was looped through the distal hole in the button as well. Both limbs of the pull-stitch were inserted into the passed 0 Vicryl suture and force was applied to the pull-stitch in a vector parallel to the ulnar tunnel to pull the RetroButton through the lateral (radial) cortex of the ulna. A differential force was then applied to the 2 ends of the pull-stitch to force the RetroButton to lie flat against the surface of the ulnar cortex before removing the pull-stitch. After seating of the button, the graft was pulled into the ulnar socket and held under tension. An arthroscopic knot-pusher was then inserted into the ulnar tunnel from the medial cortex to securely tie down the RetroButton loop within the socket using 5 alternating half-hitch knots (Figure 3). Lastly, a Hewson suture passer was used to pass each remaining free limb of the graft through the humeral tunnel and the 2 suture ends were tied over the humeral bone bridge to tension the graft with the elbow in 70° of flexion.8,20,21
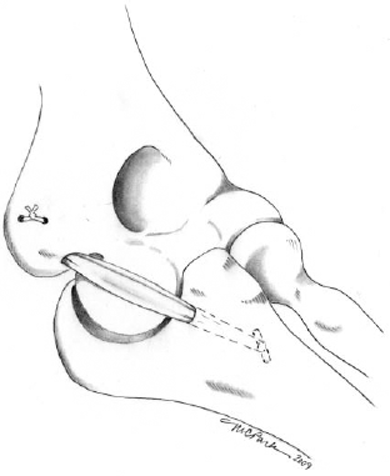
Schematic for the ulnar collateral ligament reconstruction construct.
Failure Testing
After reconstruction and kinematic testing, the elbows were mounted in an Instron materials testing machine (Instron Corp, Canton, Massachusetts) for biomechanical analyses. We used a newly designed sliding jig that allowed for Instron cross-head movement along rails in the long axis of the forearm to generate torque with a higher degree of freedom than with previous protocols. 1 The elbow was tested at 70° of elbow flexion with the humerus fixed and forearm left free to gravity. 1 The elbow was preloaded with 1 N·m of valgus before load to failure testing at a rate of 50% strain/s. Ultimate torque was measured and stiffness of the native or reconstructed ligament calculated using the corresponding torque-angular displacement curve.
Statistical Methods
Paired t tests with a Bonferroni correction for multiple comparisons were used for statistical analysis. Independent variables for kinematics testing included elbow flexion angle and UCL condition (intact, deficient, and reconstructed). The measured dependent variable was elbow valgus angle. Student t tests were performed on the matched elbow pairs for comparison of the ultimate torque and stiffness.
Results
Release of the UCL ligament caused a significant increase in valgus angle at each flexion angle tested (P < .002). When comparing UCL reconstruction to the UCL-deficient condition, the reconstruction significantly reduced the valgus angle at 0°, 30°, and 60° of elbow flexion (P < .05); while at 90° and 120° of elbow flexion, the valgus angle was reduced, but the difference did not reach statistical significance (P = .11 and P = .2, respectively). When comparing the reconstructed elbows to the intact condition, we found no significant differences in valgus angle at all elbow flexion angles tested (P > .4) (Table 1).
Elbow Valgus Angle a
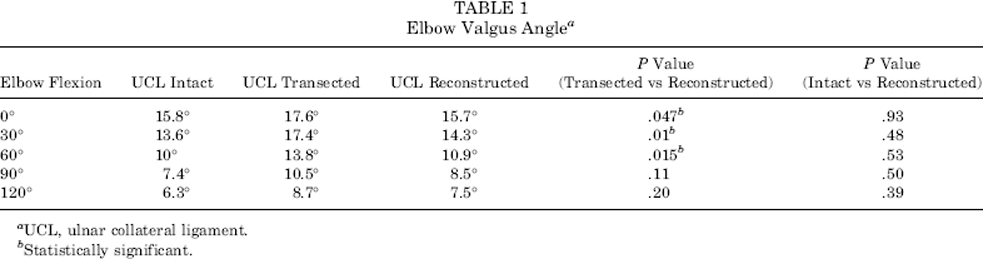
UCL, ulnar collateral ligament.
Statistically significant.
Load-to-failure tests showed that reconstructed elbows had an average stiffness of 1.1 ± 0.4 N·m/deg and an ultimate torque of 10.3 ± 5.7 N·m, which was significantly less (P = .0007 and P = .001, respectively) than intact elbows (2.4 ± 0.9 N·m/deg and 26.4 ± 10.6 N·m, respectively) (Table 2). There were no significant differences in angular displacement or energy absorbed to failure (P = .9 and P = .08, respectively).
Mode of Failure to Valgus Load for Native UCL and Reconstructed UCL a

UCL, ulnar collateral ligament.
The most common mode of failure was related to the humeral fixation, with 5 suture failures and 1 humeral bone tunnel failure. There were 2 specimen failures at the ulnar side (1 ulnar bone socket fracture and 1 suture failure), and 1 specimen with a midsubstance graft rupture (Table 2).
Discussion
There is little published in the orthopaedic literature on revision UCL reconstruction. Dines et al 7 reported on a case series of 15 collegiate and professional baseball players. The majority of patients underwent revision using the Jobe technique, but 3 of the 15 were reconstructed using a docking technique on the humeral side and an interference screw for ulnar fixation (DANE TJ [hybrid] technique). While this latter technique reduces the number of ulnar tunnels necessary for secure fixation, it does not completely obviate the need for intact ulnar cortical bone at the sublime tubercle. In contrast, using a suspension button method for ulnar fixation technically does not require this cortical bone at the tubercle, and requires few additional steps beyond that of the DANE TJ technique. Required steps are passage of a Keith needle through the ulnar socket and seating of the button on the far ulnar cortex. A potential neurovascular structure at risk with Keith needle passage is the posterior interosseous nerve (Figure 1). The humeral-sided fixation for both techniques is identical, and a low complication rate has been reported with the DANE TJ method of reconstruction, even in a revision setting. 7
The current study supports the use of a new technique for ulnar-sided fixation that can be used in UCL reconstruction surgery in the case of ulnar cortical bone loss. Elbow kinematics were restored to that of the intact state, and failure testing demonstrated comparable fixation loads to several historic controls, despite the simulated ulnar cortical bone loss.
The restoration of elbow kinematics is important in the overhead-throwing athlete as considerable valgus stress is placed on the elbow over a wide range of motion.4,9 We found a statistically significant increase in the elbow valgus angle with release of the ligament at all elbow flexion angles tested, validating our experimental model. We were able to show a statistically significant reduction in the valgus angle from the UCL-deficient state at 0°, 30°, and 60° of elbow flexion; while at 90° and 120° of elbow flexion, valgus angles were reduced, but did not reach statistical significance. We hypothesize that we did not achieve statistical significance in restoring the valgus angle at these elbow flexion angles due to the increased contribution of the posterior bundle of the UCL at higher elbow flexion angles. In addition, several studies have shown that the anterior bundle of the UCL may not experience significant stress with higher elbow flexion angles.3,17,19 More importantly, in all elbow flexion angles tested, we found no statistically significant difference in elbow valgus angle when comparing the reconstructed elbows to the intact state. Demonstrating the restoration of normal kinematics at the time of reconstruction is critical, especially in a cadaveric study where the effect of healing cannot be measured.
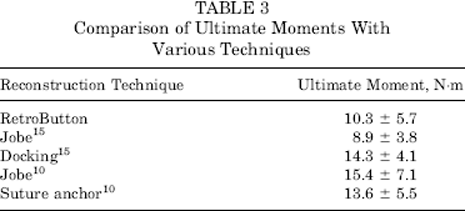
This new method of using a cortical suspension button technique for ulnar-sided fixation also demonstrated failure loads similar to several historic controls of primary reconstruction techniques (Table 3).10,15 Our ultimate failure load of the intact UCL was found to be 26.0 N·m, which is similar to that reported by Hechtman et al 10 and Paletta et al, 15 who found failure loads of 22.7 N·m and 18.8 N·m, respectively. Notably, Ahmad et al 1 found the ultimate failure load of the intact UCL under valgus stress to be 34.0 N·m. As our study was performed in the same laboratory with a similar experimental protocol and similarly aged specimens, we can attribute the difference to the use of the previously described sliding jig that allowed for application of torque with additional degrees of freedom than did the one used in the previous study. 1 A recent study also reported a lesser ultimate failure load of an intact UCL (14.9 N·m) with a 4 degrees of freedom testing apparatus. 5 However, a higher ultimate moment or testing apparatus with additional degrees of freedom may not necessarily translate into a clinically superior method of UCL reconstruction or biomechanical testing, as most postoperative rehabilitation protocols typically protect the elbow from substantial valgus forces for a period of 9 to 12 months. 22 For this same reason, we believe that restoration of elbow kinematics is more important than demonstrating an ultimate load to failure similar to the native UCL.
Comparison of Ultimate Moments With Various Techniques
Armstrong et al 3 compared the biomechanical characteristics of 4 different UCL reconstruction techniques. One of the techniques they tested included the use of an EndoButton (Smith & Nephew Endoscopy, Mansfield, Massachusetts) for ulnar cortical fixation. Our study differs from theirs in that they used a fixed loop-length EndoButton. Their EndoButton had a continuous loop length of 20 mm that in some cases limited the amount of palmaris longus graft that filled their ulnar tunnel. 3 Our technique does not rely on a fixed loop-length device and allows maximization of the amount of palmaris longus graft that can be placed inside the ulnar socket. Although this factor was not tested by our study, we hypothesize that this may have favorable implications for healing biology while obviating the need to fabricate suspension buttons with different fixed loop lengths.
Additionally, Armstrong et al 3 tested their constructs as a means of primary UCL reconstruction. Our study differs in that we simulated ulnar cortical bone loss, as might be found in a revision surgery setting, before performing our reconstruction. Despite this simulated bone loss, we were able to restore elbow kinematics to the intact state. This suggests that our technique may be applicable in a primary reconstruction situation while preserving the ease of appropriately tensioning a single-stranded graft. 3
The majority of the failures during the load-to-failure testing occurred at the humeral side. This is also consistent with 3 other biomechanical studies that used the docking technique for humeral-sided fixation.3,12,15
The limitations of our study are common to other published cadaveric studies on UCL reconstruction. These include investigation of our reconstruction at time 0 without the ability to account for any healing. We were also unable to account for dynamic factors such as active muscle contraction, which has been shown to account for valgus stability 16 ; however, normal kinematics were restored after reconstruction. In addition, our cadaveric specimens were on average older than the typical candidate for UCL reconstruction, but similar to other studies.1,15
In conclusion, UCL reconstruction using a suspension button fixation technique can be considered even in the case of ulnar cortical bone loss in a primary or revision setting.