
Abstract
Background: Patellar tendinopathy is characterized by pathologic abnormalities. Heavy slow resistance training (HSR) is effective in the management of patellar tendinopathy, but the underlying functional mechanisms remain elusive.
Purpose: To investigate fibril morphology and mechanical properties in patellar tendinopathy and the effect of HSR on these properties.
Study Design: Cohort study; Level of evidence, 2.
Methods: Eight male patients with patellar tendinopathy completed 12 weeks of HSR. Nine healthy subjects served as controls. Assessments were conducted at baseline and at 12 weeks. Patients assessed symptoms/function and maximal tendon pain during activity. Tendon biopsy samples were analyzed for fibril density, volume fraction, and mean fibril area. Tendon mechanical properties were assessed using force and ultrasonography samplings.
Results: Patients improved in symptoms/function (P = .02) and maximal tendon pain during activity (P = .008). Stiffness and modulus of control and tendinopathy tendons were similar at baseline. Stiffness remained unaffected in control tendons (3487 ± 392 to 3157 ± 327 N/mm, P = .57) but declined in tendinopathic tendons at 12 weeks (3185 ± 187 to 2701 ± 201 N/mm, P = .04). At baseline, fibril volume fraction was equal, fibril density smaller (P = .03), and mean fibril area tended to be higher in tendinopathy versus controls (P = .07). Fibril morphology remained unchanged in controls but fibril density increased (70% ± 18%, P = .02) and fibril mean area decreased (—26% ± 21%, P = .04) in tendinopathic tendons after HSR.
Conclusion: Fibril morphology is abnormal in tendinopathy, but tendon mechanical properties are not. Clinical improvements after HSR were associated with changes in fibril morphology toward normal fibril density and mean fibril area. Heavy slow resistance training improved the clinical outcome of patellar tendinopathy, and these improvements were associated with normalization of fibril morphology, most likely due to a production of new fibrils.
Keywords
Tendinopathy is the generic term for painful and disabling tendon overload injuries. 23 Tendinopathy is a highly prevalent condition characterized by extensive pathologic tissue changes.5,24,35 These pathologic changes include increased water content,7,35 increased amounts of proteoglycans and glycosaminoglycans,7,35 increased cross-link concentrations,2,18 neovascularization, 5 and fascicular disorganization.24,28 Most healthy tendons have a bimodal distribution of the fibrillar diameter with the space between the larger fibrils being filled by smaller-diameter fibrils, thus allowing a high collagen content but maintaining the flexibility of the tissue. 29 However, ruptured, grafted, and tenotomized tendons have been shown to contain fewer large-size fibrils and more small-size fibrils compared with healthy tendons.3,25,39 Whether tendinopathy is related to changes in fibril morphology remains to be established.
We have recently found that heavy slow resistance (HSR) training may be effective in the management of patellar tendinopathy (PT), 18 but the underlying mechanisms of this therapeutic regimen remain to be established. Mechanical loading has previously been shown to yield decreased,26,32 increased, 26 or unchanged 31 fibril diameters in animal models, but the effect of loading on the fibrillar morphology of injured tendons has not been investigated.
Tendon collagen fibrils are the basic force-transducing units of the tendon, 33 and the morphologic properties of the tendon fibrils have been suggested to determine the mechanical properties and function of the tendon.30,33 It has been suggested that tendons with a higher proportion of larger collagen fibrils have a greater tensile strength because of a higher density of intermolecular cross-links29,31 and a positive relationship between fibril diameter and tendon stiffness has previously been observed. 4 Surprisingly, we have recently shown that the mechanical properties (stiffness and modulus) of the patellar tendon in vivo were unaffected by tendinopathy. 18 These mechanical measurements in vivo were of course performed at subfailure force levels, which preclude any conclusions regarding the maximal/failure strength of the tendon. Accordingly, the present study aimed to investigate the effect of 12 weeks of HSR on fibril morphology and whole-tendon mechanical properties in patellar tendons affected with chronic tendinopathy.
Materials and Methods
Subjects
Eight male patients with PT were included in the study. This PT group had a mean age of 32.9 ± 3.5 years, mean height of 187 ± 3 cm, mean weight of 84 ± 3 kg, mean symptom period of 15 ± 3 months, and a mean activity level of 6.6 ± 1.6 hours/week. The patient sample for this study was not the same as the one participating in our previous study. 18 Only patients with a pain duration longer than 3 months were included to secure a chronic condition. An experienced physician (M. Kj.) confirmed the diagnosis based on defined clinical and ultrasonographic findings, including tendon pain during activity, tendon swelling, hypoechoic areas, and the presence of color Doppler signal within the hypoechoic areas. 18 In all patients the sonographic-revealed tendon abnormalities were located at the proximal tendon region.
Nine age- and activity level-matched men with healthy patellar tendons (no clinical symptoms or ultrasound abnormalities) were included in the study as healthy control subjects. This control group had a mean age of 31.5 ± 3.3 years, mean height of 185 ± 2 cm, mean weight of 85 ± 3 kg, and mean activity level of 5.5 ± 1.0 hours/week. The control subjects did not undertake any interventions during the investigation period. This group was included to control for possible effects of repeated biopsies. Subjects were excluded if any confounding diagnoses were revealed. Exclusion criteria were previous corticosteroid injections to the patellar tendon, and previous knee surgery, arthritis, or diabetes.
The study complied with the Declaration of Helsinki and was approved by the local ethics committee for medical research (protocol number KF 256131). All subjects gave their written informed consent to participate.
Heavy Slow Resistance Training
After baseline assessments, the PT patients undertook 12 weeks of HSR as previously described in detail. 18 In brief, 3 weekly sessions were conducted, with each session consisting of 3 bilateral knee extension exercises: squat, leg press, and hack squat. Subjects completed 4 sets of each exercise with a 2- to 3-minute hiatus between sets. The repetitions/loads were 15 repetition maximum (RM), week 1; 12 RM, weeks 2 to 3; 10 RM, weeks 4 to 5; 8 RM, weeks 6 to 8; and 6 RM, weeks 9 to 12. All exercises were performed from complete extension to 90° of knee flexion and back again. This training regimen subsequently implemented both eccentric and concentric contractions. Subjects were instructed to spend 3 seconds completing each of the eccentric and concentric phases respectively (ie, 6 seconds per repetition). Pain during exercises was accepted, but pain and discomfort were not to increase after cessation of training. During the 12-week treatment period, patients were allowed to perform sporting activities if these could be performed with only light discomfort (maximal pain on visual analog scale [VAS], score of 30). During the 12-week period control subjects were asked to maintain their normal activity level.
Clinical Evaluation
The PT patients completed a written Victorian Institute of Sport Assessment-patellar (VISA-p) questionnaire to assess symptoms, function, and the ability to participate in sports. 40 Also, the maximal tendon pain during preferred sporting activity was indicated on a 100-mm VAS. Subjects completed the VAS and VISA-p questionnaire with no investigator assistance at 0 and 12 weeks.
Muscle and Tendon Structural Properties
Both groups were assessed for muscle and tendon structural properties at baseline and at 12 weeks (before the tendon biopsy). In the PT group, muscle and tendon structural properties were assessed in the affected legs. In the control group, these assessments were randomly obtained from either the right or left knee. Anatomical cross-sectional area of the quadriceps femoris muscle was assessed 20 cm proximal from the tibia plateau by T1-weighted SE MRI (General Electric, Signa Horizon LX 1.5 Tesla, GE Healthcare Diagnostic Imaging, Broendby, Denmark). 19 Patellar midtendon cross-sectional area and tendon length were also determined with MRI as previously described.18,19
Assessment of tendon cross-sectional area at the proximal tendon region (pathologic area) was not possible because of indistinct tendon borders of this area on the MR images. Tendon and muscle structural properties were manually outlined using the software program Osiris 4.19 (Digital Imaging Unit, Geneva, Switzerland; http://www.sim.hcuge.ch/osiris/). The mean value of 3 measurements of the same image was used for analysis. The MRI investigator was blinded with regard to subject group.
Patellar Tendon Biopsies
At baseline and at 12 weeks all subjects from both groups had patellar tendon biopsies. A detailed description of this procedure has been reported previously. 18 In brief, a Bard MAGNUM Biopsy Instrument (C.R. Bard, Inc, Covington, Georgia) with a 14-gauge disposable core biopsy needle was used. After sterilization the skin was injected with local anesthetic (lidocaine, 1%) and a 3- to 5-mm long skin incision was created using a scalpel. Subsequently, the biopsy needle was inserted through this incision onto the tendon surface at an approximately 30° angle and fired, securing a sample of approximately 8 mg. In PT patients, tendon biopsy samples were obtained from the tendon region displaying an abnormality (proximal posterior tendon region) of the affected tendon. In the control group, the patellar tendon biopsy sample was obtained from the proximal tendon region of the same leg at which muscle and tendon structural properties were assessed. In both groups, prebiopsy and postbiopsy samples were taken from the same tendon. At 12 weeks great care was taken to avoid obtaining tissue from the previous biopsy site. Biopsy samples were immediately fixed in 2% glutaraldehyde in 0.05 M sodium phosphate buffer (pH 7.2) and subsequently stored at 4°C until further analysis.
Transmission Electron Microscopy
After 3 rinses in 0.15 M sodium cacodylate buffer (pH 7.2) the specimens were fixed in 1% OsO4 in 0.15 M sodium cacodylate buffer (pH 7.2) for 2 hours. The specimens were subsequently dehydrated in ethanol, transferred to propylene oxide, and embedded in EPON resin 828/862 mix (Hexion Specialty Chemicals, Rotterdam, The Netherlands) according to standard procedures. After this, sections were cut using a Reichert-Jung Ultracut E microtome. Semi-thin sections, for preanalytic evaluation of the samples, were stained with toluidine blue and visualized (digital images) using a Nikon Coolpix 990 (Nikon Nordic ABl, København, S. Denmark) mounted on a Zeiss Photomicroscope (Brock & Michelsen A/S, Birkerød, Denmark) equipped with crossable Polaroids, a calibrated rotating stage, and a plan apo 40/0.95 objective lens. When proper condition and orientation of the sample within the EPON block were confirmed, ultra-thin sections were cut and collected on a 1-hole copper grid with Formvar supporting membranes and stained with uranyl acetate and lead citrate. These sections were examined using a Philips CM 100 transmission electron microscope (TEM; Philips Healthcare, Best, The Netherlands) equipped with a Kodak slow-scan camera (Kodak A/S, Brøndby, Denmark) and operated at an accelerating voltage of 80 kV. From each biopsy sample cross-section, a simple random sample of 10 digitized TEM images was obtained (Figure 1).
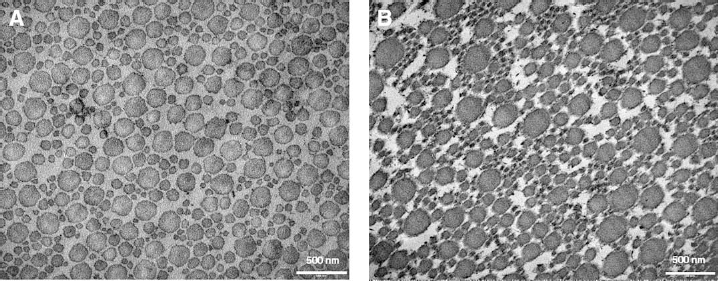
A representative cross-sectional transmission electron microscopy image of 2 tendon biopsy samples from the same patellar tendinopathy subject before (A) and after (B) HSR. Notice the comparable volume fraction but varying density and fibril diameter distribution between A and B. The presample (A) is dominated by relatively few but large-diameter fibrils. The postsample (B) is dominated by more but smaller-diameter fibrils.
Stereology
The stereologic analyses of the TEM images were completed on a computer monitor onto which the digitized TEM images were merged with a graphic representation of the stereologic test system (C.A.S.T.-grid software, The International Stereology Centre at Olympus, Denmark). The collagen fibrils were counted and measured at a magnification of 210 000. Each TEM image was examined with 16 uniformly positioned points and 16 uniformly positioned unbiased counting frames, 10 each of an area of 0.0426 μm2, in a fixed position relative to the image. The described procedure ensures that all locations of the biopsy sample cross-section have an equal probability of being sampled and counted. A complete tessellation of unbiased counting frames ensures that each profile is sampled only once. The counting frames covered 15% of the TEM image area, and the TEM images covered approximately 0.5% percent of the biopsy sample cross-section. On average, 215 fibrils (range, 121-431) were analyzed per cross-section. Fibril area was calculated from measurements of fibril diameter. Fibril diameter was measured as the largest diameter perpendicular to the longest axis of each fibril cross-section, thereby eliminating the influence of sectioning angle. The fibril density was expressed as the absolute number of fibrils per square micrometer and the fibril volume fraction states the area occupied by fibrils within the sample area. A single experienced and blinded investigator (J.L.) performed all stereologic analyses.
Patellar Tendon Mechanical Properties
All subjects from both groups had their patellar tendon mechanical properties assessed at baseline and at 12 weeks (before the tendon biopsy). The PT patients had their injured tendon evaluated. Details and reliability of this method have been reported previously.13,18 Briefly, synchronized values of patellar tendon elongation (ΔL), obtained from ultrasound recordings, and patellar tendon forces (ΔF) were sampled. All trials were analyzed to a greatest common force for all subjects (4350 N). Force-deformation curves were fitted to a second- or third-order polynomial fit that in all cases exceeded R2 = .95. Tendon stiffness (ΔF/ΔL) and modulus (Δstress/Δstrain) were calculated in the final 20% of the curves. The mean of the 3 contractions yielding the greatest force was used for analysis. Analysis was performed in an investigator-blinded fashion.
Statistical Analysis
All data are presented as means ± standard error of the mean. Statistical analyses were performed using GraphPad Prism version 4.01 (GraphPad Software, La Jolla, California). The Mann-Whitney U test was used to analyze for differences between the 2 groups. The Wilcoxon matched-pairs signed-ranks test was used to analyze for changes within each group from baseline to 12 weeks. All analyses were 2-tailed. Significance was considered as P < .05.
Results
Subject Characteristics and Clinical Findings
No differences in age, height, weight, or activity level were found between the PT patients and control subjects. In the PT group, 12 weeks of HSR resulted in a 27% ± 7% improvement in the VISA-p score (from 57 ± 3 to 82 ± 7, P = .02) and a 36% ± 5% improvement in VAS (59 ± 6 to 23 ± 5, P = .008). All patients improved in VAS score (before/after difference range, -17 to -61) during the intervention period. Regarding the individual change in Visa-p, the scores of 5 subjects increased, that of 2 subjects remained unchanged, and that of 1 deteriorated.
Structural and Functional Properties of Muscle and Tendon
The muscle and tendon structural and mechanical properties are listed in Table 1. There were no differences between the 2 groups in tendon structural and mechanical properties at baseline. There was a significant increase in quadriceps cross-sectional area (7% ± 1%, P = .008) and peak knee extension moment (10% ± 2%, P = .03) after HSR in the PT group. However, the peak knee extension moment and quadriceps cross-sectional area remained unchanged in the control group. In the PT group, patellar tendon stiffness decreased significantly by 9% ± 6% from 3185 ± 187 to 2701 ±201 N/mm (P = .04) following 12 weeks of HSR (Table 1), but remained unchanged in the control group (3157 ± 327 N/mm at 12 weeks). Also, modulus tended to decrease in the PT group from 1.8 ± 0.1 at baseline to 1.5 ± 0.2 at 12 weeks (P = .15), whereas it remained unchanged in the control group (1.7 ± 0.2 GPa at 12 weeks).
Tendon Structural and Mechanical Properties a
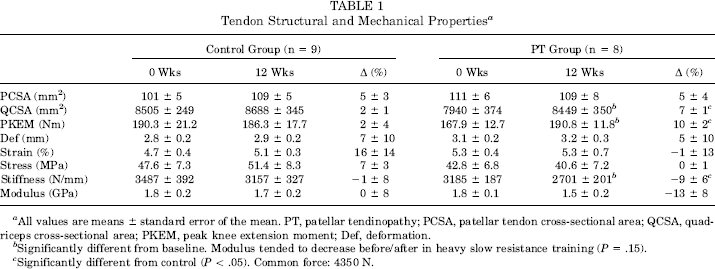
All values are means ± standard error of the mean. PT, patellar tendinopathy; PCSA, patellar tendon cross-sectional area; QCSA, quadriceps cross-sectional area; PKEM, peak knee extension moment; Def, deformation.
Significantly different from baseline. Modulus tended to decrease before/after in heavy slow resistance training (P = .15).
Significantly different from control (P < .05). Common force: 4350 N.
Tendon Fibril Morphology
Tendon fibril properties are listed in Table 2 and depicted in Figure 2. At baseline, the fibril volume fraction was equal in the control and PT groups. However, fibril density was significantly smaller in PT versus control at baseline (50.0 ± 4.8 vs 79.5 ± 10.2%, P = .03) and mean fibril area tended to be higher (9352 ± 1289 vs 7709 ± 1114 nm2, P = .07) in the PT group compared with controls. Also, at baseline the number of fibrils per square micrometer in the 60- to 70-nm fibril diameter interval tended to be higher in controls versus the PT group (P = .18) (Figure 2A). Fibril density, fibril volume fraction, mean fibril area, and fibril size distribution remained unchanged from baseline to 12 weeks in the control group (Table 1 and Figure 2B). However, in the PT group, 12 weeks of HSR did not affect volume fraction significantly but induced a significant 70% ± 18% (P = .008) increase in fibril density and a significant 26% ± 2% (P = .04) decrease in mean fibril area (Table 2). Also, 12 weeks of HSR in the PT group resulted in significant changes in fibril diameter distribution in that the number of fibrils per square micrometer in the 50- to 60-nm and 60- to 70-nm fibril diameter intervals increased significantly (P = .02 and P = .04, respectively) (Figure 2C). At 12 weeks there were no differences in density (P = .7), volume fraction (P = .37), or mean fibril area (P = .29) between controls and the PT patients.
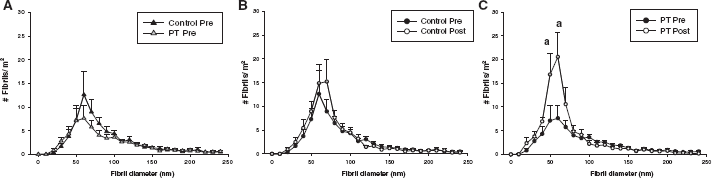
Absolute patellar tendon fibril diameter distribution. A, fibril diameter distribution of the control and patellar tendinopathy (PT) group at baseline. B, fibril diameter distribution of the control and PT groups at 12 weeks. C, fibril diameter distribution for the PT group at baseline and at 12 weeks. Con, control group; PT, PT group. Values are means ± standard error. aSignificantly-different from baseline.
Tendon Fibril Properties a
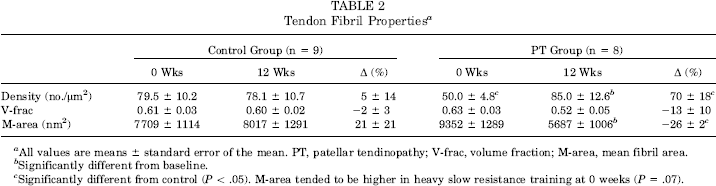
All values are means ± standard error of the mean. PT, patellar tendinopathy; V-frac, volume fraction; M-area, mean fibril area.
Significantly different from baseline.
Significantly different from control (P < .05). M-area tended to be higher in heavy slow resistance training at 0 weeks (P = .07).
Discussion
These data show that patellar tendons affected by tendinopathy display identical fibril volume fraction but a lower fibril density and a tendency toward a higher mean fibril area compared with healthy tendons. Interestingly, the good clinical effect of HSR in PT was associated with significant changes in fibril morphology, such that fibril density increased and mean fibril area greatly decreased, thus approaching the fibril morphology of healthy tendons.
Tendinopathy is characterized by numerous pathologic abnormalities, including increased water content,7,35 increased amounts of proteoglycans and glycosaminoglycans,7,35 increased cross-link concentrations,2,18 neovascularization, 5 and fascicular disorganization. 24 The present study expands on this list by including low fibril density and a high mean fibril area to the associated tendinopathic changes. To the best of our knowledge, this study is the first to assess fibril morphology of tendinopathic tendons. Both tendon ruptures and tendinopathies are associated with comprehensive pathologic tissue changes,16,24 suggesting a common pathologic basis. However, in contrast to the present findings, ruptured Achilles tendons have been reported to be dominated by small-diameter fibrils in the area of the rupture. 25 Also, the mechanical properties of tendinopathic tendons were not dissimilar to those of healthy ones, supporting the notion that tendinopathic tendon abnormalities do not weaken the tissue.8,20 Last, in contrast to tendinopathies, the majority of tendon ruptures are asymptomatic before the rupture.14,17,25 Collectively these findings suggest that the pathologic changes in tendinopathic tendons diverge from those of ruptured tendons. Also, the present findings suggest that the tendon mechanical properties seem unaffected by tendinopathy, although it has to be emphasized that the measurements were performed to subfailure loadings for obvious reasons.
The underlying cause of the altered tendon fibril morphology in tendinopathy is unclear. However, several authors have hypothesized that tendinopathy may arise from microrupture damage and subsequent stress deprivation of adjacent tenocytes, which eventually will elicit a catabolic tenocyte response.1,11 Therefore, our findings of decreased mean fibril diameter, which mainly arose from a lack of small- to intermediate-size fibrils (Figure 2A) could be explained by a reduced formation of new fibrils due to local tenocyte stress deprivation. Also, tendinopathy is associated with various disturbances of the extracellular matrix composition,22,35 and because extracellular matrix components have been shown to play important roles in fibrillogenesis and lateral fibrillar growth,15,38 the altered fibril morphology may result from such matrix alterations. Last, we cannot exclude the possibility that diverging fibril morphology could be a predisposition to the development of tendinopathy. A firm establishment of the tendinopathy etiology will have great clinical perspectives, and we can only encourage such future studies.
In agreement with our previous findings, 18 12 weeks of HSR significantly improved the clinical condition of PT. The present improvements in VISA-p and VAS scores are in line with previous studies on exercise-based management of PT.9,34 Although the application of loading-based therapies in tendinopathy management is far from new, the underlying effect mechanisms have not been established. Clinical recovery from tendinopathy is associated with a normalization of ultrasound-visualized tendon structure and reductions of tendon swelling and vascularization.18,27 In the present study, tendinopathic patellar tendons displayed a low fibril density and a large mean fibril area. Twelve weeks of HSR somewhat counteracted this altered fibril morphology by increasing fibril density and reducing the mean fibril area by increasing the presence of small-size fibrils. Subsequently, at 12 weeks there were no statistical differences in fibril morphology between the control and PT groups. Thus, this study supports an association between clinical outcome and extracellular matrix normalization following loading-based therapy for tendinopathy.
Several animal studies have reported unaltered fibril volume fraction, but significantly increased fibril density and reduced mean fibril area following increased loading,26,32 and the present findings extend this to a human model. Most likely such changes occur by a de novo synthesis/formation of new and thinner fibrils3,39 or by longitudinal splitting of existing fibrils. 26 We found that HSR increased the fibril density and decreased the mean fibril area by increasing the presence of small-diameter fibrils (50-70 nm), suiting well within the notion of an increased formation of new fibrils and/or longitudinal splitting of existing fibrils.
The present study demonstrated identical fibril volume fraction and tendon cross-sectional area in tendinopathic compared with healthy tendons, indicating that the total tendon tensile material is not reduced with tendinopathy despite the abnormalities, which corroborates previous findings on collagen content. 18 Others have reported minor reductions in tendon collagen content with tendinopathy.2,36 Those studies are, however, somewhat compromised by preceding corticosteroid injections, which can reduce tendon collagen content.18,42 Because the collagen fibrils are the basic force-transmitting unit of tendons,6,33 they are generally believed to determine tendon mechanical properties.4,30 Traditionally, bigger fibril diameters have been associated with increased strength and stiffness because of an increased cross-link capacity.4,12,25,30,31 However, recent studies show that fibril volume fraction, not fibril diameter, predicts tendon mechanical properties.21,37 Therefore, the unaltered amount of tensile material (ie, fibril volume fraction and tendon cross-sectional area) may explain why tendon mechanical properties were unaffected by the tendinopathy. At the same time, however, tendon stiffness and modulus decreased concomitantly with the reduction in mean fibril area following 12 weeks of HSR. Unfortunately, a quantification of collagen cross-links was not possible in the present study because of limitations in the size and weight of the biopsy samples. We have previously reported that pentosidine cross-links decrease in conjunction with an increased matrix turnover after 12 weeks of HSR in PT. 18 Thus, it seems possible that the reduction in mechanical stiffness observed in the PT group can be explained by reduced amounts of cross-links due to increased matrix turnover and production of new fibrils. From a more clinical point of view, the unaltered mechanical properties of tendinopathic tendons reported in this and other studies8,20 may explain why many athletes suffering from tendinopathy are able to perform at a high level. Albeit speculative, the only suppressing performance factor with tendinopathy may be the tendon pain.
The present study includes a few methodologic considerations. Although great attention was given to obtaining abnormal tendon tissue from the patients, we cannot rule out that healthy tissue was occasionally sampled. For example, regional differences in fibril density, volume fraction, and mean fibril diameter within the rabbit patellar tendon have been reported. 41 However, the difference in fibril morphology between control and PT tendons in the present study appears robust. Furthermore, we applied a strict standardized procedure of biopsy sampling and therefore do not expect differences in sampling location to contribute to the observed differences in fibril morphology.
In summary, we have demonstrated altered tendon fibril morphology in PT including a reduced fibril density and a strong tendency toward a higher mean fibril area. In addition, the good clinical effect of heavy resistance training was accompanied by changes in fibril morphology, perhaps indicative of more new fibrils. Last, tendinopathy did not affect fibril volume fraction, which may explain why tendon mechanical properties were unaffected by tendinopathy.