
Abstract
Purpose
The purpose of the study was to compare frequency of meniscal repair to partial meniscectomy in patients undergoing anterior cruciate ligament reconstruction using the American Board of Orthopaedic Surgeons (ABOS) database.
Hypotheses
(1) Practice patterns are similar with respect to geographic region. (2) Surgeons with fellowship training perform more meniscal repairs compared with general orthopaedic practitioners. (3) Younger patients are more likely to be treated with meniscal repair at the time of anterior cruciate ligament reconstruction. (4) The frequency of meniscal repair in conjunction with anterior cruciate ligament reconstruction has increased over time.
Study Design
Cross-sectional study; Level of evidence, 3.
Methods
Information was extracted from the ABOS database from 2002 orthopaedic surgeons who sat for the part II examination from 2003 to 2007. The database was queried for all patients who underwent anterior cruciate ligament reconstruction (Current Procedural Terminology [CPT] code 29888) without or with meniscectomy (CPT 29881) or meniscal repair (CPT 29882). Factors affecting meniscal surgery that were investigated included patient age, geographic region of practice, fellowship training, and declared subspecialty of the surgeon.
Results
On average there were 52000 cases per year registered in the ABOS database, approximately 1700 of whom underwent anterior cruciate ligament reconstruction. Meniscal repair was most frequently performed in the Southwest region (18.6%, P < .001) and least frequently in the Northwest region (11.3%, P < .001). Combined anterior cruciate ligament reconstruction and meniscal repair was performed significantly more often by fellowship-trained surgeons (17%) than by surgeons with other fellowship training (12%) or no fellowship training (12%, P < .001) and in patients younger than age 25 years (19%) compared with those age 40 years and older (8%, P < .001). Meniscal repair was performed in 13.9% of anterior cruciate ligament reconstructions in 2003 and in 16.4% of anterior cruciate ligament reconstructions in 2007 (P < .05).
Conclusion
Combined anterior cruciate ligament reconstruction with meniscal repair was more frequent for younger patients and by surgeons with sports fellowship training. Concomitant meniscal repair is performed by fellowship-trained surgeons in this study in only 18% of anterior cruciate ligament reconstructions.
The incidence of concomitant meniscal tears in anterior cruciate ligament (ACL) injuries is reported to be approximately 55% to 65%.11,12,14,23,26,38,39 Increased time from injury of the ACL leads to increased prevalence and complexity of meniscal tears. 19 Therefore, repair of a torn meniscus associated with ACL injury is recommended whenever possible. Repair is best accomplished with inside-out, vertical mattress sutures utilizing an accessory posterior incision.3,4,9,10,17,31,41
The medial meniscus has an important role as a secondary restraint to anterior tibial translation and can therefore protect the ACL graft.1,22,27,31 Long-term clinical outcome studies have shown significantly better clinical outcomes when the menisci are intact or repaired at the time of ACL reconstruction.11,34 Detrimental effects on articular cartilage integrity and joint function have been observed when concomitant meniscectomy was performed at the time of ACL reconstruction.36,42
The combination of ACL injury and partial meniscectomy is known to lead to radiographic osteoarthritis (OA) at intermediate-term and long-term follow-up (30 years).24,28–30,35 Positive predictive factors for developing OA are obesity (body mass index >30), a degenerative meniscal tear, partial resection of the lateral meniscus, and intraoperative cartilage changes. 15
There are several reasons concomitant meniscal repair at the time of ACL reconstruction seems appropriate: (1) the combined effect of instability and meniscal injury leads to OA, 24 (2) chronic meniscal injury makes repair less likely, 15 and (3) the likelihood of successful meniscal repair is enhanced when combined with ACL reconstruction. 11
The purpose of this study was to document the frequency of concomitant meniscectomy and meniscal repair in patients undergoing ACL reconstruction using the American Board of Orthopaedic Surgeons (ABOS) database. We hypothesized that (1) practice patterns are similar with respect to geographic region, (2) surgeons with sports fellowship training perform more meniscal repairs than other fellowship-trained surgeons or surgeons without fellowship training, (3) meniscal repair is performed more frequently for younger patients, and (4) the frequency of meniscal repair has increased over time from 2003 to 2007.
Methods
The ABOS regulates certification in orthopaedic surgery in the United States. Upon completion of an accredited orthopaedic surgery residency, candidates take a written part I examination. After successful completion of the part I examination as well as 24 months of practice, candidates are eligible to take the part II examination. The part II examination consists of a practice-based oral examination. Seventy percent of candidates take the part II examination of ABOS within the first 2 years in practice.
Data from each of the surgical procedures during a defined 6-month period are submitted by the candidates in preparation for the part II examination. The hospital or surgical center reviews the case list before submission to the ABOS and the ABOS validates the case list with the hospitals. The cases are entered into a secure database maintained by the ABOS. Information collected includes the date of the procedure, location of the candidate's practice, ICD-9 (International Classification of Diseases, 9th Revision) diagnosis codes, CPT (Current Procedural Terminology) codes, patient age and gender, as well as surgical and medical complications.
Medical and surgical complications are also entered into the database. Complications were grouped into subgroups for analysis. The subgroup “procedure-related complications” included hemorrhage, wound dehiscence, wound infection, fracture, implant failure or fracture, surgical procedure intervention (unplanned return to the operating room), and surgical unspecified.
For the purpose of this study, the ABOS database was searched for ICD-9 codes 844.2 (ACL rupture), 836.1 (lateral meniscal tear, current), and 836.0 (medial meniscal tear, current) for the years 2003 through 2007. The database was queried to identify all patients who underwent ACL reconstruction (CPT code 29888). For each patient it was determined if concomitant meniscectomy (CPT code 29881) or meniscal repair (CPT 29882) was performed. Thus, we were able to determine the number of patients undergoing ACL reconstruction with no meniscal surgery, meniscectomy, and meniscal repair. The ABOS database did not include information on the time from injury to surgery, type or location of meniscal tear, or method of meniscal repair, thus we were unable to analyze these factors.
Candidates applying for the part II examination of the ABOS were informed that the data that they submit as part of the voluntary process of board certification may be used for research and that the form that they sign during application for the examination gives permission to use the case list data for that purpose.
Data Analysis
We began data analysis by determining the proportion of individuals undergoing ACL reconstruction without concomitant meniscal surgery, ACL reconstruction with concomitant meniscectomy, and ACL reconstruction with concomitant meniscal repair. Chi-square tests for proportions were used to identify differences in the proportion of meniscectomy and meniscal repair by geographic region, patient age, fellowship training status, declared subspecialty, and year of examination. To evaluate how geographic region affects performance of meniscal repair and meniscectomy, the United States were separated into 6 geographic regions based on the 10 trauma regions of the American College of Surgeons as previously described by Anglen and Weinstein. 2 To determine differences in meniscectomy or meniscal repair by patient age, patients were grouped into 3 age categories: younger than 25 years, 25 to 39 years of age, or 40 and older. Fellowship training status was categorized as sports medicine fellowship, other fellowship, or no fellowship training. The declared subspecialty was categorized as sports, other subspecialty, or general practice. The alpha level was set at .05 for all statistical tests.
Results
From 2003 to 2007, the case lists that were submitted by the candidates included 8342 patients with an ACL tear (ICD-9 code 844.2), for an average of 1668 ACL tears per year. A total of 2002 candidates submitted case lists in the 5-year period. Thus candidates performed an average of 4 ACL reconstructions during the 6-month data collection period.
Across all geographic regions of the United States, isolated ACL reconstruction was performed 51% of the time. Of the remaining 4088 patients undergoing ACL reconstruction, 2836 (34%) underwent concomitant partial meniscectomy and 1251 (15%) underwent meniscal repair.
Anterior cruciate ligament reconstruction and concomitant meniscal surgery varied by geographic region (P < .001). Meniscal repair was most frequently performed in the Southwest region (18.6%, P < .001) and least frequently in the Northwest region (11.3%, P < .001; Figure 1). Meniscectomy was most frequently performed in the Southeast region (35.4%) and least frequently performed in the Midwest (31.2%); however, these differences were not significant from the other regions.
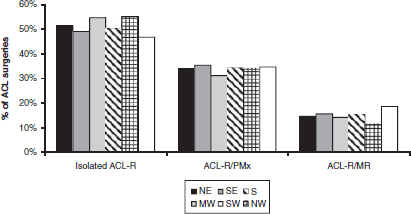
Proportion of isolated anterior cruciate ligament reconstruction (ACL-R), ACL-R and partial meniscectomy (PMx), and ACL-R and meniscal repair (MR) between 2003 and 2007 separated by geographic regions. MW = Midwest (Iowa, Kansas, Nebraska, Missouri, Illinois, Indiana, Michigan, Minnesota, Ohio, Wisconsin); NE = Northeast (Connecticut, Massachusetts, Maine, New Hampshire, Rhode Island, Vermont, New Jersey, New York, Delaware, Maryland, Pennsylvania, Washington, DC, Puerto Rico); NW = Northwest (Alaska, Idaho, Oregon, Washington, Montana, North Dakota, South Dakota, Utah, Wyoming); S = South (Alabama, Kentucky, Mississippi, Tennessee, Arkansas, Louisiana, Texas); SE = Southeast (Virginia, West Virginia, North Carolina, South Carolina, Florida, Georgia); and SW = Southwest (New Mexico, Oklahoma, Arizona, California, Hawaii, Nevada, Colorado).
Age also affected performance of meniscal surgery during ACL reconstruction (P < .001) (Figure 2). In this series, 4002 patients were younger than 25 years (46.2%), 3267 (37.8%) were between 25 and 39 years of age, and 1385 patients were 40 years and older (16.0%). Meniscal repair was performed in 746 individuals (18.6%) undergoing ACL reconstruction who were under the age of 25 years, compared with 452 (13.8%) in those between the ages of 25 to 39 years and 112 (8.1%) age 40 years or older. The difference in meniscal repair between those younger than 25 years and those 25 years of age and older was significant (P < .001). Conversely, meniscectomy was more commonly performed in those between the ages of 25 to 39 years (n = 1189, 36.4%) and 40 years and older (n = 521, 37.6%) than in those younger than 25 years (n = 1215, 30.4%) (P < .001).
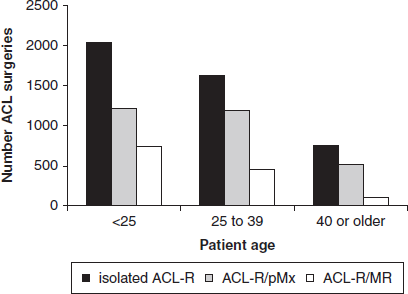
Total number of cases performed on patients younger than 25 years than of age, between 25 and 39 years, and older than age 40 years. ACL-R, anterior cruciate ligament reconstruction; pMx, partial meniscectomy; MR, meniscal repair.
Meniscal repair was significantly more likely when the ACL tear was treated by a sports medicine fellowship–trained surgeon (16.6%) than by a general orthopaedic surgeon (11.7%) or other fellowship-trained surgeon (12.0%) (P < .001). Sports medicine fellowship–trained surgeons performed combined ACL reconstruction and partial meniscectomy (n = 2000) twice as often as combined ACL reconstruction and meniscal repair (n = 983). In contrast, surgeons with other fellowship training and general orthopaedic surgeons were almost 3 times more likely to perform combined ACL reconstruction and partial meniscectomy (n = 925) when compared with combined ACL reconstruction and meniscal repair (n = 327) (Figure 3).
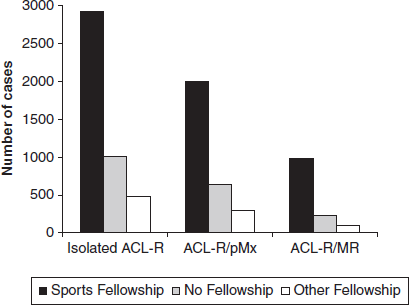
Total number of cases performed by surgeons with sports medicine fellowship training, no fellowship training, and other fellowship training. ACL-R, anterior cruciate ligament reconstruction; pMx, partial meniscectomy; MR, meniscal repair.
Case volume of the surgeon did not influence the percentage of concomitant meniscal repairs. Meniscal repairs were performed in 15.0%, 15.5%, 14.8%, and 15.7% of ACL reconstructions by surgeons with a volume of less than 5, 6 to 10, 11 to 25, and >26 ACL reconstructions per year, respectively (P > .05).
Meniscal surgery associated with ACL reconstruction was also related to the surgeon's declared area of subspecialty (P < .001). Meniscal repair was more likely when surgery was performed by a sports orthopaedic surgeon (18.0%) than when performed by a surgeon with another declared subspecialty (14.8%) or general orthopaedic surgeon (13.6%; P < .001).
In this study, meniscal surgery varied over time from 2003 to 2007 (P = .034). Meniscal repair was performed in 13.9% of the individuals undergoing ACL reconstruction in 2003 and in 16.4% of the individuals undergoing ACL reconstruction in 2007; however, these differences were not significant (P = .10 and P = .11, respectively; Figure 4).
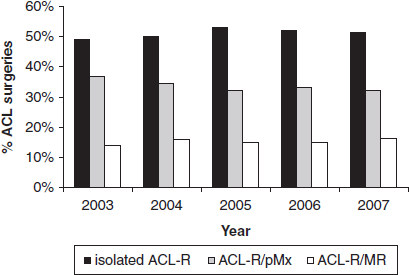
Percentage of cases performed between 2003 and 2007. ACL-R, anterior cruciate ligament reconstruction; pMx, partial meniscectomy; MR, meniscal repair.
Nonspecified surgical complications occurred in 3.2% of the individuals undergoing combined ACL reconstruction and meniscal repair, compared with 1.9% in combined ACL reconstruction and partial meniscectomy, and 2.2% in those undergoing ACL reconstruction without concomitant meniscal surgery (P = .02). Wound dehiscence occurred in 0.4% of the individuals undergoing combined ACL reconstruction and meniscal repair, compared with 0.2% in those undergoing combined ACL reconstruction and partial meniscectomy and 0.6% in those undergoing isolated ACL reconstruction (P = .03). There were no differences in the remainder of medical and surgical complications between groups (Table 1).
Medical and Surgical Complications by Type and Year a
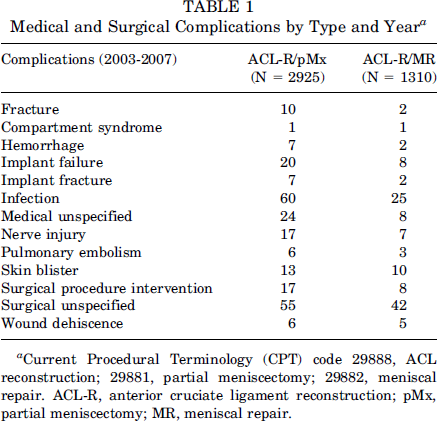
Current Procedural Terminology (CPT) code 29888, ACL reconstruction; 29881, partial meniscectomy; 29882, meniscal repair. ACL-R, anterior cruciate ligament reconstruction; pMx, partial meniscectomy; MR, meniscal repair.
Discussion
For this study, we searched a large database of the ABOS consisting of >2000 surgeons and >8000 ACL reconstructions. Half of the patients in this study received meniscal surgery; 16%, meniscal repairs; and 34%, meniscectomies. Because there was no information in the ABOS database on meniscal tears left in situ, the true number of isolated ACL reconstructions is unknown from the data of this study. The results of this study partially supported our hypotheses. Specifically, meniscal repair was more commonly performed during ACL reconstruction in younger patients and when performed by an orthopaedic surgeon who completed a sports fellowship and who declares sports as his or her subspecialty practice area. There was no consistent trend in performance of meniscal repair over time; however, concomitant meniscectomy was performed more frequently in 2003 than in 2004 to 2007. Additionally, we found that the frequency of meniscal repair during ACL reconstruction varied geographically throughout the United States, with more meniscal repairs being performed in the Southwest region.
The literature suggests that the incidence of meniscal tears with concomitant ACL injury is approximately 55% to 65%.11–13,19,25,38,39 The incidence of meniscal repair in this study was 16%. The number of meniscal repairs reported to the ABOS database falls well short of the overall incidence of meniscal tears with concomitant ACL injuries. Not all tears may have been recognized or were repairable. The surgeon is advised to inspect all regions of the meniscus to confirm absence of a meniscal tear. This may sometimes warrant the establishment of accessory portals. A recent analysis has shown that 85% of ACL reconstructions are done by surgeons who perform fewer than 10 ACL reconstructions per year. 16 However, we did not find a difference in the rate of meniscal repairs between surgeons who performed fewer than 5 ACL reconstructions per year (15% of 2289 cases) compared with surgeons who performed more than 26 ACL reconstructions per year (15.8% of 336 cases; P > .05). From this database, it is unknown if the reported meniscal tears were deemed repairable, or if the injury was in the avascular region of the meniscus. It is possible that a percentage of the tears in this study was too chronic or in the avascular zone, and therefore correctly considered incapable of healing.3,4,18 Another unknown variable is that the surgeon may have decided to leave the meniscal tear in situ. Certain tears, especially small incomplete tears of the lateral meniscus, have been found to be capable of healing if left in situ. 37
There are also economic implications in the question of why meniscectomy is still more commonly performed than meniscal repair. Based on calculations from an urban academic medical center (University of Pittsburgh Medical Center), the current reimbursement rate per Medicare standards is $882 for CPT code 29888 (ACL reconstruction). Each additional procedure is reimbursed with 50% of its relative value unit. Therefore, concomitant coding of 29882 (meniscal repair) reimburses with an additional $304 versus 29881 (meniscectomy) at $281. The resultant net gain of $23 for meniscal repair has to be carefully weighed against increased time for the procedure and additional implant cost (up to $330 for all-inside devices).
Performing traditional open arthroscopic-assisted meniscal repair (inside-out or outside-in technique)17,33,41 is also associated with several risks. An additional incision needs to be made. This bears additional risk of possible nerve damage or blood vessel damage, as well as more possible wound complications. In this study, there was no increased incidence of neurovascular injury; however, there was a higher incidence of wound dehiscence after combined ACL reconstruction and meniscal repair.
An alternative to open meniscal repair is the all-inside repair, which bears its own risk factors but can be performed in a more timely fashion and without additional incisions. Healing with first-generation all-inside devices is reported to be inferior to traditional open meniscal repair and complications such as articular cartilage damage and implant failure have been reported.20,21,32 However, good clinical outcomes have been shown with newer devices in level IV studies. 8 The database of the ABOS does not specify the type of repair performed nor the size, location, or chronicity of the meniscal lesion. Therefore, no conclusions can be made with respect to the use of all-inside devices or traditional open repairs.
Although this study was not designed to give information on ultimate clinical outcome of patients after ACL reconstruction and meniscal surgery, it can be assumed that the majority of patients treated with partial meniscectomy will have increased peak contact pressures in their respective meniscectomized compartments and progressive posttraumatic arthritis.5,6,27 It is therefore recommended to perform meniscal repair in combined ACL tears with meniscal injury whenever possible. This statement is further supported by increased meniscal healing rates in combined injuries when compared with isolated meniscal tears.7,11,31 Tenuta and Arciero 40 described improved healing rates when treating younger patients with acute injuries and a rim width of less than 3 mm.
This study has the advantage of not having been based on surveys but rather utilizing certified data from young orthopaedic surgeons who are sitting for part II of the ABOS certification process. However, given that the data that were used for this study are self-reported for a high-stakes process, one has to interpret the results of this study carefully. One has to acknowledge the young age of surgeons, potential inexperience, and self-report nature of the data as limitations.
Limitations of this study also include the lack of information on the type, location, and chronicity of meniscal tears, as well as what type of repair was performed. Furthermore, there is no information on long-term clinical outcome. In the future, prospective clinical studies are needed to answer these questions.
In summary, we found that combined ACL reconstruction with meniscal repair is more frequently performed for younger patients and when surgery is performed by a sports fellowship–trained surgeon. There has not been a consistent increase in meniscal repairs over time. Although these are encouraging data, concomitant meniscal repair is performed by fellowship-trained surgeons in only 18% of the reported cases of ACL reconstruction. This number is approximately half that of meniscectomies and warrants further investigation.